Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Turner syndrome wikipedia , lookup
DiGeorge syndrome wikipedia , lookup
Down syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
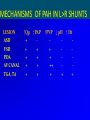
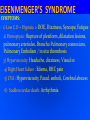
Prof. S. Shanmuga Sundaram K.S. Hospital, Chennai PULMONARY HYPERTENSION AT SYSTEMIC LEVEL, DUE TO HIGH PULMONARY VASCULAR RESISTANCE ( > 800 dynes sec cm-5 ) WITH REVERSED OR BIDIRECTIONAL SHUNT….. 8% (1950) → → → → 4% Complications associated with the Eisenmenger syndrome Vongpatanasin, W. et. al. Ann Intern Med 1998;128:745-755 DEATH: Sudden death 30% , Heart failure 23% , Hemoptysis 11% Death during noncardiac surgery & pregnancy DISSECTION OF PULMONARY ARTERY PROXIMAL PA THROMBOSIS PULMONARY ARTERIAL HYPERTENSION IN SHUNT LESIONS mPAP > 25 mmHg at rest / > 30 mm Hg post exercise PAWP < 15 mm Hg ; PVR > 3 Wood Units • TRANSMISSION OF SYSTEMIC ARTERIAL PRESSURE • VASOCONSTRICTION • VASCULAR OBLITERATION – MEDIAL HYPERTROPHY FIBROSIS INTIMAL PROLIF + ARTERIAL THROMBI OBLITERATIVE PVR PA PP/PA SP HYPERKINETIC < 5 W.U > 60% > 5 W.U < 40% ASD CA, APVC APWINDOW VSD PDA TGA VSD, DORV SINGLE VENTRICLE TRUNCUS > 2 cm > 1 cm > 1 cm PULMONARY CIRCULATION - STRUCTURAL REMODELING Elastic > Fully muscular > Partially muscular > Non muscular At birth the smallest muscular arteries dilate with medial thinning By 4 months, this process involves larger arteries & get completed Alveoli and Arteries grow both in number & size Al : Art = 20:1 > 8:1 With shunt lesions resulting in increased flow ± pressure, proximal arteries dilate, distal arteries reduce in number and size bcause of extension of muscle in media of partially or non muscular arteries NORMAL VSD MATURATION OF PULMONARY VASCULAR BED Lucas R. Am J Dis Child PAH IN L > R SHUNTS NONRESTRICTIVE VSD = 15 % < 2 yrs of life MODERATE DEFECTS = 3% ; LARGE DEFECTS (1.5cm) = 50% LARGE PDA = similar incidence LARGE ASD = 6-10% > 3rd decade Frequent in SVC, partial AV Canal defects & in Lutembacher’s TGA = 8% (intact IVS ) 40% ( VSD/PDA ) < 1 yr 75% at 2 yrs COMMON AV CANAL all develop PAH TRUNCUS ARTERIOSUS by 1-2 yrs SYSTEMIC - PA SHUNTS: BT Shunt (<10%) Waterston / Pott’s ~ 30% MECHANISMS OF PAH IN L>R SHUNTS LESION ASD VSD PDA AV CANAL TGA, TA ↑Qp ↑PAP + + + + + + + + + ↑PVP ↓ pH ↑ Ht + + ++ + + + ENDOTHELIAL DYSFUNCTION ↑ ET, TXA2 , SEROTONIN ↓ NO ,PGI2,VIP PLATELET ADHESION + THROMBUS GENETIC SUSCEPTIBIILITY BMPR2 MUTATION = 6 % 26%(IPAH) 50% (FPAH) MORPHOMETRIC GRADING Rabinovitch M Grade A : Extension of muscle into small peripheral arteries Wall thickness increased but < 1.5 times the normal ↑ PBF ↑ PA PP + NORMAL MEAN PAP Grade B : Mild : medial thickness 1.5 – 2.0 times the normal Severe : medial thickness > 2 times the normal PAH - MEAN PAP > 50 % OF SYSTEMIC LEVEL Grade C : Size and number of arteries reduced PAH - PVR > 3.5 - 6.0 u.m2 CLINICAL RECOGNITION • Apparent improvement of neonatal HF • Reduction of frequency of respiratory infections • Precordium becomes less tumultous • Flow murmur decreases > disappears • Shunt murmur decreases in intensity & duration • S2 split decreases and P2 increases in intensity EISENMENGER’S SYNDROME SYMPTOMS: 1) Low C.O + Hypoxia > DOE, Dizziness, Syncope, Fatigue 2) Hemoptysis : Rupture of plexiform, dilatation lesions, pulmonary arterioles, Broncho Pulmonary connexions, Pulmonary Embolism / in situ thrombosis 3) Hyperviscosity: Headache, dizziness, Visual sx 4) Right Heart failure : Edema, RHC pain 5) CVA : Hyperviscosity, Parad. emboli, Cerebral abscess 6) Sudden cardiac death: Arrhythmia EISENMENGER’S SYNDROME SIGNS : 1) Cyanosis and Clubbing 2) JVP inconspicuous 3) Pulmonary Ejection Sound 4) 2-3/6 Ejection Systolic Murmur 5) Loud P2 6) Murmurs of TR and PR EISENMENGER’S SYNDROME FEATURE ASD Neonatal HF - Age 30-40 - - Single - Differential ± + Fixed - 2-12 Uniform - Prominent ‘a’ JVP S2 split Long PR murmur 2-12 + PDA + ± Uniform Cardiomegaly,PSH Wide pulse pressure + ± Syncope Cyanosis VSD Normal + - PAH GROWING PDA DOPPLER PATTERN S PULSATILE CLOSING CLOSED DOPPLER IN PDA SHUNT LESIONS - OPERABILITY Qp : Qs = > 2:1 No or mild PAH Qp : Qs = < 1.5:1 Severe PAH - INOPERABLE Qp = O2 Consumption / PV – PA O2 content Qs = O2 consumption / SA - MV O2 content O2 content = O2 saturation x O2 carrying capacity x Hb Qp : Qs = SA – MV O2 sat / PV – PA O2 sat Why to assess operability ? CHD PAH – REVERSIBILITY TESTING HIGH SURGICAL RISK ( 20% ) RIGHT VENTRICULAR FAILURE ( IPAH like ! ) PROGRESSION OF PAH AGENTS CRITERIA 100% OXYGEN (10 mts) ↓Rp /Rs > 20% NITRIC OXIDE (10-80ppm) Rp:Rs < 0.33 02 + N.O (Se 97% Sp 90%) Rp < 8 u.m2 ADENOSINE (50-500µg/kg/mt) EPOPROSTENOL (2-10 ng/kg/mt) ILOPROST (2.5-5.0 µg ) ASSESSING OPERABILITY BASED ON PVR MISTAKES & MISCONCEPTIONS 22 to 44% 40 to 60% 60 to 100% Expecting PAP to decline ( ↓ PVR > ↑ FLOW ) Assuming O2 consumption Ignoring dissolved O2 in calculating PVR O2 sat x 1.36 x Hb = 60 x 1.36 x 12 = 98 ml/L ( 0.03 x 55 = 1.7ml ) 98 x 1.36 x 12 = 160 ml/L ( 0.03 x 95 = 2.9ml ) PVR = 60 – 8 = 52 / 3.2 = 16 units ( 16.5 units ) After 100% oxygen : 72 x 1.36 x 12 = 118 ml/L ( 0.03 x 100 = 3 ml ) 98 x 1.36 x 12 = 160 ml/L ( 0.03 x 500 = 15 ml) PVR = 55 – 8 = 47 / 4.8 = 9.8 units ( 12.7 units ) PVR INDEXED TO BODY SURFACE AREA A child of BSA of 0.5 m2 has a PBF of 2 l/mt PA mean pressure = 20 mmHg ; mean LAP = 8 mmHg PVR absolute value = 20-8/2 = 6 units If corrected for BSA = 6/0.5 = 12 units PBF corrected to BSA = 2/0.5 = 4 l/mt/m2 PVR indexed to BSA = 20-8/4 = 3 u.m2 ROLE OF ECHOCARDIOGRAPHY • Qp/Qs by doppler, PAcT not reliable • PA peak velocity > 1.0 m/s predictive • PVR = TR Velocity/ TVI RVOT x 10 + 0.16 • Vp > 18 cm/s = PVR < 6 units 4 WU 8.8 W.U 12.4 cm/s 16.4 W.U 23.1 cm/s PULMONARY WEDGE ANGIO PREDICTION OF PVOD Wilson NJ CCVD 1993;28:22 PREDICTING HEATH EDWARDS Grade III - IV Sensitivity Specificity PVR > 6 units 100% 94% Monopedial count<3 83% 100% Abnormal blush 83% 69% Combination of all 100% 100% LUNG BIOPSY MORPHOMETRIC GRADING Rabinovitch M Grade A : Extension of muscle into small peripheral arteries Wall thickness increased but < 1.5 times the normal ↑ PBF ↑ PA PP + NORMAL MEAN PAP Grade B : Mild : medial thickness 1.5 – 2.0 times the normal Severe : medial thickness > 2 times the normal PAH - MEAN PAP > 50 % OF SYSTEMIC LEVEL Grade C : Size and number of arteries reduced PAH - PVR > 3.5 - 6.0 u.m2 CARDIAC MR DEFECT SIZE & LOCATION PA SIZE ↑ WITH PAH RV FUNCTION Qp/Qs RATIO Phase contrast velocity mapping MR OXIMETRY ( T2 relaxation time) DEGREE OF PAH BALLOON OCCLUSION IN HYPERTENSIVE DUCTUS Roy A IHJ 2005;57:332 Fall in m/d PAP > 20 mmHg TRIAL OCCLUSION OF PDA Yan C Heart 2007;93:514 Trial occlusion for 30 mts with ADO Reduction of mPAP 78 ± 19.3 to 41 ± 13.8 mm Hg FU for 3 to 6 months – clinical improvement PAH IN ATRIAL SEPTAL DEFECT • 6% ( Mayo clinic); 9% - half were below 20 yrs(CMC) • PAH (mPAP>30 mmHg) 26% SVC (9% FO) ↑PVR 16% SVC (4% FO ) ; at younger age • 85 % were women ( overall F:M = 2:1 ) • PVR > 15 units do poorly – death / progression of PAH • PVR < 10 units do well with surgery • PVR 10 – 15 units – if SPO2 is < 90% surgery not useful DEVICE CLOSURE IN ASD + PAH Balint OH Heart 2008;94:1189 PAH Moderate Severe PASP 50-59 >60 At 3 m PASP ↓ 57± 11 to 51±17 At 3 yrs PASP ↓ to 44 ±16 Only in 43.6% PAP normalised 15.4% had persistent severe PAH EISENMENGER’S SYNDROME MANAGEMENT Avoid dehydration, livingISSUES at high altitude Air travel safe (supplemental O2) Avoid pregnancy ( No OCP – tubal ligation/vasectomy) Treat Iron deficiency ( MCV < 82 ) ; hyperuricemia Vensection for hyperviscosity syndrome Antiplatelet / Anticoagulants ? Disease targeting therapies : Prostacyclin & analogues, sildenafil, bosentan Surgery: Correction after PA banding, prolonged vasodilator therapy, Heart Lung Transplant Management of the patient with the Eisenmenger syndrome and erythrocytosis Vongpatanasin, W. et. al. Ann Intern Med 1998;128:745-755 Causes of and Therapy for Hemoptysis in Patients with the Eisenmenger Syndrome Vongpatanasin, W. et. al. Ann Intern Med 1998;128:745-755 BOSENTAN IN CHD + PAH Diller GP Heart 2007;93:974 BOSENTAN IN CHD + PAH 2007;93:621 Alto MD, Heart PROGNOSIS EISENMENGER SYNDROME ~ IPH ACTUARIAL SURVIVAL 1 yr 2 yr 3 yr E.S 97 % 89 % 77 % IPAH 77 % 69 % 35 % MORPHOMETRIC GRADING Rabinovitch M Grade A : Extension of muscle into small peripheral arteries Wall thickness increased but < 1.5 times the normal ↑ PBF ↑ PA PP + NORMAL MEAN PAP Grade B : Mild : medial thickness 1.5 – 2.0 times the normal Severe : medial thickness > 2 times the normal PAH - MEAN PAP > 50 % OF SYSTEMIC LEVEL Grade C : Size and number of arteries reduced PAH - PVR > 3.5 - 6.0 u.m2 Pooled Data from Studies of Pregnant Patients with the Eisenmenger Syndrome* Vongpatanasin, W. et. al. Ann Intern Med 1998;128:745-755 VENTRICULAR SEPTAL DEFECT PATENT DUCTUS ARTERIOSUS