Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
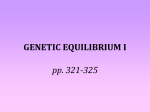
Vagal modulation of heart rate during exercise: effects of age and physical fitness MIKKO P. TULPPO,1,2 TIMO H. MÄKIKALLIO,1,2 TAPIO SEPPÄNEN,1 RAIJA T. LAUKKANEN,2 AND HEIKKI V. HUIKURI1 1Department of Medicine, Division of Cardiology, University of Oulu, 90220 Oulu; and 2Merikoski Rehabilitation and Research Center, 90100 Oulu, Finland cardiovascular regulation; Poincaré plot MEASUREMENT OF HEART RATE (HR) variability has become a widely used tool for assessing the autonomic input to the heart under various physiological conditions (4–7, 15, 18). Previous research has suggested that autonomic modulation of HR is influenced by certain physiological factors such as aging and physical fitness. Studies of HR variability have demonstrated a decline in the vagal modulation of HR at rest at an advanced age (15, 18, 25), but there is little evidence regarding the extent to which these age-associated changes depend on the simultaneous decline in aerobic capacity. Although HR variability has been commonly observed to be related to physical fitness (5–7, 13), there is also some controversy regarding this issue (4, 14). In previous studies HR variability has been measured in standardized supine or upright positions or during routine daily activities, but because the cardiovascular system at rest or in different postures functions at only a fraction of its capacity, results obtained H424 at rest may not completely characterize this system or its regulatory mechanisms. Relatively little information is available on the effects of physiological factors on cardiovascular autonomic function during exercise. Experimental studies (1, 19, 23) have shown that vagal control of HR plays an important cardioprotective role during exercise. Therefore, it would be important to know whether certain physiological factors have influence on cardiac vagal function during the course of physical exercise. The present cross-sectional study was designed to examine the association of aerobic fitness and aging on vagal modulation of HR during exercise in a random population of healthy males. METHODS Subjects. The subjects were recruited by placing a notice in a newspaper, which attracted 210 replies. The subjects were interviewed with a standardized scheme to ascertain their medical histories and levels of physical activity. All smokers, subjects with high body mass index (.27), and those with diabetes mellitus or cardiovascular disorders were excluded. We invited 130 subjects to our laboratory for a more specific assessment of physical status and excluded 13 subjects on account of various relative contraindications for the maximal exercise test. We tested 117 subjects and excluded 7 from the final analysis because of the number of artifacts or ectopic beats in data acquisition. Finally, 110 male subjects (age 41 6 11 yr) were included in the analysis. The population was divided into tertiles according to age and aerobic fitness. The different age tertiles were matched for fitness, and the different aerobic fitness tertiles were matched for age (Tables 1 and 2). The protocol was approved by the ethics committee of the Merikoski Rehabilitation and Research Center, and all subjects gave informed consent. Protocol. Measurements of HR variability and oxygen consumption were made on all the subjects at rest and during incremental exercise on a bicycle ergometer. The subjects were not allowed to eat or drink coffee for 4 h before the test, and vigorous exercise and alcohol were forbidden for 48 h before the day of testing. All the tests were performed between 8:00 AM and 2:00 PM. The subjects stayed in a supine position in a quiet room for 30 min, after which R-R intervals (30 min) and blood pressure were measured in a supine position. The R-R intervals for the last 2 min of each load were analyzed during the exercise test. Twelve of the subjects repeated the test protocol four times (with four days of recovery in between) to ascertain the reproducibility of the measurement of HR variability at rest and during exercise. Measurement of peak O2 consumption. The subjects performed a graded maximal exercise test on a bicycle ergometer (Ergomedic 818 E, Monark Exercise, Varberg, Sweden), starting at 25 W and following a ramp protocol with the work rate increasing at a rate of 25 W every 3 min until voluntary exhaustion. Ventilation (VE), gas exchange (M909 ergospirometer, Medikro, Kuopio, Finland), and HR responses (Polar 0363-6135/98 $5.00 Copyright r 1998 the American Physiological Society Downloaded from ajpheart.physiology.org on October 20, 2009 Tulppo, Mikko P., Timo H. Mäkikallio, Tapio Seppänen, Raija T. Laukkanen, and Heikki V. Huikuri. Vagal modulation of heart rate during exercise: effects of age and physical fitness. Am. J. Physiol. 274 (Heart Circ. Physiol. 43): H424–H429, 1998.—This study was designed to assess the effects of age and physical fitness on vagal modulation of heart rate (HR) during exercise by analyzing the instantaneous R-R interval variability from Poincaré plots (SD1) at rest and at different phases of a bicycle exercise test in a population of healthy males. SD1 normalized for the average R-R interval (SD1n ), a measure of vagal activity, was compared at rest and during exercise among subjects of ages 24–34 (young, n 5 25), 35–46 (middle-aged, n 5 30), and 47–64 yr (old, n 5 25) matched for peak O2 consumption (V̇O2 peak) and among subjects with V̇O2 peak of 28–37 (poor, n 5 25), 38–45 (average, n 5 36), and 46–60 ml · kg21 · min21 (good, n 5 25) matched for age. SD1n was higher at rest in the young subjects than in the middle-aged or old subjects (39 6 14, 27 6 16, and 21 6 8, respectively; P , 0.001), but the age-related differences in SD1n were smaller during exercise [e.g., 11 6 5, 9 6 5, and 8 6 4 at the level of 100 W; P 5 not significant (NS)]. The age-matched subjects with good, average, and poor V̇O2 peak showed no difference in SD1n at rest (32 6 17, 28 6 13, and 26 6 11, respectively; P 5 NS), but SD1n differed significantly among the groups from a low to a moderate exercise intensity level (e.g., 13 6 6, 10 6 5, and 6 6 3 for good, average, and poor fitness groups, respectively; P , 0.001, 100 W). These data show that poor physical fitness is associated with an impairment of cardiac vagal function during exercise, whereas aging itself results in more evident impairment of vagal function at rest. HEART RATE VARIABILITY AND FITNESS Table 1. Characteristics of subjects at different fitness-matched age tertiles Young Old 25 29 6 3 24–34 180 6 6 82 6 7 16 6 4 30 40 6 3a 35–46 178 6 5 81 6 7 18 6 3 25 53 6 4b,c 47–64 177 6 6 79 6 9 15 6 4 123 6 11 80 6 8 3.5 6 0.5 122 6 11 78 6 8 3.3 6 0.4 122 6 8 82 6 7 3.2 6 0.5 42 6 5 41 6 4 41 6 6 32–51 34–50 32–54 191 6 8 182 6 9a 170 6 13b,c 8.0 6 0.9 8.0 6 1.5 7.2 6 1.4 Values are means 6 SD except for ranges. V̇O2peak , peak O2 consumption. a P , 0.001, young vs. middle-aged; b P , 0.001, young vs. old; and c P , 0.001, middle-aged vs. old, according to analysis of variance followed by post hoc analysis (unpaired t-tests) between groups. a frequency of 1,000 Hz (17) and saved in a computer for further analysis of HR variability with Heart Signal software (Kempele, Finland). The R-R interval series was passed through a filter that eliminates undesirable premature beats and noise. An R-R interval was interpreted as a premature beat if it deviated from the previous qualified interval by .30%. All the R-R intervals were edited automatically, and then by visual inspection, to exclude all the undesirable beats, which accounted for ,1% in every subject. The details of this analysis and the filtering technique have been described previously (9, 10). An autoregressive model was used to estimate the power spectrum densities of R-R interval variability (9, 10). The high-frequency (HF; 0.15–0.40 Hz) component of power spectral analysis (HF power) was calculated as the square root of HF power and then divided by mean R-R interval [coefficient of component variance (CCV%)] (8). The Poincaré plot is a diagram (scattergram) in which each R-R interval of a tachogram is plotted as a function of the previous R-R interval. The Poincaré plots were analyzed quantitatively. This quantitative method of analysis is based on the notion of different temporal effects of changes in the vagal and sympathetic modulation of the HR on the subsequent R-R intervals without a requirement for a stationary quality of the data (22). The computerized analysis entails fitting an ellipse to the plot, with its center coinciding with Sport Tester, Polar Electro, Kempele, Finland) were monitored continuously during the ramp protocol. VE and gas exchange were calculated on a breath-by-breath basis but were reported as mean values for 30 s. A fingertip venous blood sample was taken 2 min after the exercise to analyze venous blood lactate (YSI 1500 Sport, YSI, Yellow Springs, OH). The highest value of oxygen consumption measured during the test was used as peak oxygen consumption (V̇O2peak) (16). Measurement and analysis of HR variability. The R-R intervals were recorded (Polar R-R Recorder, Polar Electro) at Table 2. Characteristics of subjects at different age-matched fitness tertiles Poor n Age, yr Age range, yr Height, cm Weight, kg Fat, % Blood pressure, mmHg Systolic Diastolic V̇O2peak , l/min V̇O2peak , ml · kg21 · min21 V̇O2peak range, ml · kg21 · min21 Maximal heart rate, beats/min Maximal lactate, mmol/l Average Good 25 43 6 10 27–56 178 6 7 83 6 8 18 6 4 36 40 6 9 27–54 179 6 5 81 6 7 17 6 3 25 40 6 9 29–56 178 6 4 78 6 7 14 6 4d,f 126 6 12 84 6 9 2.8 6 0.3 123 6 10 79 6 9a 3.3 6 0.3b 122 6 8 79 6 6c 4.0 6 0.3e,g 34 6 3 41 6 2b 51 6 4e,g 28–37 38–45 46–60 180 6 15 183 6 12 181 6 10 7.7 6 1.6 8.0 6 1.3 7.9 6 1.5 Values are means 6 SD except for ranges. , 0.05 and b P , 0.001: poor vs. average; c P , 0.05, d P , 0.01, and e P , 0.001: poor vs. good; f P , 0.05 and g P , 0.001: average vs. good, according to analysis of variance followed by post hoc analysis (unpaired t-tests) between groups. aP Fig. 1. Two-dimensional (2-D) vector analyses of Poincaré plots for 2 subjects. A: subject with good aerobic fitness (age 5 35 yr, V̇O2 peak 5 45 ml · kg21 · min21 ) at rest and during exercise (100 W). B: subject with poor aerobic fitness (age 5 29 yr, V̇O2 peak 5 34 ml · kg21 · min21 ) at rest and during exercise. A: example of 2-D vector analysis of a Poincaré plot in subject at rest. Standard deviation of instantaneous beat-to-beat R-R interval variability (SD1) is short diameter of ellipse (axis 1), and standard deviation of continuous R-R interval variability (SD2) is long diameter (axis 2). SD1 is almost identical in these 2 subjects at rest (left) but is significantly higher in subject with good aerobic fitness during exercise (right). HR, average heart rate. Each R-R interval (R-Rn 1 1 ) is plotted as a function of previous R-R interval (R-Rn ). Downloaded from ajpheart.physiology.org on October 20, 2009 n Age, yr Age range, yr Height, cm Weight, kg Fat, % Blood pressure, mmHg Systolic Diastolic V̇O2peak , l/min V̇O2peak , ml · kg21 · min21 V̇O2peak range, ml · kg21 · min21 Maximal heart rate, beats/min Maximal lactate, mmol/l Middle Aged H425 H426 HEART RATE VARIABILITY AND FITNESS RESULTS Age and vagal modulation of HR. The mean HR and mean values for SD1n and HF power in the young, middle-aged, and old age groups during exercise are shown in Fig. 2. The individual values for SD1n at rest and at the level of 100 W are shown in Fig. 3A. HR did not differ among the three age groups at rest (59 6 8, 58 6 7, and 56 6 8 beats/min for young, middle-aged, and old subject groups, respectively) but was lower in the old than in the younger subjects at the submaximal and maximal exercise levels (Fig. 2A). Two-dimensional vector analysis of the Poincaré plots showed the mean values for SD1n (Fig. 3A) and SD2n (116 6 29 vs. 80 6 21; P , 0.001) to be significantly higher in the younger than in the older subjects at rest as well as during exercise up to an exercise intensity of 75 W (Fig. 2B). The mean value of the HF power (32 6 12 vs. 17 6 7 CCV%; P , 0.001) was significantly higher in the younger than in the older subjects at rest as well as during exercise up to an exercise intensity of 75 W (Fig. 2C). SD1 decreased progressively to 1.79 6 0.32, 1.74 6 0.32, and 1.70 6 0.35 l/min in the young, middle-aged, and old subject groups, respectively, during the graded exercise (P 5 NS). Fitness and vagal modulation of HR. The mean HR and mean values for SD1n and HF power in the good, Fig. 2. HR (A), 2-D vector analysis of Poincaré plots as indicated by SD1 normalized for average R-R interval (SD1n; B), and highfrequency (HF) power of spectral analysis (HF power) normalized for average R-R interval (CCV%; C) in 3 age groups (fitness-matched) during exercise. Values are means 6 SD. Kruskal-Wallis H-tests were used at each exercise intensity level (among all 3 groups) followed by post hoc analysis (Mann-Whitney U-test) between young group and old group. xx P , 0.01 and xxx P , 0.001 for young group compared with old group. ns, Not significant. average, and poor fitness groups during exercise are shown in Fig. 4. The individual values for SD1n at rest and at a level of 100 W are shown in Fig. 3B. The mean HR was significantly lower in the good than in the poor fitness group at rest (54 6 5 vs. 62 6 7 beats/min; P , 0.001) and during submaximal exercise but not at the end of the exercise (Fig. 4A). SD1n or HF power (27 6 14, 23 6 10, and 22 6 11 CCV% for good, average, and poor fitness groups, respectively) did not differ significantly at rest among the different fitness groups (Fig. 3B). SD1n and HF power during exercise were significantly higher in the good than in the poor fitness group up to the level of 150 W (Figs. 4B and 4C). SD2n did not differ among the three fitness groups at rest, but SD2n during exercise was significantly higher in the good than in the poor fitness group at the levels of 100 and 125 W (P , 0.01). SD1 decreased progressively to Downloaded from ajpheart.physiology.org on October 20, 2009 the center point of the markings (Fig. 1A, left). Axis 2 shows the slope of the longitudinal axis, whereas axis 1 defines the transverse slope, which is perpendicular to axis 2. In the computerized analysis, the Poincaré plot is first turned 45° clockwise, and the standard deviation of the plot data is then computed around the horizontal axis (axis 2), which passes through the data center (SD1). SD1 shows the instantaneous beat-to-beat variability of the data. The standard deviation of continuous long-term R-R intervals is quantified by turning the plot 45° counterclockwise (SD2) and by computing the data points around the horizontal axis (axis 1), which passes through the center of the data. SD1 and SD2 were calculated as absolute values and in normalized units (SD1n and SD2n, respectively), obtained by dividing the absolute value by the average R-R interval and then multiplying by 1,000. Statistical methods. Normal Gaussian distribution of the data was verified by the Kolmogorov-Smirnov goodness-of-fit test. Whenever the data were not normally distributed (Z value .1.0), the Kruskal-Wallis H test was used, followed by post hoc analysis (Mann-Whitney U-test). Otherwise, analysis of variance was used and the differences between the mean values were tested for significance using the unpaired t-test. Reproducibility was estimated according to the recommendations of Bland and Altman (2). This method consists of calculating the means of the repeated measures and the standard deviation of the differences and plotting the difference between the measurements as a function of the mean value for each subject. The smaller the confidence interval of the difference, the better the reproducibility. The Friedman’s randomized-block analysis of variance was used to compare the paired data. The exercise intensity level at which the instantaneous beat-to-beat R-R interval variability (SD1) reached its minimum during the exercise was defined as the first exercise intensity level of two consecutive points at which SD1 decreased by ,1 ms between two exercise intensity levels. HEART RATE VARIABILITY AND FITNESS H427 DISCUSSION There are two new findings in this study. First, middle-aged subjects with good aerobic fitness have enhanced cardiac vagal function during exercise compared with subjects with poor physical fitness. Second, aging itself does not result in significant impairment in vagal function during exercise despite reduction in vagal modulation of HR at rest. Together, these findings may provide insight into the cardioprotective role of physical fitness in middle-aged subjects. Age and vagal modulation of HR. The present results confirm previous observations that aging results in a reduction in respiratory vagal modulation of HR at rest and show that this reduction seems to be independent of any impairment of physical fitness. Less profound age-related differences were observed in instantaneous HR variability in the course of exercise, showing that aging itself entails a less marked impairment of cardiac Downloaded from ajpheart.physiology.org on October 20, 2009 Fig. 3. Individual (s) and mean 6 SD (r) values for SD1n at rest and during exercise (100 W). A: subjects categorized according to age and matched for peak O2 consumption (V̇O2 peak). B: subjects categorized according to aerobic fitness and matched for age. Kruskal-Wallis H-tests were used, followed by post hoc analysis (Mann-Whitney U-test) among groups. xx P , 0.01 and xxx P , 0.001 between groups indicated. 1.90 6 0.28, 1.74 6 0.28, and 1.56 6 0.38 l/min in the good, average, and poor fitness groups, respectively, during the graded exercise, and that point was at a significantly lower O2 consumption level in the poor than in the good fitness group (P , 0.01). Examples of Poincaré plots for subjects with good and poor aerobic fitness are shown in Fig. 1. Reproducibility of Poincaré plot analysis. The differences among 4 measurements of SD1 in the case of 12 subjects are plotted as a function of each subject’s mean value at rest and during exercise in Fig. 5. The confidence interval (95%) of the difference for SD1n was 6 5.3 at rest and decreased during exercise, i.e., 63.3 and 62.2 for 50 and 75 W, respectively. The confidence interval (95%) of the difference for HF power was 6 4.4 at rest and also decreased during exercise, i.e., 6 3.8 and 6 2.2 CCV% for 50 and 75 W, respectively. No significant differences among the days of measurement were found in HF power or in the two-dimensional vector analysis parameters at rest or during exercise. Fig. 4. HR (A), 2-D vector analysis of Poincaré plots (SD1n; B), and HF power (C) in 3 fitness groups (age-matched) during exercise. Values are means 6 SD. Kruskal-Wallis H-tests were used at each exercise intensity level (among all 3 groups) followed by post hoc analysis (Mann-Whitney U-test) between good fitness group and poor fitness group. x P , 0.05, xx P , 0.01, and xxx P , 0.001 for good fitness group compared with poor fitness group. ns, Not significant. H428 HEART RATE VARIABILITY AND FITNESS vagal modulation during physical exercise. The results also confirm previous observations (22, 24) that vagal modulation disappears at the level of 50–60% of maximal O2 consumption, whereafter the increase in HR is mainly mediated by sympathetic activation. The exercise level at which instantaneous R-R interval variability disappeared was not related to age, suggesting that advanced age may not result in adverse sympathovagal balance during physical exercise unless concomitant impairment of aerobic capacity occurs with aging. Physical fitness and vagal modulation of HR. It is widely assumed that good physical fitness and regular exercise training induce adaptation of the autonomic nervous system, which is most commonly observed in the form of a decrease in basal HR at rest. This is thought to be mediated in part by an increase in cardiac vagal tone. Although it is commonly assumed that cardiac vagal tone is increased in well-trained individuals, this is a somewhat controversial matter. Studies (5–7, 13) comparing athletes and age-matched sedentary subjects have mostly observed higher HR variability in trained individuals than in controls, but Lazoglu The authors appreciate the technical and financial support received from Polar Electro (Kempele, Finland) and the generous help Downloaded from ajpheart.physiology.org on October 20, 2009 Fig. 5. Differences among 4 measurements performed on each of 12 subjects as a function of their mean values for SD1 at rest (A), during exercise at an intensity level of 50 W (B), and during exercise at an intensity level of 75 W (C). Horizontal lines indicate mean (solid lines) and 95% confidence intervals (dashed lines) of differences among 4 measurements. et al. (14) did not find significant differences in 24-h HR variability between cyclists and sedentary controls. Controversial results may be due to differences in the baseline characteristics among the study populations and in the methodology of analysis of HR variability. Previous studies may be partly influenced also by differences in life-style habits other than physical fitness itself between well-trained athletes and sedentary control subjects, because a population-based crosssectional study (4) did not observe any significant relationship between maximal O2 consumption and HR variability measured in subjects at supine, seated, or standing postures. The present results in a random population of healthy males also demonstrate that there are no significant differences in HR variability at rest between the subjects with poor and good physical fitness despite significant differences in basal HR. However, subjects with better exercise capacity have significantly higher vagal modulation of HR during exercise than those with poor physical fitness, and the exercise intensity level at which their vagal modulation disappears is also significantly higher, supporting the concept that cardiac vagal function is related to aerobic fitness in middle-aged subjects. Reproducibility of Poincaré plot analysis. HR variability generally has rather poor reproducibility when measured from short-term electrocardiogram recordings at rest (3), because it can potentially be influenced by factors such as the time of day, food intake, mental state, etc., when measurements are repeated on successive days. Exercise causes a marked alteration in autonomic function, with a gradual vagal withdrawal followed by sympathetic activation. The repeated tests performed in the present study showed that the measurement of vagal modulation of HR is more reproducible during exercise than at rest, possibly because the profound effects of the exercise itself on autonomic function minimize the influence of other confounding factors. In conclusion, the main finding of this study, i.e., that physical fitness is related to vagal modulation of HR during exercise independent of aging, provides further evidence that good aerobic fitness has beneficial effects on cardiovascular autonomic function. Experimental data have shown that vagal activity prevents ventricular fibrillation during exercise (1, 19, 23) and that exercise training confers anticipatory protection from sudden death by enhancing cardiovascular autonomic function (12). There is also experimental and clinical evidence that augmented sympathetic outflow is related to arrhythmogenesis and cardiovascular morbidity and mortality (20, 21). Rapid loss of vagal activity followed by sympathetic activation during mild-tomoderate exercise intensity may be one potential mechanism for adverse clinical events, and the present data support the concept that good aerobic fitness may exert cardioprotective effects by enhancing the cardiac vagal function during exercise. HEART RATE VARIABILITY AND FITNESS from Heart Signal (Kempele, Finland). The authors also thank Timo Karppinen for help with the data processing. This research was partly funded by grants from the Finnish Foundation for Cardiovascular Research (Helsinki, Finland) and the Medical Council of the Academy of Finland (Helsinki, Finland). Address for reprint requests: H. V. Huikuri, Dept. of Medicine, Div. of Cardiology, Univ. of Oulu, Kajaanintie 50, 90220 Oulu, Finland. Received 18 February 1997; accepted in final form 24 September 1997. REFERENCES 12. Hull, S. J., Jr., E. Vanoli, P. B. Adamsson, R. L. Verrier, R. D. Foreman, and P. J. Schwartz. Exercise training confers anticipatory protection from sudden death during acute myocardial ischemia. Circulation 89: 548–552, 1994. 13. Katona, P., M. McLean, D. Dighton, and A. Guz. Sympathetic and parasympathetic cardiac control in athletes and nonathletes at rest. J. Appl. Physiol. 82: 1652–1657, 1982. 14. Lazoglu, A. H., B. Glace, G. W. Gleim, and N. L. Coplan. Exercise and heart rate variability. Am. Heart J. 131: 825–827, 1996. 15. Lipsitz, L. A., J. Mietus, G. B. Moody, and A. L. Goldberger. Spectral characteristics of heart rate variability before and during postural tilt: relations to aging and risk of syncope. Circulation 81: 1803–1810, 1990. 16. McArdle, W. D., F. I. Katch, and V. L. Katch. Exercise Physiology: Energy, Nutrition, and Human Performance (3rd ed.). Philadelphia, PA: Lea and Febiger, 1991, p. 211–213. 17. Ruha, A., S. Sallinen, and S. Nissilä. A real-time microprocessor QRS detector system with a 1 ms timing accuracy for the measurement of ambulatory HRV. IEEE Trans. Biomed. Eng. 44: 159–167, 1997. 18. Shannon, D. C., D. W. Carley, and H. Benson. Aging of modulation of heart rate. Am. J. Physiol. 253 (Heart Circ. Physiol. 22): H874–H877, 1987. 19. Schwartz, P. J., G. E. Billman, and H. L. Stone. Autonomic mechanisms in ventricular fibrillation induced by myocardial ischemia during exercise in dogs with healed myocardial infarction. An experimental preparation for sudden cardiac death. Circulation 69: 780–785, 1984. 20. Schwartz, P. J., and S. G. Priori. Sympathetic nervous system and cardiac arrhythmias. In: Cardiac Electrophysiology: From Cell to Bedside, edited by D. P. Zipes and J. Jalife. Philadelphia, PA: Saunders, 1990, p. 330–343. 21. Tsuji, H., M. G. Larson, F. J. Venditti, Jr., E. S. Manders, J. C. Evans, C. L. Feldman, and D. Levy. Impact of reduced heart rate variability on risk for cardiac events: the Framingham heart study. Circulation 94: 2850–2855, 1996. 22. Tulppo, M. P., T. H. Mäkikallio, T. E. S. Takala, T. Seppänen, and H. V. Huikuri. Quantitative beat-to-beat analysis of heart rate dynamics during exercise. Am. J. Physiol. 271 (Heart Circ. Physiol. 40): H244–H252, 1996. 23. Vanoli, E., G. M. De Ferrari, M. Stramba-Badiale, S. S. Hull, R. D. Foreman, and P. J. Schwartz. Vagal stimulation and prevention of sudden death in conscious dogs with a healed myocardial infarction. Circ. Res. 68: 1471–1481, 1991. 24. Yamamoto, Y., R. L. Hughson, and J. C. Peterson. Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J. Appl. Physiol. 71: 1136–1142, 1991. 25. Yoshimitsu, Y., M. Kodama, M. Matsuhisa, M. Kishimoto, H. Ozaki, A. Tani, N. Ueda, Y. Ishida, and T. Kamada. Diurnal heart rate variability in healthy subjects: effects of aging and sex difference. Am. J. Physiol. 271 (Heart Circ. Physiol. 40): H303– H310, 1996. Downloaded from ajpheart.physiology.org on October 20, 2009 1. Billman, G. E., and R. S. Hoskins. Time-series analysis of heart rate variability during submaximal exercise. Evidence for reduced cardiac vagal tone in animals susceptible to ventricular fibrillation. Circulation 80: 146–157, 1989. 2. Bland, J. M., and D. G. Altman. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1: 307–310, 1986. 3. Breuer, H.-W. M., A. Skyschally, M. Wehr, R. Schulz, and G. Heusch. Poor reproducibility of parameters of heart rate variations. Z. Kardiol. 81: 475–481, 1992. 4. Byrne, E. A., J. L. Fleg, P. V. Vaitkevicius, J. Wright, and S. W. Porges. Role of aerobic capacity and body mass index in the age-associated decline in heart rate variability. J. Appl. Physiol. 81: 743–750, 1996. 5. Davy, K. P., N. L. Miniclier, J. A. Taylor, E. T. Stevenson, and D. R. Seals. Elevated heart rate variability in physically active postmenopausal women: a cardioprotective effect? Am. J. Physiol. 271 (Heart Circ. Physiol. 40): H455–H460, 1996. 6. De Meersman, R. E. Heart rate variability and aerobic fitness. Am. Heart J. 125: 726–731, 1993. 7. Goldsmith, R. I., J. T. Bigger, R. C. Steinman, and J. L. Fleiss. Comparison of 24-hour parasympathetic activity in endurance-trained and untrained young men. J. Am. Coll. Cardiol. 20: 552–558, 1992. 8. Hayano, J., Y. Sakakibara, A. Yamada, M. Yamada, S. Mukai, T. Fujinami, K. Yokoyama, Y. Watanabe, and K. Takata. Accuracy of assessment of cardiac vagal tone by heart rate variability in normal subjects. Am. J. Cardiol. 67: 199–204, 1991. 9. Huikuri, H. V., M. K. Linnaluoto, T. Seppänen, K. E. J. Airaksinen, K. M. Kessler, J. T. Takkunen, and R. J. Myerburg. Circadian rhythm of heart rate variability in survivors of cardiac arrest. Am. J. Cardiol. 70: 610–615, 1992. 10. Huikuri, H. V., T. Seppänen, M. J. Koistinen, K. E. J. Airaksinen, M. J. Ikäheimo, A. Castellanos, and R. J. Myerburg. Abnormalities in beat-to-beat dynamics of heart rate before the spontaneous onset of life-threatening ventricular tachyarrhythmias in patients with prior myocardial infarction. Circulation 93: 1836–1844, 1996. 11. Huikuri, H. V., J. O. Valkama, K. E. J. Airaksinen, T. Seppänen, K. M. Kessler, J. T. Takkunen, and R. J. Myerburg. Frequency domain measures of heart rate variability before the onset of nonsustained and sustained ventricular tachycardia in patients with coronary artery disease. Circulation 87: 1220–1228, 1993. H429