Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiac surgery wikipedia , lookup
Jatene procedure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
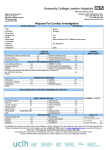
12 Lead-ACS Fleming College Paramedic Program Focus of ACS Common reason for transport Much can be done during transfer Reduce risk of morbidity and mortality The first step = recognizing the ACS Signs and symptoms ECG changes Biochemical changes Summary Strategies for reducing morbidity and mortality Reduce cardiac workload Improve perfusion to cardiac tissue Reduce risk of fatal arrhythmias Reduce extension of clot formation Reperfuse the ischemic myocardium Myocardial Infarction ASA (2 x 80 mg) P.O. O2 therapy IV access NTG via SL, transdermal, and/or IV Morphine Heparin and/or Beta blockers 12 Lead ECG as soon as possible Pre-hospital Thrombolysis Air Ambulance-Ornge Oshawa Land ALS Positive empirical trends Pre-hospital Thrombolysis prolonged transport time no thrombolysis at the sending facility Long delays Indications - Thrombolysis Ischemic Less C.P. than 12 hours duration Ischemic Chest Pain? O - at rest or with exertion P – better or worse Q - heaviness, tightening, sharp, weakness etc R - neck, jaw and/or left arm S - varies T - consistent, does NOT come & go 12 Lead ECG Criteria ST segment elevation New onset Left Bundle Branch Block with S&S? Some acute coronary syndromes (A.C.S.) do not benefit from thrombolysis LBBB-FYI ONLY! Cannot reliably diagnose AMI in the setting of a LBBB Collaborative data (history, enzymes etc.) in the setting of a new LBBB is an indication for thrombolysis What are the Benefits? Varies between subgroups of patients Time to thrombolysis “Infarct to Drug Time” shorter the better the outcome Its all about Timing Thrombolytics within one hour of onset of CP - 50% reduction in infarct size Thrombolytics within two hour of onset of CP - 30% reduction in infarct size Thrombolytics within 3-4 hour of onset of CP - 13% reduction in infarct size TIME IS MUSCLE - after 6-12 hours less helpful Examples of Thrombolytics Retaplase Tenectoplase (TNK) Streptokinase Tissue plasmingen activator (TPA) Absolute Contraindications for Thrombolytics Aortic dissection Active (significant) bleeding Pericarditis Relative Contraindications CPR >10 minutes Pregnancy Uncompressible puncture site (from IV etc) Age (>75) Recent surgery or trauma or stroke (>2 wks) Current use of warfarin or other anticoagulant Aortic Dissection How to not get fooled CP radiating into back Tearing vs pressure Unequal pulses or blood pressures in limbs Neurological symptoms Hypertension ++ (or low if they are leaking) CXR Things to do BEFORE Thrombolysis Venipunctures CXR Blood analysis INR, aPTT, CBC etc. Explain risk/benefits to patient Pericarditis How not to get fooled? Non-specific CP - sometimes severe ST segment elevation (ah..ha! But where?) Pericarditis How to not get fooled Atypical ischemic CP Sitting forward can decrease discomfort Fever or systemic illness Younger without cardiac risk factors ST elevation is diffuse, no anatomical pattern Serial ECG’s Active Bleeding Non-compressible site(s) most common are GI and GU More Relative Contraindications The grey area intracranial/intraspinal surgery intracranial neoplasm, A-V malformation, aneurysm bleeding diathesis severe hypertension What is the Risk? Intracranial hemorrhage Overall rate - 0.9% Varies considerably between patients What is the Risk? Baseline risk w/o RF - 0.75% 2-3% up to 5% in anterior As low as 1% in inferior What is the Risk? Age > 65 add 0.5% Add another 0.5% > 75 y.o. >80 y.o. >85 y.o. What is the Risk? SBP > 160 add 0.5% SBP > 180 add another 0.5% Weight < 70 kg add 0.5% Any previous stroke add 2-4% In the right patient the risk is significant All stroke risks!! Other Treatment Options ASA Heparin Beta Blockers IIB/IIIA inhibitors Primary PTCA Best option in patients with increased risk or in patients with limited benefit Potential for ambulances close to these centers (tertiary care centres) e.g Peterborough, Kingston, toronto, Ottawa Percutaneous Transcoronary Angiography (PTCA) Success Approx. 70% of patients regain patency of the vessel Pain relief Reduction in ST segment deviation Arrhythmia's Access Specialty procedure Rescue angioplasty (fast transfers!!) high risk for thrombolytics Rx thrombolytics failed to correct the problem Post Thrombolytic Care Watch for reperfusion arrhythmias Usually benign Usually transient Watch for signs of bleeding Watch for signs of bleeding! Now to the 12 lead bit…. Introduction to 12 Lead ECG Diagnostic 12 lead is performed to rule in/out various pathologies Standard limb leads (I,II,III) Augmented vector leads (aVL,aVR, aVF) Precordial or chest leads The Importance of a 12 lead EKG Many calls involve the CVS 12 lead ECG is a useful tool in the cardiac assessment. What Can be Assessed on the 12 lead EKG? Axis Bundle branch conduction Hypertrophy Fascicular conduction Ischemia/Injury/Infarction patterns Pericarditis Electrolyte disturbances Drug intoxication AND MUCH MUCH MORE!!!!! Required Skills to Interpret the 12 lead EKG Comprehension of electrophysiology electrolyte and cellular functions during normal and abnormal de/repolarization Advanced knowledge of cardiac pathophysiology Recognizing normal versus abnormal Ability to follow an organized and sequential approach LOTS AND LOTS OF PRACTICE!!!!! Fundamentals of 12 Lead Interpretation Review of cardiac conduction Refresh the understanding of the anatomy and physiology applicable to EKG interpretation Cardiac Conduction Sinoatrial node Right atrium Near superior vena cava Depolarizing the atria through intranodal tracts Cardiac Conduction Atrioventricul ar node Right atrium Near the septum Mediates conduction to the ventricles Cardiac Conduction Bundle of His Originates in the AVN Left and right branches Spreads action potential throughout ventricles 12 Lead EKG - Limb Leads Lead I Lead II Right arm to left arm Left positive Right arm to Left leg Left leg positive Lead III Left arm to Left leg Left leg positive 12 Lead EKG - Limb Leads Bipolar leads form Einthoven’s triangle Reference points are the lead origins This is important ! 12 Lead EKG - Augmented Leads Augmented lead right (aVR) Origin point to the right Augmented lead left (aVL) Origin point to the left Augmented lead foot (aVF) Origin point downward 12 Lead EKG - Augmented Leads Unipolar leads form Goldberger’s triangle Origin point is the heart This is an important reference! A tip: imagine this triangle within the Einthoven’s triangle! The 6 Limb Leads I 0° II +60 ° III +120 ° aVL -30 ° aVR -150 ° aVF +90 ° What Part of the Heart? Frontal plane leads look at different segments of the heart Know what area the leads focus on Relationship Leads II, III and aVF view the inferior wall Leads I and aVL view the lateral wall Lead aVR is not helpful here Purpose of the 12 Lead Identify ST elevation/depression T wave inversion Identify VT in wide complex rhythms Electrical axis and hypertrophy Bundle branch blocks Indications? Ischemic chest pain (unstable angina) Chest pain – NYD Change in chest pain presentation To rule out cardiac involvement Rule of Thumb Perform a 12-lead when considering differential diagnoses It It It It could could could could be be be be angina an MI an aneurysm pericarditis Don’t do it unless you are prepared (or someone else is) to act on the result! Precordial Leads - 12 Lead Precordial Leads - How are they placed? V1 - 4th intercostal space, R sternal border V2 - 4th intercostal space, L sternal border V4 - 5th intercostal space, midclavicular line V3 - between V2 and V4 V6 - 5th intercostal space, midaxillary line V5 – anterior axillary line between V4 and V6 The 6 Chest Leads 12 Lead ECG - LP 12 Attach limb leads as per normal Attach precordial leads to multi-lead adapter Attach to patient as per prior diagram Press ’12 lead’ button DON’T TOUCH PATIENT DURING NEXT 20-30 SECS. ASK PATIENT NOT TO MOVE Receive 12 lead from Printer 12 Lead ECG Each of the 12 leads views the left ventricle from the positive electrode In the precordial leads, it is assumed this is in the center of the heart Review 12 lead information in Bledsoe Myocardial Infarction The BIG ONE! Lead Perspective Lead I and aVL = lateral wall Lead II, III and aVF = inferior wall aVR is not helpful here V1 and V2 = anterior-septal wall V3 and V4 = anterior wall V5 and V6 = lateral wall ST Segment Deviation ST segment is typically isoelectric ST segment represents total ventricular depolarization ST segment changes are caused by cellular changes Causes of ST segment changes During ischemia the resting membrane potential is lowered relative ST segment elevation Asynchronous depolarization of multiple cardiac cells true ST segment elevation Criteria for Cardiac Injury on the EKG Transmural cardiac injury Limb ST segment elevation of 1mm and extending at least 2mm out from the J point Precordial ST segment elevation of 2mm Other findings may include Inverted or flipped T waves Pathological Q waves Phases of an Acute MI Hyper acute phase - ST segment elevation begins in the first hours and may last 1-6 weeks Evolved phase - deep T waves and onset of pathological Q waves Resolution phase - T waves return to normal morphology and position Chronic phase - pathological Q waves How can we determine the affected vessels? The left coronary artery bifurcates into two primary branches circumflex artery left anterior descending Determining the Affected Vessels? The right coronary artery right atria & ventricle inferior wall of the left ventricle 2/3 of the posterior wall How can we determine the affected vessels? Observe the vessel mapping! Knowledge Application! Is there any ST segment deviation? What leads are affected? What area do these leads look at? Reciprocal Changes ST changes opposite from the anatomical location of the injured region ‘mirror-like’ image ST segment depression is reciprocal to ST elevation Investigate further to rule out/in injury pattern Practice! Differential Diagnosis - ST Segment Elevation Acute myocarditis Hyperkalemia Hypothermia Acute cor pulmonale Cerebrovascular hemorrhage Cardiac tumor Even occasionally in healthy individuals!!! Ischemia Electrophysiology - Ischemia Cells quickly lose O2 and nutrient supply CO2 removal is impeded Unable to completely repolarize ECG depressed ST segment and/or inverted T waves T waves = ventricular repolarization ST depression of 2mm or greater = pathology Other Multi-lead ECG Configurations 15 lead ECG and 18 lead ECG Right Side EKG To provide a more specific look at the right ventricle Leave V1 in place - this becomes V2R Leave V2 in place - this becomes V1R Move V4 to the 5th ICS on the right midclavicular line = V4R Move V3 halfway between V2R and V4R = V3R Move V5 to the right anterior axillary line in the 5th ICS = V5R Move V6 to the right midaxillary line = V6R Posterior EKG To provide a closer look at the posterior wall of the heart Move 3 precordial leads to the same horizontal plane as V5 & V6 Be sure to note which leads you have repositioned Position them at the bottom of the left shoulder blade left of the vertebral column Utility of a 12 Lead ECG It is only as good as the interpretation Treat the patient first! Start with the basics - O2, NTG, MS, IV etc. Closely monitoring patients with suspected ACS Practice Practice Google it! Buy a book Try it on everyone in EMERG with chest pain! Volunteer