Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
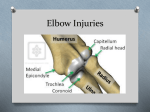
DIAGNOSIS AND MANAGEMENT OF ELBOW PAIN ELBOW PAIN • Lateral elbow pain • Medial elbow pain • Posterior elbow pain Lateral elbow pain - Causes • Common – Extensor tendinopathy – Referred pain (cervical/ upper thoracic/ neural) • Less common – Sinovitis of radiohumeral joint – Posterior interosseous nerve entrapment • Rare – Osteocondritis dissecans (capitulum/ radius) Lateral elbow pain - History • History of pain – Onset, duration, character, severity, radiation, aggravating movements. – Recent change of activity – Treatment obtained – RA , DM Lateral elbow pain- Examination 1. 2. 3. 4. 5. 6. Observation Active movements Passive movements Resisted movements Palpation Special tests Examination of the patient with lateral elbow pain Active movement Wrist flexion with forearm fully pronated Examination of the patient with lateral elbow pain Resisted muscle testing Wrist extension Examination of the patient with lateral elbow pain Resisted muscle testing Extension at third metacarpophlangeal joint Examination of the patient with lateral elbow pain Restricted muscle testing Grip strength, attempt to reproduce pain Examination of the patient with lateral elbow pain Palpation Lateral epicondyle Try to locate painful site distal to the lateral epicondyle Examination of the patient with lateral elbow pain Neural tension test Upper limb tension test with forearm pronation to isolate the radial nerve Lateral elbow pain - Causes • Common – Extensor tendinopathy – Referred pain (cervical/ upper thoracic/ neural) • Less common – Sinovitis of radiohumeral joint – Posterior interosseous nerve entrapment • Rare – Osteocondritis dissecans (capitulum/ radius) Extensor tendinopathy • Pathology – Degeneration of ECRB tendon in proximal 1-2 cm – Angiofibroblstic hyperplasia which contain large number of nociceptive nerve endings. – Microscopic tears in degenerative tissue leading to scarring Process leading to development of ERCB tendinoathy Clinical features • 40 to 50 years • Associated with repeated wrist extension activity • Maximal tendernes is 1 to 2 cm distal to lateral epicondyle • Rest of the muscle is tight and hypersensitive • Tests – Mills’ test , Extension of middle finger • *perform neural tension tests • *Examine cervical spine Treatment • A combination of different treatments necessary 1. Control of inflammation with rest, ice, NSAIDS 2.Electrotheraputic modalities ultrasound, laser, galvanic stimulation 3. Local heat therapy (heat retaining brace) 4. Massage therapy sustained myofascial tension transverse friction digital ischemic pressure 5. Dry needling of trigger points Treatment cont. 6. Muscle stretching 7. Muscle strengthening 8. Treat other components of pain 9. Correct predisposing factors 10. Corticosteroid injection 11. Surgery 12.Graduated return of activity Massage techniques Sustained myofascial tension Applied to the injured area from proximal to remove fibrous irregularities Massage techniques Transverse friction with extensor tissue under tension (wrist and hand flexion) Muscle stretching Stretching of ERCB tendon Strengthening exercises for elbow Concentric and eccentric Treat other components of pain Cervical mobilization Correct predisposing factors Incorrect Back hand technique Correct Steroid Injection Lateral elbow pain Posterior interosseous nerve entrapment Possible entapments @ fibrous bands in front of the radial head Recurrent radial vessels Arcade of Frhose Tendinous margin of the ECRB muscle Posterior interosseous nerve entrapment Neural stretch Medial elbow pain Common Flexor tendinopathy medial collateral ligament sprain acute chronic Less common Ulna nerve compression avulsion of medial epicondyle traction apophysitis of medial epicondyle Referred pain Medial elbow pain- Flexor tendinopathy Clinical features Repeated strain Localized tenderness just below medial epicondyle Pain on resisted wrist flexion and pronation Test – reverse Mills’ test Treatment – Same liens as lateral tendinopathy Medial elbow Pain – Flexor tendinopathy Pain is reproduced with resisted wrist flexion and forearm pronation Stretching exercises for forearm flexors and pronators Medial elbow pain Medial collateral ligament pain Acute injury Chronic injury Clinical features localized tenderness instability in valgus strain Treatment activity modification local electrotheraputic modalities ulrtasound muscle strengthening strapping Assessment of the integrity of the medial collateral ligament Medial elbow pain- Ulna nerve compression Ulna nerve entrapment Traction injuries Inflammatory adhesions Recurrent subluxation of nerve Irregularities in the bony grove Clinical features posteromedial elbow pain neurological symptoms tender nerve TREATMENT Local massage therapy Neural streching Nerve transposition Nural streching – ulna nerve The strech can be increased by further shoulder abduction, Forearm supination and wrist extension Posterior elbow pain 1. Olecranon bursitis 2. Triceps tendinopathy 3. Posterior impingement Olecranon bursitis