Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
1) Title of study project : - Comparison of Efficacy of Bromocriptine mesylate and
Pioglatazone in Type 2 Diabetes Patients: A Randomized Controlled clinical trial.
2) Location of study : SMT KASHIBAI NAVALE MEDICAL COLLEGE AND GENERAL
HOSPITAL, NARHE, PUNE
Department / Institution : DEPARTMENT OF MEDICINE AND PHARMACOLOGY
3) Name(s) & signature(s) of the Principal investigator(s) :
DR. RADHA YEGNANARAYAN, DR. YOGENDRA KECHE
Designation & Department
PROFESSOR AND HEAD,
LECTURER,
DEPARTMENT OF PHARMACOLOGY, SKMNC & GH
4) Name(s) & signature(s) of the co-investigator(s) :
Designation & Department:
DR. Y. D. SINGH
PROFESSOR
DEPARMENT OF MEDICNE, SKNMC & GH
DR. J. SASTRY
HEAD, DEPARTMENT OF CLINICAL RESEARCH
5) Approval of the Head(s) of the Department(s) undertaking the study :
Name(s) & Signature
1) DR RADHA YEGNANARAYAN
PROFESSOR AND HEAD, DEPARTMENT OF PHARMACOLOGY, SKMNC & GH
2) DR BABAN SANAS
PROFESSOR AND HEAD, DEPARTMENT OF MEDICNE, SKMNC & GH
3) DR D. P. GHADAGE
PROFESSOR AND HEAD, CENTRAL CLINICAL LABORATORY, SKMNC & GH
6) Duration of study: 1 year
7) Deadlines for periodic progress review & data analysis : 3 months
8) Detailed Research Plan :
This study will start after approval from Ethics Committee of Smt Kashibai Navale Medical
College and General Hospital in department of Medicine and Department of Pharmacology. Patients
of Type 2 Diabetes on Sulphonylureas/ Metformin not responding adequately and having Hb1Ac >
8% will be recruited from Medicine OPD with the help of physician. Patients will be given
information about the drugs including adverse effect (See Annexure VII). A written informed
consent {See Annexure IV} will be taken from each patient and those who will be willing to
participate in study will be enrolled .All the information will be written in case report form{See
Annexure V}. There will be two groups of patients, out of which one group will receive
bromocriptine (Bromocriptine Group) and other group will be given pioglitazone (Pioglitazone
Group ). Patients will be maintained on the same Sulfonylureas / Metformin doses as before.
Bromocriptine will be given in the dose starting from 1.25 mg to 4.375 mg (MAXIMUM) along
with Sulfonylureas / Metformin therapy. Bromociptine tablet 1.25 mg (1 tablet) daily will be given
in first week, followed by 2.5 mg (2 tablets) in 2nd week, later 3.75 mg (3 tablets) in 3rd week and
lastly 4.375 mg (31/2 tablets ) if tolerated by patient. The patient will be asked to take the tablet
within 2 hours after waking from sleep with some food. Maximum tolerated dose is kept constant
for the period of 6 months. This dose used in this study is different from quick release formulation.
This particular dose is chosen in this study as dose of bromocriptine quick release formulation for
antidiabetic effect is 0.8 mg to 4.8 mg (increased gradually), another aspect is that in India quick
release formulation is not available hence have to use conventional formulation that is available as
1.25mg oral tablet.The other group (Pioglitazone Group) will be maintained on pioglitazone therapy
in their maximum tolerated doses started from 15 mg daily to maximum dose of 45 mg31 for period
of six months At baseline all the investigations will be carried out as follows:
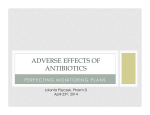
STUDY DESIGN FLOW CHART
ENROLLMENT OF PATIENTS ON SULFONYLUREAS /
METFORMIN AND Hb1Ac > 8 %
BASELINE INVESTIGATIONS &
RANDOM ALLOACTION IN TWO GROUPS OF PATIENTS.
BROMOCRIPTINE
THERAPY STARTED
PIOGLITAZONE
THERAPY STARTED
FOLLOW UPS AT 1,2,3
AND 6 MONTHS
FOLLOW UPS AT 1,2,3
AND 6 MONTHS
INVESTIGATIONS FLOW CHART
Both the Groups (Bromocriptine and Pioglitazone)
Baseline
Blood sugar-Fasting/PP, Serum lipid profile, HbA1c level, Serum insulin, Body weight, height,
Blood pressure,(These investigations will be carried out to to measure the effect of Bromocriptine
and Pioglitazone) Blood urea, Serum creatinine, Serum Bilirubin, SGOT,SGPT, Alkaline
phoshatase, Hb % and CBC (These Investigations will be carried out to rule out hepatic or renal
dysfunction ), ECG (To rule out cardiac abnormality viz, IHD, arrhythmias)
1month
Blood sugar-Fasting/PP, Hb1Ac, Serum insulin, LFT, Hb % and CBC, Body weight, Blood pressure
2 months
Blood sugar-Fasting/PP, Hb1Ac, Serum insulin, LFT, Hb % and CBC, Body weight, Blood
pressure
3 months
Blood sugar-Fasting/PP. Serum lipid profile, HbA1c level, Serum insulin, LFT, Hb % and CBC,
Body weight, Blood pressure
6 months
Blood sugar-Fasting/PP. Serum lipid profile, HbA1c level, Serum insulin, LFT, Hb % and CBC,
Body weight, Blood pressure
Inclusion Criteria:
1.Age between 30 -70 years
2.Sex: Male/ Non-lactating female
3.HbA1 > 8
4.Type 2 Diabetic patient on Sulphonylureas/ Metformin not responding adequately
Exclusion Criteria:
1. Age < 30 yrs.
2. Pregnancy
3. Lactating mother
4. Patient with Insulin dependent Diabetes Mellites
5. Patient who is taking oral antidiabetic drugs other than Sulphonyureas and Metformin
6. Severe and Complicated diabetes
7. Patient with IHD
8. Patients having renal or hepatic dysfunction
9. Patient of Parkinsonism, syncopal migraine
10. Patient who is taking - Salicylates, Sulfonamides, Chloramphenicol, Probenecid, Phenithiazines,
Butyrophenones, Thioxanthenes,Metoclopramide
11. Strong Inhibitors/Inducers/ Substrates of CYP 3A4
Inhibitors -sodium valproate, erythromycin, Fluroquinolones except ofloxacin, verapamil,
diltiazem,
propoxyphene,
allopurinol,
MAO
inhibitors,
disulfiram,
tolbutamide,
metronidazole,captopril, enalpril, carbidopa
Inducers :Phenobarbitone, phenytoin, carbamazepine, ethanol, clofibrate, griseofulvin,
Rifampcin, pyridoxine
Substrates:
barbiturates,
dextropropoxyphene,
warfarin,theophylline,
paracetamol,
ascorbic
acid,
tolbutamide, diazepam, vit D, oral contraceptives, antidepressants,
quinidine, terfanidine,phenytion, carbamazepine, morphine, pethidine,
12. HIV positive patients
After enrollment of patient for study, all the baseline investigations will be carried out at Central
Clinical Laboratory except Hb1Ac which will be carried out at department of Pharmacology. ECG,
Blood pressure recording will be carried out in Department of Medicine.
Reporting of Adverse effects:
All patients will be given checklist of Adverse effect of Bromocriptine (Annexure VI
) as well as Pioglitazone(Annexure VIII ). Information of ADR will be taken in next follow-up. If
patients are unable to tolerate ADR, they are advised to contact any of investigators at any time.
Contact numbers of investigators will be mentioned on patient information sheet. ADRs will be
treated according to gradations of ADRs of Common Terminology Criteria for Adverse Events
(CTCAE) Version 4.0 (NIH)36. Only severe ADRs will be reported to respective company and
DCGI in standard format. Treatment ADRs will be done according to grades of ADRs.
Investigational drug use will be stopped if grade of ADR is 3 or more than 3. Alternative drug
therapy will be made available to patient who has got ADRs due to investigational drug.
General Guidelines for grading as well as treatment of ADRs are as below:
Grade 1 : Mild; asymptomatic or mild symptoms; clinical or diagnostic observations only;
intervention not indicated.
Grade 2 : Moderate; minimal, local or noninvasive intervention indicated; limiting age-appropriate
instrumental ADL*.
Grade 3 : Severe or medically significant but not immediately life-threatening.
hospitalization or prolongation of hospitalization indicated; disabling; limiting self care ADL**.
Grade 4 : Life-threatening consequences; urgent intervention indicated.
Grade 5 : Death related to AE.
Activities of Daily Living (ADL)
*Instrumental ADL refer to preparing meals, shopping for groceries or clothes, using the telephone,
managing money, etc.
**Self care ADL refer to bathing, dressing and undressing, feeding self, using the toilet, taking
medications, and not bedridden.
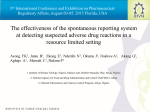
Expected ADRs of Bromocriptine:7,12,31
Nausea, fatigue, dizziness, vomiting and headache
Grading of ADRs to Bromocriptine:36
Bromocriptine
Grades of ADRs
1
Symptom/ADR
Nausea
Fatigue
2
3
Loss of
Oral intake
appetite
decreased
Inadequate oral
without
without
caloric or fluid
alteration in
significant
intake; tube
eating
weight loss,
feeding, TPN, or
habits
dehydration or
hospitalization
malnutrition
indicated
Fatigue not
Fatigue not
Fatigue
relieved by rest;
relieved by rest,
relieved by
limiting
limiting self care
rest
instrumental
ADL
4
5
ADL
Mild
Dizziness
Moderate
Severe
unsteadiness unsteadiness or
unsteadiness or
or sensation
sensation of
sensation of
of
movement;
movement;
movement
limiting
limiting
instrumental
self care ADL
ADL
1-2
Vomiting
episodes
3 - 5 episodes
>=6 episodes
Life-
(separated
(separated by 5
(separated by 5
threatening
by 5
minutes) in 24
minutes) in 24
consequences;
minutes) in
hrs
hrs; tube feeding,
urgent
TPN or
intervention
hospitalization
indicated
24 hrs
Death
indicated
Moderate pain;
Headache
Mild pain
limiting
Severe pain;
instrumental
limiting self care
ADL
ADL
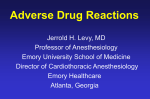
Expected ADRs of Pioglitazone :31
Anaemia, weight gain, edema, and plasma volume expansion, hepatotoxicity, macular edema31
Grading of ADRs to Pioglitazone:36
Pioglitazone
Grades of ADRs
1
Symptom/ADR
2
3
4
Hgb <8.0
Hemoglobin
Anemia
Weight gain
Death
g/dL; <4.9
Life-threatening
(Hgb) <LLN -
Hgb <10.0 - 8.0
mmol/L;
consequences;
10.0
g/dL; <6.2 - 4.9
<80 g/L;
urgent
g/dL; <LLN - 6.2
mmol/L; <100 -
transfusion
intervention
mmol/L; <LLN -
80g/L
indicated
indicated
5 - <10% from
10 - <20% from
>=20% from
baseline
baseline
baseline
100 g/L
5
Edema face
Moderate
Severe
Localized facial
localized facial
swelling;
edema
edema; limiting
limiting self
instrumental
care ADL
ADL
>10 - 30% interlimb
discrepancy in
Edema limbs
volume or
>30% inter-
circumference at
limb
point of
discrepancy
5 - 10% inter-
greatest visible
in
limb discrepancy
difference;
volume;
in volume or
readily apparent
gross
circumference at
obscuration of
deviation
point of greatest
anatomic
from
visible
architecture;
normal
difference;
obliteration of
anatomic
swelling or
skin folds;
contour;
obscuration of
readily
limiting self
anatomic
apparent
care ADL
architecture on
deviation from
close inspection
normal
anatomic
contour; limiting
instrumental
ADL
Symptomatic
Death
liver
dysfunction;
Hepatotoxicity
fibrosis by
Decompensated
biopsy;
liver function
Asymptomatic,
compensated
(e.g., ascites,
treatment not
cirrhosis;
coagulopathy,
indicated
reactivation
encephalopathy,
of chronic
coma
hepatitis
Optic disc
Decreased
visual acuity
(worse than
Blindness
20/40);
(20/200 or worse)
marked
visual field
defect
but sparing
the central 20
degrees
Decreased visual
acuity
(20/40 or better);
visual
field defect
Asymptomatic
edema
present
Expected ADRs of Sulfonylureas: Nausea, vomiting, hypoglycemia, cholestatic jaundice,
Hypersensitivity reaction. Grading for ADRs like agranucytosis, aplastic anemia, hemolytic anemia
not available.CBC and Hb % will be done at each follow up and these ADRs will be graded on the
basis of general guidelines for grading of ADRs.
Grades of ADRs of Sulfonylureas:
Sulfonylureas
Grades of ADRs
1
Symptom/ADR
Nausea
2
3
Loss of appetite
Oral intake
Inadequate oral
without
decreased without
caloric or fluid
alteration in
significant weight
intake; tube
eating habits
loss,
feeding, TPN, or
dehydration or
hospitalization
4 5
malnutrition
Vomiting
Hypoglycemia
indicated
>=6 episodes
Life-
(separated by 5
threatening
3 - 5 episodes
minutes) in 24
consequences;
1 - 2 episodes
(separated by 5
hrs; tube feeding, urgent
(separated by 5
minutes) in 24 hrs
TPN or
intervention
minutes) in 24
hospitalization
indicated
hrs
indicated
<LLN - 55
mg/dL; <LLN 3.0
mmol/L
<55 - 40 mg/dL;
<3.0 - 2.2
mmol/L
<40 - 30 mg/dL;
<2.2 - 1.7
mmol/
Death
<30 mg/dL;
Death
<1.7 mmol/L;
lifethreatening
consequences;
seizures
Symptomatic
Death
liver
Cholestatic
dysfunction;
Decompensat
jaundice
fibrosis by
ed liver
biopsy;
function
Asymptomatic,
compensated
(e.g., ascites,
treatment not
cirrhosis;
coagulopathy,
indicated
reactivation of
encephalopath
chronic
y, coma
hepatitis
Hypersensitiviy Transient
Intervention or
Prolonged (e.g.,
Life-
flushing or rash,
infusion
not rapidly
threatening
drug
interruption
responsive to
consequences;
fever <38 degrees indicated; responds
symptomatic
urgent
C (<100.4
promptly to
medication
intervention
degrees F);
symptomatic
and/or brief
indicated
Death
intervention not
treatment (e.g.,
interruption of
indicated
antihistamines,
infusion);
NSAIDS,
recurrence of
narcotics);
symptoms
prophylactic
following initial
medications
improvement;
indicated for <=24
hospitalization
hrs
indicated for
clinical sequelae
(e.g., renal
impairment,
pulmonary
infiltrates)
Expected ADRs of Metformin : Nausea, Diarrhea, Indigestion, Abdominal cramps/bloating,
Lactic acidosis
Grades of ADRs of Metformin: Grading for ADRs like deficiency of Vit B12, lactic acidosis,
Indigstion, Abdominal bloating not available.CBC and Hb % will be done at each follow up and
these ADRs will be graded on the basis of general guidelines for grading of ADRs.
Sulfonylureas
Grades of ADRs
1
Symptom/ADR
2
3
Oral intake
Nausea
decreased
Inadequate oral
Loss of appetite
without
caloric or fluid
without
significant
intake; tube
alteration in
weight loss,
feeding, TPN, or
eating habits
dehydration
hospitalization
or
indicated
malnutrition
4
5
Increase of >=7
Death
stools per day
over baseline;
incontinence;
Increase of 4 - hospitalization
Diarrhea
6 stools per
indicated;
Increase of <4
day
severe
stools per day
over baseline;
increase in
over baseline;
moderate
ostomy output
Life-threatening
mild increase in
increase in
compared to
consequences;
ostomy output
ostomy output baseline;
compared to
baseline
compared to limiting
baseline
self care ADL
urgent
intervention
indicated
Sample Size Calculation and statistical analysis:
Sample size of 30 for each group is calculated in the ratio of 1, power 80 %,
considering 10 fold difference of drug effect in bromocriptine group and control group by using
OpenEpi software. Randomization of study population will be carried out with help of
randomization number table.
9) Justification for study :
Newer therapeutic approach to treat Type II Diabetes with Bromocriptine will improve glycemic
control as well as may be helpful in improving lipid profile as well as reducing body weight.
Pioglitazone has following drawbacks :1) it has variable effect on lipid profile 2) Caution should
be exercised while prescribing in hepatic disorders and heart failure patients as it causes plasma
volume expansion 3) risk of developing bladder cancer. Due to these drawbacks pioglitazone, need
is there to search alternative to pioglitazone. Bromocriptine is time tested drug for indications like
Parkinson’s disease and hyperprolactenemia and recently in May 2009, approved for type 2 diabetes
in USA. Bromocriptine causes only mild ADRs like nausea, vomiting, fatgue, giddiness, headache.
Caution to be exercised in patients with syncope and hypotension. Bromocriptine use not associated
with increased cardiovascular risk, infact it is found to reduce cardiovascular risk in type 2 diabetic
patients and has beneficial effect over cardiovascular function. In this context, bromocriptine has
beneficial features and can be used as alternative to pioglitazone in treatement of type 2 diabetes
wherever pioglitazone can not be used due ADRs and limitations in form of cautions for using in
hepatic dysfunction and heart failure.
10) Funding :
SMT KASHIBAI NAVALE MEDICAL COLLEGE AND HOSPITAL
Source of funding / Sponser
Sanction letter from authorities
11) Whether informed consent of study subject is required ?
12) If study involves drug intervention
Availability of drug
YES
- Central Pharmacy, SKNNMC & GH Pune -41
Source of procurement of drug
13) If new drug / formulation :
Permission letter from DCGI
- required
14) Date of submission for ethical review -
15) Remarks of the secretary:
Date:
Names & Signature of
Principal Investigators
Names(s) & Signature of
Co-investigators
Dr. Radha Yegnanarayan
Dr. Y. D. Singh
Dr. Yogendra Keche
Dr. J. Sastry
Prof & Head of the Department