Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
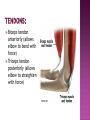
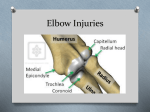
Medical ppt http://hastaneciyiz.blogspot.com The important structures of the elbow can be divided into several categories. These include: •Bones and joints •Ligaments and tendons •Capsule •Muscles •Nerves •Blood vessels There are 3 joints at the elbow: 1- Humeroulnar joint (hinge joint) – between trochlea of humerus and trochlea notch of ulnar 2- Humeroradial and radius head joint (hinge joint) – between capitilum of humerus 3- Proximal radioulnar joint (pivot joint)- between proximal end of ulna and proximal end of radius. is the material that covers the ends of the bones of any joint.with functions to absorb shock and make motion at the elbow joint easier. Ligaments are soft tissue structures that connect bones to bones. The ligaments around a joint usually combine together to form a joint capsule. Lateral Collateral Ligament Medial Collateral Ligament (Together these two ligaments connect the humerus to the ulna, to form the main source of stability for the elbow) Annular Ligament: that wraps around the radial head and holds it tight against the ulna. Biceps tendon anteriorly (allows elbow to bend with force) Triceps tendon posteriorly (allows elbow to straighten with force) The articular surfaces are connected together by a capsule Anterior part – from radial and coronoid fossa of humerus to coronoid process of ulna and annular ligament of radius Posterior part – from capitulum, olecranon fossa, and lateral epicondyle of humerus to annular ligament of radius, olecranon of ulna, and posterior to radial notch. The wrist extensors originate from the lateral epicondyle of the humerus The wrist flexors originate from the medial epicondyle of the humerus The median and ulnar nerve are at risk of injury in: -Elbow dislocation - Supracondylar fracture of humerus It is the angle at which the humerus and forearm articulate, with the elbow in full extension, and the palms facing forward The carrying angle permits the arm to be swung without contacting the hips The normal carrying angle of the elbow is about 15 degrees of valgus in males and up to 20 degrees in females. www.icareunit.com Causes Supracondylar fractures of the childhood. *Function of the elbow is almost normal. www.icareunit.com Usually indicated for cosmetic reasons; Consists of removing a bone wedge from the lateral aspect of supracondylar area. www.icareunit.com Causes: 1- Errors in management of lateral humeral condyle fracture. When present at birth it can be a sign of Turner or Noonan syndrome. www.icareunit.com Clinical features Obvious Tardy lateral angulation of the elbow. Ulnar Nerve Palsy. (most important sequel ( The ulnar nerve is repeatedly stretched behind the medial epicondyle (for many years) insidious impairment of the nerve trunk with ulnar nerve palsy. www.icareunit.com Treatment: Elbow deformity needs no treatment, but the nerve palsy is treated by transposing the nerve anterior to the elbow. www.icareunit.com The most common pathology in the elbow. Lateral epicondylitis (tennis elbow) is an overuse injury involving the extensor muscles that originate on the lateral epicondylar region of the distal humerus (any activity involving extension and/or supination). It is more properly termed a tendinosis that specifically involves the origin of the extensor carpi radialis brevis muscle. Occurs in up to 50% of tennis players Cause has been attributed to microscopic tearing with formation of reparative tissue (ie, angiofibroblastic hyperplasia) in the origin of the extensor carpi radialis brevis (ECRB) muscle Patients present with lateral elbow and forearm pain exacerbated by use Typical patient- man or woman between 35-55 years who is a recreational athlete or who engages in rigorous daily activities Treatment: - Rest - Counterforce brace - NSAIDs - Wrist splinting - Corticosteroid and injections - Low level laser therapy Approximately 90-95% of patients respond to conservative measures and do not require surgical intervention. Patients whose condition is unresponsive to 6 months of conservative therapy (including corticosteroid injections) are candidates for surgery. This condition is an overuse syndrome that is characterized by pain at the flexor-pronator tendinous origin and is seen in sports activities with repetitive valgus stress, flexion, and pronation, such as occurs in golf, baseball, tennis, fencing, and swimming. This condition is also seen with occupations that require hand, wrist, and forearm motions. Most common cause of medial elbow pain but less common than tennis elbow Males: females = 2:1 Presence of microtears in the flexorpronator tendons without inflammation Patient presents with achy pain over the anterior medial epicondyle, usually during activity, and the patient may describe weakness in the forearm or hand. In addition, radiation of the pain may occur in the shoulder, forearm, or hand. Treatment: 1- Patient education and golf-swing (or the relevant activity) modification 2- Nonsteroidal anti-inflammatory drugs (NSAIDs) 3- Counterforce brace 4- Wrist splints 5 -Corticosteroid injections Surgical treatment should be considered in cases in which conservative treatment has failed after 6-12 months and after all other pathology has been excluded. Medical ppt http://hastaneciyiz.blogspot.com