Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
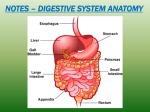
Digestion: breakdown of food molecules for use by the cell Food is broken down by the digestive system into a form that can diffuse directly through the wall of the digestive tract and into the blood Made of digestive tract (muscular tube) and accessory organs (salivary glands, gallbladder, liver, & pancreas) Functions: 1) Ingestion: taking food into the mouth 2) Mechanical mixing: physical manipulation of solid foods by tongue, teeth, & muscles of tract 3) Digestion: chemical breakdown of food into smaller molecules 4) Secretion: release of water, acids, enzymes, and buffers 5) Absorption: movement of small organic molecules, electrolytes, vitamins, & water across the digestive epithelium & into the interstitial fluid 6) Excretion: waste products (indigestible substances & worn out cells) are compacted and discharged by defecation Histology -lining is made of 4 major layers that secrete, contract, contain blood vessels, & protect the rest of the body against enzymes, acids, & bacteria 1) Mucosa: inner lining -epithelium covering a layer of loose connective tissue (lamina propria) -folded to increase surface area, form villi (fingerlike projections) in small intestine -areas of mechanical stress (mouth esophagus, & anus) have stratified epithelium, rest has simple columnar epithelium -lamina propria contains secretory cells -outer layer contains thin muscle that contracts to move villi and folds 2) Submucosa: second layer of loose connective tissue -large blood vessels, lymph vessels, & nerves 3) Muscularis externa: smooth muscle arranged in circular & longitudinal layers -peristalsis: contractions that move contents thru tract -segmentation: regions of small intestine that churn materials to continue mechanical breakdown & mix secretions 4) Serosa: outer layer, serous membrane -none in mouth, esophagus, & rectum (covered by dense collagen fibers (adventitia) that attach these to surrounding structures) -peritoneum: lines cavities -mesentary: parietal & visceral peritoneum that suspends tract to stabilize organs & prevent tangling/injury Oral Cavity: part that receives food 1) analyzes material 2) mechanically processes material 3) lubricates material 4) begins digestion of lipids & carbohydrates with salivary enzymes -anterior boundaries = cheeks & labia (lips) -vestibule: space between cheeks/lips & teeth -gingivae: gums that surround teeth base -superior boundary = hard & soft palates -inferior = tongue -lingual frenulum: fold that connects anterior tongue to underlying tissues -posterior = base of tongue & uvula The Tongue Tongue: manipulate food inside the mouth -Functions 1) mechanical processing by compression, abrasion, & distortion 2) manipulate to help chewing & swallowing 3) sensory analysis by touch, taste, & temperature receptors Salivary Glands -3 pairs 1) Parotid salivary glands 2) sublingual salivary glands 3) Submandibular salivary glands -produce 1 – 1.5 liters of saliva daily -made of 99.4% water with ions, buffers, waste products, metabolites, & enzymes -lubricates & dissolves chemicals to stimulate taste buds when eating -mucus reduces friction when swallowing -continuous production flushes oral cavity & produces immunoglobulins & lysozymes to kill bacteria -production failure would cause infection & erosion of teeth & gums Secretions -salivary amylase: produced by parotid, breaks down starch -other gland products contain less enzymes but more buffers & mucus -max. production is 7ml/minute -submandibular produces 70% of volume -normal pH = 6.7, shifts to 7.5 during eating Teeth Mastication: chewing -breaks down tough connective tissue & plant fibers -helps disperse saliva (mucus & enzymes) PARTS 1. Neck: boundary between root & crown 2. Root: part surrounded by bone 3. Crown: exposed section -covered by enamel: crystalline form of calcium phosphate (hardest biologically made substance) -requires adequate calcium, phosphates, & Vitamin D in diet for complete coating & decay resistance 4. Dentin: mineralized matrix that makes up most of tooth -does not contain living cells 5. Pulp cavity: central area -cells extend into dentin -receives blood vessels & nerves through root canal 6. Alveolus: socket in bone where root extends 7. Periodontal ligament: collagen fibers that connect root dentin to bone 8. Cementum: layer covering root dentin -gives protection & anchors root to periodontal ligament -softer, can be easily eroded if gum disease allows bacterial infection Types of Teeth 1. Incisors: used for clipping/cutting -most anterior 2. Cuspids: Canines, used for tearing & slashing -conical w/ ridgeline & pointed tip 2. Bicuspids (premolars) & Molars: -flattened crowns w/ large ridges -used for crushing, mashing, & grinding Tooth Development Deciduous teeth: first teeth to appear -20 total -periodontal ligaments & roots erode & teeth fall out Secondary teeth: permanent dentition -permit processing of a wider variety of food -32 total -impacted: develop in locations that don’t allow proper eruption Pharynx com -common passageway for food, air, & liquid -food passes thru oropharynx & laryngopharynx -muscles help initiate swallowing Esophagus -muscular tube connecting pharynx & stomach -lies posterior to trachea, passes thru mediastinum & esophageal hiatus: opening in diaphragm -25 cm long, 2cm diameter -lined w/ stratified squamous epithelium for protection & mucous glands to lubricate Deglutition: Swallowing -food must have proper texture & consistency -tongue creates bolus: small mass -takes 9 seconds to complete process -Phases 1) Oral phase: voluntary -bolus compressed against hard palate & is forced into oropharynx while elevating the soft palate 2) Pharyngeal phase: involuntary swallowing reflex -larynx elevates & epiglottis folds to close trachea -pushes bolus thru upper esophageal sphincter into esophagus 3) Esophageal phase: involuntary -bolus pushed thru esophagus to lower esophageal sphincter & into stomach by peristalsis Esophagitis: inflammation of the esophagus due to weak/relaxed esophageal sphincter that allows acid reflex Heartburn: occasional occurrence Hiatal (Diaphragmatic) Hernia: abdominal organs slide into thoracic cavity thru esophageal hiatus -severity depends on location, size, & number of herniated organs -mild condition is common & mostly unnoticed Stomach -muscular, J-shaped organ that receives food from esophagus -4 functions 1) temporary storage of ingested food 2) mechanical breakdown of resistant materials 3) chemical breakdown by acids & enzymes 4) production of intrinsic factor needed for vitamin B12 absorption -chyme: viscous, acidic mixture of partially digested food created in stomach -4 regions 1) cardia: surrounding esophagus opening, smallest 2) fundus: bulge superior to cardia 3) body: large central area 4) pylorus: narrow inferior area, where stomach connects to small intestine at pyloric sphincter: regulates flow of chyme into small intestine -can expand to hold ~1.5 L -muscularis externa is thick & contains longitudinal, circular, & inner oblique layers to add strength & mix/churn contents -rugae: large ridges & folds in mucosa that allow for distension -visceral peritoneum a) greater omentum: extends inferior & creates pouch that hangs over & protects abdominal organs b) lesser omentum: extends from lesser curvature to liver -lined by mucous epithelium that creates a protective alkaline mucous -gastric pits: shallow depressions that open onto gastric surface -end with gastric glands -secrete 1500 ml daily -2 gland types 1) Parietal cells -secrete intrinsic factor: facilitate vitamin B12 absorption across intestinal lining -secretes hydrochloric acid to lower pH to 1.5 – 2 -kills microorganisms, breaks cell walls/connective tissue, & activates enzymatic secretions 2) Chief Cells: -secrete pepsinogen: inactive enzyme, converted into pepsin (proteolytic enzyme) by hydrochloric acid Gastritis: inflammation of the gastric mucosa -causes: drugs, alcohol, aspirin, severe emotional/physical stress, bacterial infection, or ingesting highly acidic/alkaline chemicals Peptic ulcer: acids & enzymes erode thru mucous & stomach lining, or beginning of small intestine -caused by excessive acid production or inadequate alkaline mucous production -bacteria infection causes 80% Phases of gastric regulation 1) Cephalic phase: -begins with sight, smell, taste, or thought of food -prepares stomach -gastric juice production reaches 500 ml/hr 2) Gastric phase: -begins as food reaches stomach -stretch receptors & chemoreceptors cause release of hormone gastrin into blood -causes parietal & chief cells to increase production -may continue for several hours -stomach contracts to churn/mix contents, pylorus contractions squirt small amounts of chyme thru phyloric sphincter 3) Intestinal phase: -controls gastric emptying rate -inhibitory to reduce gastric juices so small intestine has time to deal with & neutralize acidic chyme Digestion in Stomach -preliminary protein digestion -carbohydrates broken down by salivary amylase until pH reaches 4.5 (1-2 hrs) -no absorption occurs -thick mucous layer -epithelial cells not specialized for transport -gastric lining impermeable to water -digestion not complete (protein & carbohydrates only partially digested) Small Intestine -90% of nutrient absorption -6m (20ft) long, diameter 2.5 – 4 cm -3 subdivision 1) Duodenum: 25cm (1ft) long -receives chyme from stomach & secretions from pancreas & liver 2) Jejunum: starts at 1st bend, 2.5m (8ft) -most of chemical digestion & nutrient absorption occurs 3) Ileum: 3.5m (12ft) long -ends at ileocecal valve, sphincter that leads to cecum of large intestine -fits into relatively small space because it’s well-packed & stabilized by mesentaries Intestinal wall -plicae: series of transverse folds -villi: fingerlike projections -covered with simple columnar epithelium & microvilli -folds increase surface area for absorption 611x -capillaries carry respiratory gases & absorbed nutrients to liver -lacteal: lymph vessel in each villus -transport materials that can’t cross into capillaries (e.g. fatty acids) -intestinal glands lie at villi base -secrete watery intestinal juice Intestinal Movements -segmentation mixes chyme w/ secretions & enzymes to prepare for absorption -weak peristaltic contractions move material from duodenum thru ileum in about 5 hours Intestinal juice: 1.8 L secreted into lumen each day -moistens contents, buffers acids, & dissolves enzymes & products of digestion Products -food is broken into simple sugars, fatty acids, & amino acids which are absorbed with most of water Pancreas -elongated, pink/gray organ -15 cm (6 in.) & 80 g (3 oz.) -lumpy texture w/ soft tissue that is easily torn Pancreatic juice: secretion of digestive enzymes & buffers & carried thru ducts that converge at pancreatic duct which funnels juice to duodenum -1000 ml secreted daily -make-up -buffer (sodium bicarbonate) with pH of 7.5 to 8.8 to neutralize chyme -pancreatic amylase: carbohydrates -pancreatic lipase: lipids -nucleases: nucleic acids -proteases: proteins, 70% of total volume -enzymes are secreted as proenzymes, inactive form that are activated by enzymes in the small intestine to protect lining of pancreatic ducts Liver -largest organ, 3.3 lbs, 2.5% of total body weight -essential metabolic & synthetic functions -tough fibrous capsule -4 lobes -large right & left lobes separated by faliciform ligament -smaller caudate & quadrate lobes -Histology -liver lobules: basic functional unit -~100,000 -lined with Kupffer cells: phagocytic macrophages that engulf pathogens, cell debris, & damaged blood cells -as blood flows past, hepatocytes adjust levels by selective absorption (glucose) & secretion -secrete bile (digestive fluid) into common hepatic duct as it leaves -can flow into a. common bile duct: empties into duodenum b. common cystic duct: leads to gallbladder Liver Functions -more than 200 identified 1) Metabolic regulation -regulated composition of circulatory blood -after absorption in intestines blood travels to liver a. extracts toxins & metabolic wastes that will be inactivated/excreted b. monitor & adjust organic nutrient levels -remove & store excess, synthesize or release deficiencies e.g. blood sugar-breaks down glycogen blood sugar-absorbs glucose & builds glycogen -fat-soluble vitamins (A, D, K, & E) absorbed & stored 2) Hematological regulation -largest blood reservoir (25% of cardiac output) -Kupffer cells “clean” blood -synthesize plasma proteins for osmotic control, nutrient transport, & clotting systems 3) Bile Production -water, ions, bilirubin (pigment derived from hemoglobin breakdown), cholesterol, & bile salts (lipids) -water & ions dilute & buffer acids -bile salts emulsify (create tiny drops) lipids that aren’t water-soluble & normally form large blobs that are difficult to breakdown -increase surface area to allow lipases to digest fats Gallbladder -pear-shaped muscular organ that stores & modified bile -nestled under right lobe of liver -liver produces 1L of bile daily, sphincter to common bile duct remains closed until chyme reaches duodenum -most bile travels to gallbladder via cystic duct -can hold 40-70 ml -during storage bile loses water & becomes more concentrated (if too much water is lost, bile salts precipitate out forming gallstones) -wall contractions push bile into duodenum - fat content in chyme bile secretions Large Intestine -runs from end of ileum to anus -main functions 1) water reabsorption & feces compaction 2) absorption of vitamins released by bacterial action 3) storage of fecal material for defecation -1.5m (5 ft) long & 3 in diameter -3 parts 1) Cecum: expanded chamber where contents enter from ileum thru ileocecal valve -veriform appendix: small thin pouch attached to inferior area -contains lymph tissue -can become infected if bacteria become trapped & divide rapidly 2) Colon: 4 regions, dominated by haustra: pouches that permit distension & elongation -3 longitudinal muscle (taeniae coli) help bunch to create haustra -regions a) ascending colon: from ileocecal valve to bend b) transverse colon: horizontal region c) descending colon: inferior to bend d) sigmoid colon: S-shaped, empties into rectum 3) Rectum: end of digestive tract -ends with anal canal -boundary between simple columnar & stratified squamous tissues -anus: anal canal opening of keratinized skin -internal anal sphincter: involuntary, -external anal sphincter: voluntary Large Intestine Functions 1) Absorption -1500ml of material passes thru ileocecal sphincter daily -1300ml of water is recovered, 200ml of feces are defecated -fecal content -75% water -5% bacteria -20% indigestible material, inorganic matter, & dead cells a) bile salts-reabsorbed & transported to liver for re-use b) vitamins-organic molecules needed to metabolic reactions (many assist enzymes) -generated by bacteria 1. Vitamin K-needed by liver to create clotting factors, bacteria produce 50% of daily requirement 2. Biotin-glucose metabolism 3. Vitamin B5-pantothenic acid, help produce steroid hormones & some neurotransmitters c) Bilirubin products-bacteria convert into products that can be excreted in urine (create yellow color), or others stay & turn brown when exposed to oxygen d) Toxins-peptide breakdown creates ammonia, nitrogen-containing compounds (most odor), hydrogen sulfide, many are removed by liver & excreted by kidneys -Indigestible carbohydrates provide food source for bacteria 2) Defecation: forcing feces out the sigmoid colon -defecation reflex: -stretch receptors trigger peristalsis in colon & rectum to move feces toward anus -increases peristalsis throughout large intestine -removal requires internal sphincter to relax, which immediately causes the external sphincter to shut until conscious control opens it