Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
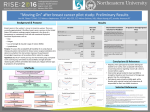
Impact of Under-insurance on Patients with Breast Cancer Related Lymphedema National Congress on the Un and Under Insured Impact of Being Uninsured or Underinsured Individuals with Cancer December 11th, 2007 Ya-Chen Tina Shih, Ph.D. Associate Professor Section of Health Services Research Department Biostatistics Division of Quantitative Sciences University of Texas MD Anderson Cancer Center 1 Breast Cancer Related Lymphedema (BCRL) Upper extremity lymphedema (persistent arm swelling) is one of the most dreaded sequelae of breast cancer treatment BCRL affects 15-30% of breast cancer pts Risk factors of BCRL – – – – – Axillary node dissection Axillary radiation therapy Mastectomy High body mass index Chemotherapy 2 Clinical Management of BCRL No cure for BCRL to date, the mainstay of treatment is symptom control Clinical management includes – – – – – Compression therapy Massage therapy Use of elastic garment or pneumatic pumps Manual lymph drainage … Complications of BCRL – Lymphangitis and cellulites – Other infections The distressing symptoms of lymphedema has caused some patients to describe this condition as “worse than cancer” 3 Coverage of BCRL Treatments Under Women’s Health and Cancer Rights Act (WHCRA) of 1998, group health plans, insurance companies and HMOs offering mastectomy coverage also must provide coverage for certain services relating to the mastectomy, including lymphedema Not all states passed state laws conforming to the lymphedema treatment provision of the WHCRA As of Dec 31, 2006, only 21 states required private insurance to provide coverage for lymphedema treatment incident to breast 4 cancer State Laws Mandated Private Insurance to Cover BCRL Treatment in 1998 - 2004 1998 2004 N=1 N=21 Source: NCI, State Cancer Legislative Database 5 Study Objective and Hypothesis Objective: to compare total health care costs between BCRL patients in states with versus without coverage mandate (i.e., the under-insured states) Hypothesis: the under-insured states will incur lower costs in the short run but higher costs in the long run due to a higher rate of costly complications 6 Data: MarketScan HPM, 1997-2003 MarketScan®: nationwide employment-based claims data – Insurance claims from over 100 payers from 45 large employers – Medical and outpatient prescription drug claims – Include: employees, spouses, and dependents Health and Productivity Management (HPM) – Productivity information (time lost from work) for a subset of employees – Include: work loss due to absence, short-term 7 disability, or workers’ compensation Study Sample and Measures Inclusion: – lymphedema ICD-9 codes: 457.0; 457.1 – BC-related codes • • • • Two or more claims on different dates with BC DX One or more claim indicate BC-related surgery (i.e., mastectomy or lumpectomy) Two or more claims for non-surgical definitive treatment (i.e., chemo or radiation) Two or more RX claims for tamoxifen or aromatase inhibitors (AIs) Exclusion: – Duration of continuous enrollment < 12 months Calculation of BCRL-related costs – Collect all claims for the study sample identified above – Excluded claims related to BC treatment • • • • • • Surgery: mastectomy, lumpectomy Radiation Chemotherapy Prescriptions of tamoxifen or AIs Supportive care due to cancer treatment Tests to determine staging – Excluded claims related to routine screening and/or testing 8 Descriptive Statistics Age: mean 49.5 ; SD=8.15 Relationship with employers – employee – spouse (48%) (52%) 138 200 218 76 2 (21.8%) (31.5%) (34.4%) (12.0%) (0.3%) Regions – – – – – 306 328 Northeast Northcentral South West Unknown Sample size variations by duration of continuous enrollment – One-year – Two-year – Three-year N = 634 N = 447 N = 278 9 Comparisons of Total Costs of BCRL Patients by State Coverage 0 – 12 months Sample size Rate of cellulitis or lymphangitis Difference Out-of-pocket pay Difference 0 – 24 months Not covered Covered Not covered Covered Not covered Covered 504 130 438 92 383 64 11.9% 10.8% 16.2% 8.7% 18.0% 10.9% P=0.72 Total payment 0 – 18 months $24,103 $25,147 -$1,044 (P=0.01) $1,460 $1,521 -$62 (P=0.01) P=0.07 $32,020 $30,280 $1,740 (P=0.006) $2,833 $2,195 $638 (P=0.02) P=0.16 $38,878 $33,164 $5,714 (P=0.031) $3,279 $2,537 $743 (P=0.03) Note: Costs in this table include treatment costs related to breast cancer; 2 test was used to compared the rate of cellulitis 10 between groups; Mann-Whitney two-sample test was used to compare costs between groups Cost Comparison by State Coverage $20,000 $16,000 $12,000 $8,000 $4,000 $0 YR1 covered Total YR1 not covered RX YR2 covered Inpatient Note: Costs excluded claims possibly related to breast cancer treatment Outpatient YR2 not covered 11 Cost Comparison by State Coverage $16,000 $12,000 $8,000 $4,000 $0 YR1 covered Total YR1 not covered RX YR2 covered Inpatient Note: Costs excluded claims possibly related to breast cancer treatment Outpatient YR2 not covered 12 Cost Comparison by State Coverage $20,000 $16,000 $12,000 $8,000 $4,000 $0 YR1 covered Total YR1 not covered RX YR2 covered Inpatient Note: Costs excluded claims possibly related to breast cancer treatment Outpatient YR2 not covered 13 Discussion and Conclusion Compared with BCRL patients in the under-insured states, those resided in the covered states had – Similar rate of complication in the first 12 months, but lower rate in the first 18 and 24 months – Higher total costs in the first 12 months, but significantly lower costs in the first 18 and 24 months – Slightly higher out-of-pocket payment in the first 12 months, but significantly lower OOP in the first 18 and 24 months – In year 2: lower total costs, and much lower inpatient costs Findings confirmed our hypothesis that BCRL patients resided in the under-insured states incur higher longterm costs from poorly managed lymphedema Exploratory need a larger sample size to confirm!! 14 Acknowledgement Funding Source: American Cancer Society Collaborators – – – – – – – HSR/Epidemiology: Linda S. Elting, DrPH Surgical oncology: Janice N. Cormier, MD, MPH Breast medical oncology: Sharon H. Giordano, MD Radiation oncology: Thomas A. Buchholze, MD Radiation oncology: George Perkins, MD HSR/Stat analyst: Ying Xu, MD, MS Nursing, Vanderbilt Univ.: Sheila H. Ridner, PhD, RN 15