Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
CT Anatomy
of
the Female
Pelvis:
A Second
Look1
Mary
C. Foshager,
James
W. Walsh,
MD
MD
Computed
tomography
(CT) remains
a valuable
technique
in the assessment
of the female
pelvis.
The CT appearance
of the normal
ligamentous,
vascular,
and visceral
anatomy
of the female
pelvis
can be
confusing.
Newer
high-resolution
CT scanners
combined
with mechanical
intravenous
contrast
medium
injectors
and thinner
sections
have substantially
improved
the imaging
of female
genital
tract anatomy. In addition
to the cardinal,
uterosacral,
and round
ligaments,
the ovaries
and their ligamentous
attachments,
as well as the blood
supply
to the female
internal
organs,
can now be visualized.
Inferiorto-superior
image
acquisition
following
bolus
administration
of intravenous
contrast
material
with an angiographic
injector
facilitates
precise identification
of the uterine
artery and its relationship
to the
pelvic
ureter
and the vascular
plexus
supplying
the vagina,
ovaries,
and uterine
body.
Ideally,
familiarity
with variations
in the CT appearance of normal
female
pelvic
anatomy
will enable
more
accurate
evaluation
of pelvic
abnormalities.
.
INTRODUCTION
The computed
tomographic
(CT) appearance
of the normal
ligamentous,
vascular,
and visceral
anatomy
of the female
pelvis
can be confusing
unless
one is familiar
with the basic anatomy
of these
structures
and normal
variations
in their appearance.
High-resolution
CT scanners
and techniques
tailored
to examination
of the
pelvis
now permit
detailed
visualization
of the ovaries,
uterus,
and cervix,
as well as
precise
identification
of their ligamentous
attachments
and vascular
supply.
In this
article,
genitalia
Index
we
review
the normal
and discuss
techniques
terms:
Computed
neoplasms.
1994;
the
Received
‘
85. 12 1 18
#{149}
Pelvic
organs.
85. 12 1 18, 85.92
#{149}
Pelvic
organs,
ofDiagnostic
MN
Recipient
February
55455.
12,
1993;
Radiology,
ofa
revision
Cum
requested
University
Laude
ofMinncsota
award
March
for a scientific
26 and
received
Hospital.
exhibit
July
Box
at the
14; accepted
292
UMIIC,
420
1992
RSNA
scientific
July
15. Address
Delaware
St SE.
assembly.
reprint
re-
to M.C.F.
RSNA,
See
thin-section,
of the female
internal
of these
structures.
14:51-66
Department
Minneapolis.
quests
(CT),
and CT appearance
facilitate
visualization
85.32
RadioGraphics
From
tomography
anatomy
that
1994
the commentary
by flattery
et al following
this
article.
51
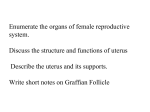
Figure 1. Posterior
view of the female
ligaments
and viscera. Drawing
illustrates the broad,
round,
cardinal,
uterosacral, and
ovarian
ligaments
and their relationships
to the
ovaries,
and
uterus,
pelvic
ureters.
U PATIENT
POPULATION
AND
IMAGING
TECHNIQUES
CT images
were selected
from a review
of 135
pelvic CT examinations
performed
on 125
women
ranging
in age from 22 to 83 years. A
group
of 80 patients
(1 5 with normal
findings
and 65 with abnormal
findings)
and another
group
of 45 patients
(10 with normal
findings
and 35 with abnormal
findings)
underwent
imaging
performed
with two different
scanners. Diagnoses
in the patients
with abnormal
findings
were cancer
of the ovary, endometrium,
52
U
Scientific
Exhibit
cervix,
vagina,
and
vulva.
All images
were
acquired
with
a Somatom
Plus CT scanner
with an Impress
detector
system (Siemens,
Iselin,
NJ) or a GE 9800
Quick
CT scanner
(Milwaukee,
Wis). All studies
utilized a tailored
pelvis
protocol
consisting
of
(a) a bolus
intravenous
injection
of 100-150
mL of 60% iodinated
contrast
material
administered
with an angiographic
injector
at 2 mL/
sec; (b) inferior-to-superior
image
acquisition
with an 8-10-mm
section
thickness
from the
pubis
to the iliac crest,
a 1-second
scan time,
and a 5.0-6.5-second
interscan
delay;
(C) delayed 2-5-mm
sections
through
the pelvic
abnormality
or region
of interest;
and (d) oral
administration
of 750 mL of 2% barium
during the 2 hours
before
the examination
to optimize
colonic
opacification
at image
acquisition.
Volume
14
Number
1
Figure
2.
Axial view of the female
pelvic
viscera
and ligaments
at the level of the uterme body.
Drawing
illustrates
the uterine
body and the ovaries
to the round,
broad,
and their relationships
and ovarian
ligaments.
The purpose
of the tailored
pelvis
protocol
fivefold:
(a) to help differentiate
pelvic
blood vessels
from lymph
nodes
and parametrial
tumor
extension;
(b) to enhance
uterine
myometrium
and epithelium
and delineate
the endometrial
cavity;
(c) to enhance
the
cervical
stroma
and epithelium;
(d) to demarcate tumor
from normal
uterine
and cervical
parenchyma;
and (e) to opacify
the bladder
and pelvic
ureters,
further
delineate
abnor-
edge
is formed
by the fallopian
tube medially
and the suspensory
ligament
of the ovary laterally
(2,4-6).
The lower
margin
of the broad
ligament
ends at the cardinal
ligament
(Fig 1).
malities,
sets, mesonephric
remnants,
and a portion
of
the ureter
(1,2,7,8).
Although
the broad
ligament
is rarely
seen unless
ascites
is present,
was
and
ing on delayed
U
PELVIC
extend
January
thin
partial
volume
averag-
sections.
LIGAMENTS
The broad
peritoneum,
sidewall
eliminate
ligament
is formed
by two layers
of
which
drape
over the uterus
and
laterally
from the uterus
to the pelvic
(Figs 1 , 2) (1-5).
The superior
free
1994
Between
is loose
the
two
leaves
of the
extraperitoneal
broad
connective
ligament
tissue,
smooth
muscle,
and fat known
as the parametrium,
which
contains
the fallopian
tube,
round
ligament,
ovarian
ligament,
uterine
and
ovarian
blood
vessels,
nerves,
lymphatic
yes-
its position
that
it abuts
can
or
be
determined
by structures
contains.
Foshager
and
Walsh
#{149}
RadioGraphics
#{149}
53
i;
a.
Figure
3.
Normal round ligaments.
(a) CT scan
the uterus
(U) and a right ovarian
cyst (0)
shows normal
round ligaments
bilaterally
(black arrows). The left ligament
tapers distally
(small white
arrow),
where it crosses
the left external
iliac artery
and vein anteriorly
(large white arrows).
(b) CT scan
through
an enlarged
uterus
(U) shows fine round
ligaments (small white arrows)
that cross anteriorly
toward the inferior
epigastric
vessels (large white arrow), where the ligaments
enter the internal
inguinal
ring. The necrotic
cavity (N) and metastatic
right obturator
lymph node (L ) are due to recurrent
cervical
carcinoma.
(c) CT scan through
the uterus
(U), normal pelvic ureters
(white arrows),
and right ovary (o)
shows a normal
asymmetric
left round ligament
(black
arrows)
resulting
from a variation
in uterine
position.
Note the triangular
shape of this round ligament,
with
gradual
distal tapering.
through
.,.,.
..
:.
.
.
.,.
‘I
,
I
.c
.\
Figure 4. Axial view of the cardinal
and uterosacral
ligaments.
Drawing
illustrates
the relationship
of the
cardinal
and uterosacral
ligaments
to the cervix.
54
U
Scientific
Exhibit
Volume
14
Number
1
a.
b.
Figure
through
woman
5.
Normal
cardinal
ligaments.
(a) CT scan
a small,
normal
cervix
(C) in a postmenopausal
shows normal,
bilateral,
thin, tapering
cardinal
ligaments
(arrows).
An additional
finding
is a large
right inguinal
lymph node metastasis
(m) from known
carcinoma
of the vulva. (b) CT scan through
a normal
cervix (C) shows
marked
asymmetry
of the cardinal
hgaments,
with the triangular
left ligament
(white arrow)
tapering
laterally
toward
the pelvic sidewall
and the
right cardinal
ligament
(black arrows)
ending
abruptly
with a wedgelike
appearance.
(C) CT scan
through
an
anteflexed
normal
uterus and cervix (c) shows an uncommon
variation
of the cardinal
ligaments
(arrows),
which do not taper and have a squared
appearance
where they end in the paracervical
fat.
C.
The round
ligament
is a band
of fibromuscular tissue
that attaches
to the anterolateral
uterine
fundus
just below
and anterior
to the
fallopian
tube and anterior
to the ovarian
ligament
(Figs 1, 2) (1,2,4,6,7).
It is positioned
anterolaterally
in a curved
course
within
the
broad
ligament
to enter
the internal
inguinal
ring and terminates
in the labia majora
(Fig 2)
(1-3,5,7). The round
ligament
is frequently
seen on CT scans
as a thin soft-tissue
band
that extends
laterally
from the fundus
and
gradually
tapers
from its relatively
broad
base
at the uterus
(9). Its appearance
is variable
(Fig 3).
January
1994
The cardinal
ligament
(transverse
cervical
ligament,
Mackenrodt
ligament)
forms
the
base of the broad
ligament
and provides
the
primary
ligamentous
support
for the uterus
and upper
vagina
(2,7).
It extends
laterally
from the cervix
and upper
vagina
to merge
with a fascia overlying
the obturator
internus
muscle
(Figs 1, 4) (2,7).
The uterine
artery
runs
along
its superior
aspect
(1). The cardinat ligament
is usually
seen on CT scans
as a
triangular
soft-tissue
structure
with the base
of the triangle
abutting
the cervix
and the
apex tapering
toward
the pelvic
sidewall
(10, 1 1). There
is a wide variation
in thickness,
shape,
and contour
of the normal
cardinal
ligament
(Fig 5).
Foshager
and
Walsh
U
RadioGraphics
#{149}
55
6.
Normal
and abnormal
uterosacral
ligaments.
(a) CT scan through
a normal
cervix (C) shows
the typical appearance
of uterosacral
ligaments
(arrows) tapering
posteriorly
from the posterolateral
margin
of the cervix
toward
the sacrum
(s). (b) CT
Figure
scan
(C)
of a thin 4-mm
shows
very fine
section
uterosacral
through
a normal
cervix
ligaments
(arrows).
These ligaments
were not identified
on the standard,
8-mm pelvic CT sections.
s = sacrum.
(C) CT scan
through
the cervix (C) in a patient
who
underwent
radiation
cervix
therapy
shows
adjacent
ally. These
for female
for squamous
thickening
to the
uterosacral
cell
of the tissue
ligaments
changes
are typical
genital
tract cancer.
after
carcinoma
of the
planes
of and
(arrows)
pelvic
bilater-
irradiation
C.
Figure 7.
Normal
ovarian
ligament.
CT scan through
the uterus
(U) shows
both ovaries
(o) and the left
ovarian
ligament
(arrow),
which lies between
the
ovary and the body of the uterus.
Note also the normal anterior
location
of the left round ligament
(arrowhead).
56
#{149}
Scientific
Exhibit
Volume
14
Number
1
a.
b#{149}
8.
Normal
suspensory
ligament
of the ovary.
Serial inferior-to-superior
sections
through
a
large central
endometrial
tumor
(7). (a) Scan shows
the base ofthe
left round ligament
(arrow).
(b) Scan
shows a portion
of the left suspensory
ligament
of the
ovary (white arrow)
posterior
to the round ligament
(black arrow).
(C) Scan shows
the normal
left ovary
Figure
(a-c)
(o) with
the
The
uterosacral
from
the
ligament
lateral
extends
cervix
and
posteri-
vagina
at the
level of the internal
cervical
os and forms
a
curved
arc toward
the anterior
body of the
sacrum
at S-2 orS-3
(4,5,7,10,11).
Its fibers
fuse
medially
dinah
ligament
with
(Figs
posterior
the uterosacral
ligament
ters thick,
it is frequently
lution
CT scanners
(Fig
January
1994
fibers
1, 4)
(2,4,1
of the
ligament
(arrow).
The ovarian
ligament
(round
ligament
of
ovary)
extends
medially
from the ovary to
the uterus,
just inferior
and posterior
to the
fallopian
tubes
and round
ligaments
(Figs 1,
2) (3,4,9).
Its position
varies
with the ovaries.
This structure
is usually
not identified
on CT
scans
(Fig 7).
The suspensory
ligament
of the ovary (infundibulopelvic
ligament)
occupies
the lateral
aspect
of the free upper
edge of the broad
ligament
(Fig 1) (3,4).
It extends
from the
ovary anterolaterally
over the external
iliac
C.
orly
its suspensory
vessels
to fuse
with
connective
tissue
over
psoas
muscle
(1). The suspensory
ligament
transmits
the ovarian
artery
and vein and
rarely
seen on CT scans
(Fig 8) (1,3,6).
the
is
car-
1). Although
is only a few millimeseen with high-reso6).
Foshager
and
Walsh
U
RadioGraphics
#{149}
57
Fo1
1
Figure
9.
Posterior
view of the pelvic
vascular supply.
Drawing
illustrates
o=Vk(
the
course
of the uterine
and ovarian
blood
vessels and their relationships
pelvic
1!’
\
u.
uw*.
Aflsry
k
w
wd
to the
viscera
F
and
ligaments.
Figure
ternal
course
their
Note
10.
Detailed
organ vascular
of the uterine
branches,
particularly
anterior
view of the pelvic insupply.
Drawing
illustrates
the
and ovarian arteries
and veins,
and their rich anastomotic
the relationship
of the
to the pelvic ureter
uterine
artery.
as the ureter
passes
networks.
uterine
artery
below
the
U VASCULAR
SUPPLY
TO THE
PELVIC
ORGANS
The paired
uterine
arteries
provide
the primary blood
supply
to the uterus
(Figs 9, 10)
(1,7).
These
large arteries
are branches
from
the anterior
(visceral)
trunk
of the internal
iliac (hypogastric)
arteries
(2,3,7).
The uterine
artery
courses
medially
above
the cardinal
ligament
in the base of the broad
ligament
and crosses
anterior
to the pelvic
ureter
en
route
to the cervix
(Fig 10) (1,3-6,12-14).
The artery
divides
and sends
a smaller
cerncovaginal
branch
inferior
to the vagina
and
lower
cervix
and a larger
uterine
branch
supenor to the uterus
(Figs 9, 10) (3,7,15).
Each of
these
branches
is tortuous
and forms
extensive
and
vascular
uterus,
artery
ultimately
trifurcates
at the upper
with branches
to the fallopian
tube,
uterine
fundus,
and the ovary
(1,2,5).
uterus
the
58
#{149}
Scientific
Exhibit
networks
respectively
lateral
(4,7,
to the vagina
14). The uterine
The
ies
that
vagina
arise
is also
directly
supplied
from
by vaginal
the
internal
arteriliac
arteries
(1). The uterine
arteries,
their branches
and rich anastomotic
networks,
and their anatomic
relation
to the pelvic
ureters
can often
be precisely
identified
with high-resolution
CT scanning
techniques
tailored
to the pelvis.
The arteries,
which
demonstrate
the most intense
opacification
when
the arterial
bolus
of
contrast
material
reaches
the pelvis,
enhance
along with the internal
and external
iliac arteries.
The CT appearance
of the uterine
arteries
is variable
(Figs 1 1, 12).
Volume
14
Number
1
Figure
1 1 . Normal
uterine
arteries.
(a) CT scan at the level of the
left uterine
artery (arrow)
Note the concurrent
opacification
of the
(b) CT scan obtained
at a slightly
higher
level than a shows
that the
the lateral aspect of the uterus
(U) and lower uterine
segment.
(C)
a beaded
appearance
of the opacified
right uterine
artery (arrow).
.
cervix
(C) shows
a prominent
enhanced
external
iliac arteries
(arrowheads).
artery
(arrows)
courses
superiorly
along
CT scan through
a normal
cervix (C) shows
(d) CT scan
through
an anteverted
uterus
shows
prominent
enhancing
uterine
vessels
(arrows)
ascending
along
the lateral
aspect
of the uterus,
where
they will eventually
anastomose
with branches
of the ovarian
vessels.
These
vessels
most likely represent
uterine
arteries,
given the concurrent
enhancement
of the external
iliac arteries
(arrowheads).
(Reprinted,
with permission,
from reference
18.) (e) CT scan through
the cervix
(c) in an elderly
diabetic
woman
shows
characteristic
calcification
in both uterine
arteries
(arrows).
i;”
‘,
-
.
..
.
..:--‘#{149}-.
a.
c&!*1
.
b.
e.
January
1994
Foshager
and
Walsh
U
RadioGraphics
#{149}
59
a.
12.
Figure
tomic
Uterine
relationship
arteries
and their
to the pelvic
ureters.
through
a normal,
anteflexed
lateral uterine
arteries
(large
orly
over
ureters
artery arc sign’ ‘ is the
of the uterine
artery
scan through
a cervix
tumor
(7) shows
rows)
completely
arrow),
nal
the
arrows)
classic
(c)
uterine
segment
carcinoma
shows
shows biarcing anteri-
(U)
.
This
anatomic
‘
‘uterine
I.
relationship
to the pelvic
ureter.
(b) CT
replaced
with endometrial
an arc of blood
surrounding
representing
branches.
(small
uterus
arrows)
normal
ana(a) CT scan
vessels
the
the uterine
CT scan
obtained
(white
ar-
left ureter
(black
artery
and its vagiat the lower
in a patient
with stage IIIB cervical
bilateral
prominent
uterine
arter-
ies (white
arrows)
arising
teries
(arrowheads),
with
arcing
over an obstructed
‘V
from the internal
iliac arthe right uterine
artery
ureter
(black
arrow).
Venous
drainage
of the upper
vagina,
ceruterus,
and ovaries
is via an extensive
plexus of thin-walled,
valveless
veins that lie
between
the layers of the broad
ligament
within
the parametrium
(1,3,5,12).
This
vix,
plexus
eventually
forms
veins that largely
parallel the arterial
blood
supply
(1,4,5,7).
The
left ovarian
vein, however,
drains
into the left
renal
vein instead
of the inferior
vena cava
(4,5). The veins and their companion
arteries
can be seen on CT scans
as enhancing
vascular networks
or a plexus
in the pelvic
fat.
Their
appearance
varies
from prominent
yessets to very delicate
strands
(Fig 13).
The paired
ovarian
arteries
(gonadal
arteries)
arise
the
the
origin
ovarian
directly
from
the
aorta
just
below
of the renal
arteries
(2,3,7).
Once
artery
descends
to the pelvis,
it
enters
the broad
ligament
through
the suspensory
ligament
of the ovary
(Figs 9, 10) and
sends
multiple
branches
to the ovary via the
mesovarium
(1,2,5,7).
The artery continues
medially
to anastomose
with the ovarian
branch
ofthe
uterine
artery (Figs 9, 10) (1,3,5,7).
This vessel
is infrequently
visualized,
even
with high-resolution
dynamic
scanning
techniques
(Fig 14).
U
PELVIC
Improved
bihities,
VISCERA
high-resolution
combined
with
CT scanning
dynamic
capa-
inferior-to-
superior
image
acquisition,
utilize
the rich
vascular
supply
to the uterus,
cervix,
and vagina to better
define
normal
and disease
processes
not previously
visualized
on CT scans.
Endometrium
and myometrium
cannot
yet be
differentiated
from one another
on CT scans.
However,
endometrial
and myometrial
60
#{149}
Scientific
Exhibit
Volume
14
Number
1
a.
b.
Figure
13.
Cervical
and vaginal vascular
plexus.
(a) CT scan through
a normal
cervix
(c) shows
a
very delicate,
enhancing
vascular
network
(arrows)
along the lateral aspects
of the cervix and in the hatera! paracervical
cervical
tumor
(7)
fat. (b) CT scan through
surrounded
by normal
cervical stroma
shows a prominent
fled cervicovaginal
vascular
plexus
scan
obtained
at the
level
of the
that the bilateral
paravaginal
rows) is prominent
lateral
jacent
to the
pelvic
a central
peripheral
bilateral,
(arrows)
vagina
(V)
.
opaci(c) CT
shows
vascular
plexus
(arto the rectum
(r) and ad-
sidewall.
C.
a.
Figure
b.
14.
Ovarian
vascular
supply.
(a) CT scan through
the uterus
(U) and both ovaries
(o) shows
an enhancing
curvilinear
vessel
(arrow)
along
the posterior
aspect
of the right ovary.
(b) CT scan of the same
patient,
obtained
at a slightly
higher
level through
the right ovary
(o), shows
the contrast-enhanced
right ovarian blood
vessels
(arrow)
in the right ovarian
ligament.
January
1994
Foshager
and
Walsh
#{149}
RadioGraphics
S
61
a.
b.
C.
Figure
15.
Normal
and abnormal
uterus.
(a) CT scan through
an anteflexed
uterus
and a large central
cervical tumor
(7) shows
a normal
contrast-enhanced
uterine
myometrium
(m) and central
endometnal
cavity
(e). (b) CT scan through
a uterine
fluid collection
(f) that contains
a Copper-7
intrauterine
device
(arrow)
(Searle
Laboratories,
Chicago,
Ill) shows
contrast
enhancement
ofthe
myometrium
(m), which helps to delineate
a portion
of the nonenhanced
obstructing
cervical
tumor
(7). (c) Dynamic
CT scan through
an adenosquamous
carcinoma
of the myometrium
shows
a round
hypoattenuating
tumor
(7) invading
the myometrium
(m) and a dilated
almost
complete
washout
the mass (arrow)
is seen.
enhancement
metrial
cavity
helps
from
identification
of lesions
wall (Fig
vical and
determined.
enhancing
correlates
central
endometrial
of the initial
myometrial
to distinguish
the uterus
and
within
the endoaids in the
uterine
1 5). The CT spectrum
of normal
cervaginal
enhancement
is still being
It is likely that the moderately
peripheral
portion
of the cervix
with the fibrous
stroma
described
in MR
imaging
and
pathologic
(16,17).
The
highly
enhancing
believed
16) (16).
the
cavity
(e). (d)
enhancement
to represent
The intense
cervical
central
inner
zone
is
epithelium
(Fig
vaginal
enhance-
its ovarian
ships,
patient
focal
shows
enhancement
superiorly
posteriorly
vessels;
(Figs
as well
of
by
the
by the
external
ureter
and
in-
and medially
by the ovar1, 2) (1 ,3). These
relation-
as the
are well
Ovarian
(3,7,10,1
Exhibit
of the same
residual
vessels;
ternal
iliac
ian ligament
17).
#{149}
Scientffic
Some
vessels;
ovaries,
62
CT scan
(m).
ment
likely corresponds
to vaginal
mucosa
that can be differentiated
from the poorly
enhancing
vaginal
wall (Fig 16) (16).
The ovaries
lie tucked
in the ovarian
fossa
on the posterior
floor of the true pelvis
(1,5).
They are bordered
anteriorly
by the broad
ligament,
mesovarium,
and hilus of ovary with
iliac
correlations
Delayed
internal
delineated
position
anatomy
of the
on CT scans
is extremely
(Fig
variable
1).
Volume
14
Number
1
a.
b.
Figure
16.
Cervix
and vagina.
(a) Dynamic
CT scan through
a normal
cervix
shows
presumed
normal
central enhancement
ofthe
cervical
epithelium
(arrow).
The peripheral
cervical
stroma
enhances
to a lesser
degree (arrowhead)
. (b)
CT scan through
the vagina at the suprapubic
level shows central
intense
contrast
enhancement
of the vaginal
mucosa
(black
arrows)
and the poorly
enhancing
vagina!
wall (white
arrows).
b.
a.
Figure
17.
Normal
ovaries.
(a)
CT
scan
through
a
normal
uterus
(U) and a small left ovarian
cyst (o)
shows
the normal
relationship
of the pelvic
ureter
(white
arrow)
posteriorly
and the round
ligament
(black
arrow)
anteriorly.
(b) CT scan through
an
anteverted
uterine
body
(U) shows
a normal
right
ovary with multiple
large follicles
(arrows).
(c) Dynamic
CT scan through
a central
small cervical
tu-
mor (7) shows an anatomic
variation
sition of the ovaries
(o) bilaterally.
with
a low p0-
C.
January
1994
Foshager
and
Walsh
#{149}
RadioGrapbics
U
63
. CONCLUSION
Advances
in CT technology
and protocols
taibred
to examination
of the female
pelvis
make
possible
precise
identification
of structures
previously
not well delineated
with CT.
The utility of this knowledge
in the evaluation
of female
pelvic
abnormalities
when
compared
with ultrasound
and magnetic
resonance
imaging
has not yet been
definitively
studied.
Transvaginal
ultrasound
is ideally
suited
to the evaluation
of the ovaries
and
characterization
of pelvic
Knowledge
and
We also thank
ration,
and
We thank
RT (R) for her
Helen
Elizabeth
Rhonda
assistance
Durgin
Dempsey
Dragan
Elizabeth
in image
Ander-
5.
7.
8.
10.
11.
.
13.
14.
prepa-
illustrations,
for photography.
REFERENCES
1.
Gardner
E, Gray DJ, O’Rahilly
R.
Philadelphia,
Pa: Saunders,
1960;
609.
Netter
3.
lustrations.
Vol 2. Reproductive
system.
New
York, NY: Colorpress,
1965; 89-123.
Snell RS.
Gross anatomy
dissector:
a companfor
Little,
Invited
The
atlas
CIBA
of clinical
Brown,
1978;
collection
596-
2.
ion
FH.
Anatomy.
568-570,
anatomy.
ofmedical
Boston,
Novak’s
1981;
textbook
of gyne-
Md: Williams
&
8-15.
MacDonald
PC, Gant NF.
Williams
obstetrics,
17th ed. Norwalk,
Conn: AppletonCentury-Crofts,
1985; 7-30.
Agur AMR.
Grant’s
atlas of anatomy.
Baltimore,
Md: Williams & Wilkins, 1991; 170-177.
SciarraJJ,
McEhin TW.
Gynecology
and obstetrics. Cambridge,
Mass: Harper
& Row, 1980;
1-19.
Vick CW, WalshJW,
WheelockJB,
Brewer
WH.
CT of the normal
and abnormal
parametria
in
cervical
cancer.
AJR 1984; 143:597-603.
Cahill DR, Orland
MJ, Reading
CC.
Atlas of human cross-sectional
anatomy.
2nd ed. New York,
NY: Wiley,
1990; 67-94.
LeeJK,
Sagel SS, Stanley
RJ.
Computed
body
tomography.
New York, NY: Raven,
1989; 851854.
Walsh JW.
Computed
tomography
of the pelvis.
New York, NY: Churchill-Livingstone,
1985;
1-21.
Platzer W.
Pirnkopf
anatomy:
atlas of topographic
and applied
human
anatomy.
Baltimore,
Md: Urban & Schwarzenberg,
1989; 292-304.
Friedman
AC, Radecki
PD, Lev-ToaffAS,
Hilpert
PL.
Clinical
pelvic imaging.
St Louis, Mo:
Mosby,
1990; 19-23.
Hoskins
WJ, Perez CA, Young
RC.
Principles
and practice
ofgynecologic
oncology.
Philadelphia,
15.
16.
.
GS.
PritchardJA,
6.
12
Jones
10th ed. Baltimore,
Wilkins,
acquisition.
for manuscript
for medical
HW,
cology.
9.
visceral
anatomy
is currently
helpful
in identifying
pelvic
structures
and distinguishing
gynecologic from nongynecologic
abnormalities
on
CT scans.
Further
investigation
is necessary
to
fully define
the usefulness
of the precise
vascular definition
now available
with CT and to
determine
its potential
usefulness
in tumor
staging.
It is hoped
that familiarity
with variations in the CT appearance
of normal
female
pelvic
anatomy
will facilitate
more
accurate
assessment
of pelvic
abnormalities.
son,
Jones
masses.
of ligamentous
Acknowledgments:
4.
17.
il-
18.
Mass:
83-104.
Pa:
Lippincott,
1992;
447-448,
591-592.
Meschen
I. An atlas ofanatomy
basic to radiology. Philadelphia,
Pa: Saunders,
1975; 10831095.
Carrington
B, Hricak
HM.
The uterus
and vagina. In: Hricak
H, ed. Mifi of the pelvis. Norwalk, Conn: Appleton
& Lange,
1991; 93-127.
LeeJKT,
Gersell DJ, Balfe DM, WorthingtonJL,
Picus D, Gapp G.
The uterus:
in vitro MR-anatomic correlation
of normal
and abnormal
specimens.
Radiology
1985; 157:175-179.
Walsh JW.
Computed
tomography
of the pelvis.
In: Haaga JR, ed. CT and MIII of the whole
body.
3rd ed. St Louis, Mo: Mosby-Year
Book (in
press).
Commentary
From:
Robert
R. Hattery,
Cahill,
PhD,
MD,
Department
The preceding
article
principles
applicable
Carl C. Reading,
MD, Department
ofAnatomy,
Mayo Clinic
and
contains
three
basic
to CT of the pelvis:
CT
technique,
image
quality,
and knowledge
female
pelvic
anatomy.
Accurate
diagnoses,
64
#{149}
Scientific
Exhibit
of
of Diagnostic
Mayo Foundation,
Radiology,
Rochester,
Donald
R.
Minnesota
staging
of neoplasm,
assessment
of postoperative changes
or follow-up
of a disease
process
for example,
are dependent
on impeccable
technique,
the highest
quality
of images,
and
recognition
of normal
anatomy.
Volume
14
Number
1