Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
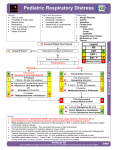
CROUP Prepared by: South West Education Committee Croup Protocol South West Education Committee OBJECTIVES Identify the anatomical differences in pediatrics which impact croup patients. Review of pediatric assessment Identify common presentations for croup. Distinguish croup from Epliglottitis. Describe the treatment for croup. Explain the indications for treatment. ANATOMICAL DIFFERENCES Anatomy is smaller and proportioned differently. Head proportionately larger on a weak neck. Obligatory nose breathers. (Infants) AIRWAY - Pediatric vs. Adult Narrower at all levels The mandible is proportionally smaller in young children The tongue is proportionally larger than adults Larynx is more anterior and superior than an adults’ (C3C4) AIRWAY - Pediatric vs. Adult AIRWAY Cricoid ring is the narrowest part of the airway in young children Tracheal cartilage is softer Trachea is smaller in both length and diameter A Picture is Worth….. Small, hypotonic jaw, large tongue, tonsils, adenoids, arytenoids, uvula, long floppy epiglottis. (prone to swelling) Excessive secretions. (requires suctioning) Gums are more delicate, bleed easily, softer teeth which dislodge easily Anatomical Differences Why is this difficult? The larynx: – 3-3-2 – More anterior. – More superior. thyromental distance – Big teeth or no teeth. – Cone shaped. AIRWAY BLS first – Open & maintain a/w – Ensure patency • Suction & insert oral &/or nasal a/w – ORAL or NASAL ETT? – Assist/prep for intubation HUMAN ERROR Most preventable deaths that happen in the pre-hospital care setting are STILL attributed to poor airway management practices. It has been found that upwards of 86% of preventable deaths of inhospital patients with airway complications were attributed to human error. PEDIATRIC REVIEW CHEST AND LUNGS Ribs are positioned horizontally Ribs are more pliable and offer less protection to organs Chest muscles are immature and fatigue easily Lung tissue is more fragile Mediastinum is more mobile Thin chest wall allows for easily transmitted breath sounds PEDIATRIC REVIEW ABDOMEN Immature abdominal muscles offer less protection Abdominal organs are closer together Liver and spleen are proportionally larger and more vascular PEDIATRIC REVIEW RESPIRATORY SYSTEM Tidal volume is proportionally smaller to that of adolescents and adults Metabolic oxygen requirements of infants and children are about double those of adolescents and adults Children have proportionally smaller functional residual capacity, and therefore proportionally smaller oxygen reserves PEDIATRIC REVIEW CARDIOVASCULAR SYSTEM Cardiac output is rate dependent in infants and small children Vigorous but limited cardiovascular reserve Bradycardia is a response to hypoxia Children can maintain blood pressure longer than adults Circulating blood volume is proportionally larger than adults Absolute blood volume is smaller than adults WRAP UP! Smaller chest and respiratory reserve, belly breathers. Poorly developed accessory and abdominal muscles. ( prone to fatigue / injury) Poorly developed rib cage. (prone injury) Excessive air swallowing. (large stomach) Poor gastric emptying. (vomit) Immature temperature regulatory system. Higher metabolic rate requires a higher respiratory and circulatory rate. Conversely they have a much lower blood pressure due to the lack of plaque, arteriosclerosis and muscle development in arteries. ASSESSMENT PEDIATRICS SCENE ASSESSMENT Observe the scene for hazards or potential hazards Observe the scene for mechanism of injury/illness – Ingestion • Pills, medicine bottles, household chemicals, etc. – Child abuse • Injury and history do not coincide, bruises not where they should be for mechanism of injury, etc. – Position patient found INITIAL ASSESSMENT General impression – General impression of environment – General impression of parent/guardian and child interaction – General impression of the patient/pediatric assessment triangle • A structure for assessing the pediatric patient • Focuses on the most valuable information for pediatric patients • Used to ascertain if any life-threatening condition exists • Components GCS / LOA Determine level of consciousness – AVPU scale • Alert • Responds to verbal stimuli • Responds to painful stimuli • Unresponsive – Modified Glasgow Coma Scale – Signs of inadequate oxygenation Pediatric Glasgow Coma Scale 0-1 year old >1 year old Score Eye Opening Spontaneous To shout To pain No response spontaneous To command To pain No response 4 3 2 1 Verbal Cry, smiles, coos Cries Inappropriate cry Grunts No response Appropriate words Disorientated Cries/screams or inappropriate Grunts or incomprehensible No response 5 4 3 2 1 Localizes pain Withdraws Flexion Extension None Obeys Command Localizes pain Withdraws Flexion Extension None 6 5 4 3 2 1 Motor AIRWAY AND BREATHING Airway – determine patency Breathing should proceed with adequate chest rise and fall. Visualize/Expose chest. Signs of respiratory distress – – – – – – – – – Tachypnea Use of accessory muscles Nasal flaring Grunting Bradypnea Irregular breathing pattern Head bobbing Absent breath sounds Abnormal breath sounds CIRCULATION Pulse – Central – Peripheral – Quality of pulse Blood pressure – 2 x Age + 80 = systolic – 2/3 the systolic = diastolic Skin color Active hemorrhage TRANSITION PHASE Used to allow the infant or child to become familiar with you and your equipment Use depends on the seriousness of the patient's condition – For the conscious, non-acutely ill child – For the unconscious, acutely ill child do not perform the transition phase but proceed directly to treatment and transport APPROACH TO PEDIATRICS Always remember there are 2 patients. Stay CALM, reassure parents and child. – remain calm but be attentive and willing to act aggressively to reduce morbidity and mortality. Handle child gently & explain before doing. Try to examine small children on parents lap when appropriate. If child or parents are extremis to the point they endanger resuscitation efforts, separate. Prevent heat stress and preserve Child’s body heat. PATIENT COMMUNICATION Try to never be alone with a pediatric patient. Sit close, eye level, but do not overcrowd. Use toys to aid your exam. Demonstrate on parents. Offer rewards. Be direct, do not lie!!!!!!! Parents sometimes feel guilty even if they did nothing wrong. HISTORY TAKING Parents of chronically ill children know the disease better than most care givers - ask them. Ask if child has had a fever / are they hot. Hx of laboured breathing or excessive drooling. Lethargy. (A very quiet child is a scary thing) Blank staring, twitching other bizarre behavior. Poor appetite, refusal to eat, vomiting or diarrhea recently. Increase or decrease in wet diapers. Inconsolable crying / screaming does not recognize parents. FOCUSED HISTORY– CONTENT Chief complaint – Nature of illness/injury – How long has the patient been sick/injured – Presence of fever – Effects on behavior – Bowel/urine habits – Vomiting/diarrhea – Frequency of urination Past medical history – Infant or child under the care of a physician – Chronic illnesses – Medications – Allergies DETAILED PHYSICAL EXAMINATION Should proceed from head-to-toe in older children Should proceed from toe-to-head in younger children (less than 2 years of age) Depending on the patient’s condition, some or all of the following assessments may be appropriate: – Pupils – Capillary refill – ECG monitoring Is patient hypoglycemic? - Hydration - Pulse oximetry ON-GOING ASSESSMENT Appropriate for all patients Should be continued throughout the patient care encounter Purpose is to monitor the patient for changes in: – – – – Respiratory effort Skin color and temperature Mental status Vital signs (including pulse oximetry measurements) Measurement tools should be appropriate for size of child RESPIRATORY COMPROMISE Several conditions manifest chiefly as respiratory distress in children including: – Upper and lower foreign body airway obstruction – Upper airway disease (croup, bacterial tracheitis, and epiglottitis) – Lower airway disease (asthma, bronchiolitis, and pneumonia) Most cardiac arrests in children are secondary to respiratory insufficiency thus, respiratory emergencies require rapid prehospital assessment and management CROUP Laryngotracheobronchitis Common inflammatory respiratory illness in children – Viral infection of the upper airway Differentiation between croup and epiglottitis in the prehospital setting may be difficult Upper Respiratory Distress CROUP – upper airway infection with “barking” cough. – mild to moderate respiratory distress with predominant stridor. – may be relieved by cold air. (mist) – usually 2 - 7 years of age, Rapid onset. Epiglottitis DEADLY EMERGENCY!!!!! • • • • • • Rarely have Stridor. (inspiratory when they do) Excessive drooling. Absence of a “barking seal cough.”. Preference for sitting in “sniffing position.” Very “eerie”, quiet & obtunded look. High grade fever. Upper Respiratory Distress PRESENTATION Onset Fever Sore Throat Fear, Anxiety Pale/Cyanosis Drooling Cough Stridor Voice Pref. Position CROUP EPIGLOTTITIS Sudden Gradual Slight/absent High Variable Prominent Variable Prominent Variable Usually Not usual YES “Barking” No Barking cough Inspiration Rare Very hoarse Muffled Variable “Sniffing position” CROUP PROTOCOL INDICATIONS Any patient who is <8 years old . A current Hx of upper respiratory infection. Barking cough (seal-like) Stridor at rest and/or Altered level of consciousness and/or Cyanosis. PROCEDURE Monitor heart rate Attach cardiac monitor Assess pulse rate. Pulse rate must be <200 bpm. PROCEDURE Nebulized Epinephrine will not exceed 2 doses. WHY EPINEPHRINE? Epi. acts on the subglottic swollen area to vasoconstrict blood vessels and reduce the swelling with the alpha 1 effects. Salbutamol has no vasoconstrictive effects and only acts on the smooth muscles of the bronchioles with its beta 2 effects. PROCEDURE Allow patient to assume position of comfort. Reassure the patient and parents. Administer 100% oxygen, via blow-by if needed, while preparing equipment PROCEDURE Nebulize Epinephrine 1:1000 based on patients weight and age. EPINEPHRINE DOSING Age and Weight Dose <1y/o and <5kg 0.5 mg(0.5 ml) in 2 ml of normal saline. <1y/o and >5kg 2.5 mg(2.5 ml) 2 ml of normal saline may be added. >1y/o and <8y/o 5.0 mg (5.0 ml) REPEAT Repeat treatment if no improvement is observed. Max Epinephrine treatments is 2! No exceptions. TRANSPORT ALL PATIENTS MUST BE TRANSPORTED WITHOUT DELAY. REASSESS - ENROUTE Reassess every 5 minutes. Airway Breathing Circulation Vitals And document it all. QUESTIONS?