Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
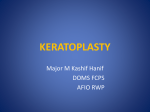
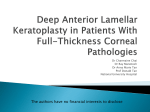
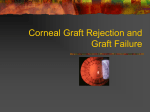
Acta Ophthalmologica 2015, Vol.41(1) ISSN 1452-3868 Originalan rad UDK: 611.841+617.7-089+615.461 STROMAL REJECTION EPISODE AFTER DEEP ANTERIOR LAMELLAR KERATOPLASTY (DALK) Ljubiša Nikolić*, Vesna Jovanović**, Slađana Delević* * Special Eye Hospital Oculus ** Faculty of Dentistry University of Belgrade, Ophthalmology Clinic, “Prof. dr Ivan Stanković”, KBC “Zvezdara” Purpose: To report an uncommon complication of the deep anterior lamellar keratoplasty in a patient with keratoconus. Methods: Deep anterior lamellar predescemetic keratoplasty was done in a patient with advanced keratoconus. Orbscan was used for corneal topography and thickness measurements. Rostock cornea module was used to measure the endothelial cell count. Results: Patient had a stromal rejection episode 14 months postoperatively. After its reversal, the graft remained clear, but with only 1449+19 cells per mm2. Conclusion: Although safer than a penetrating graft, the deep anterior lamellar corneal transplantation is not devoid of complications. However, complications can frequently be managed successfully by using medical therapy. The frequency of rejection can probably be lessened by a timely suture removal. Acta Ophthalmologica 2015;41(1):18-22. Key words: cornea, DALK; keratoconus; rejection Introduction Deep anterior lamellar keratoplasty (DALK) has become an alternative to penetrating keratoplasty (PK) in the treatment of keratoconus (KC) (1). Although PK is easier to perform and can yield superior visual results to lamellar keratoplasty, the disadvantages of the full-thickness graft include less intraoperative safety, a weakness to blunt trauma at the edge of the graft, an irregular astigmatism, and more frequent rejection episodes followed by more frequent graft failures (2). DALK permits preservation of the healthy endothelium of a young recipient, which makes late endothelial failure less probable and excludes endothelial rejection. However, the rejection of other 18 corneal layers is still possible (3,4). In the past, rejection of the epithelium and stroma in a lamellar graft were believed to be so rare that the authors used the word “exceptional” (5). More recently, the rejection of these layers was found to happen in 4.3%, 4.5%, and even 14.3% (6-8). Most of these grafts were saved after topical corticosteroid therapy. Thus, it seems worthwhile to address this issue again. We report a case of stromal rejection after DALK for keratoconus with epithelial edema and small bullae formation at the time when all donor epithelium was expected to be replaced by the host epithelium, making an epithelial rejection impossible, and present the endothelial cell loss found after the rejection reversal. Acta Ophthalmologica 2015, 41(1) Materials and methods A 37-year-old Caucasian man with keratoconus was reported for keratoplasty. He had a history of eye rubbing and contact lens intolerance. He had never experienced episodes of either vernal conjunctivitis or herpes. Munson’s sign was obvious in the right eye. Visual acuity of his right eye was finger counting at four meters, and could not be improved by any spectacle lenses. In his left eye, a spectacle correction of -2.75–1.50X100 gave a BCVA of 20/25. His left eye presented as a forme fruste keratoconus. On the slit-lamp examination, only a thin conical cornea was observed, without any signs of the corneal hydrops, guttae, keratic precipitates, a flare in the anterior chamber or vernal conjunctivitis. Axial length was 24.7mm and 24.2mm respectively. Orbscan (Bausch and Lomb, Munich, Germany) revealed a typical keratoconus in his right eye, with a thin cornea (340 micrometers) paracentraly and centrally, and of a normal thickness at the periphery (540 micrometers). (Figure 1) Endothelial cell count was measured with the Rostock Cornea Module (RCM) of Heidelberg Retina Tomograph (HRT) (Heidelberg Engineering GMBH, Dossenheim, Germany). Descemet’s membrane and endothelium were swept off from the donor cornea, which had previously been kept for five days in Optisol (Bausch and Lomb). An 8.50mm graft was transplanted into an 8.25mm corneal bed created by predescemetic dissection, and sutured with 18 interrupted 10-0 nylon sutures. Dexamethasone and gentamycin were injected subconjunctivally at the end of surgery. Seventeen sutures were taken off during the first three months postoperatively. One deeply buried suture was left at 10 o’clock. Dexamethasone 0.1% drops were tapered from six times to once daily. Seventeen sutures were taken off during the first three months postoperatively. was clear. The graft was edematous and hazy, but without vascularization, precipitates or infiltrates. Epithelium was edematous, with small bullae and erosions (Figure 3A). The graft-host interface seemed inconspicuous. Intraocular pressure was 14mm Hg. It took three months to clear the graft with topical Dexamethasone 0.1% eye-drops eight times daily for a month and six times daily for two months, and 5% sodium chloride ointment before bedtime. After the treatment, intraocular pressure was 17mmHg, but a posterior cortical cataract was noted in the right eye only. BCVA deteriorated to 20/60. Endothelial cell count was 1449+SD 19 in the operated eye, and 2689+SD 19 in the intact eye. (Figure 3B) Five months later, phacoemulsification and intraocular lens implantation were done. The graft remained clear, and the correction of -0.5-1.75X100 gave BCVA of 20/25. Figure 1.Stromal and epithelial edema of the graft, 14 months after DALK Results The graft remained clear during a 14 months follow-up. (Figure 2) At 12 months, BCVA was 20/30 with the correction of -6.0– 1.0X110. Endothelial cell count, measured with the Rostock Cornea Module (RCM) of Heidelberg Retina Tomograph (HRT) (Heidelberg Engineering GMBH, Dossenheim, Germany) was 2016+SD 19. Then, the patient appeared between two monthly visits, complaining of a sudden visual deterioration which had lasted for five days. At the slit-lamp, the peripheral, recipient cornea Figure 2. Clear lamellar graft after rejection reversal 19 Acta Ophthalmologica 2015, 41(1) Discussion Figure 3A. Graft endothelium after rejection reversal shows cell loss and polymegatism Figure 3B. Normal endothelial cell count and appearance before rejection episode 20 Our patient was young, active, with a history of eye rubbing and contact lens intolerance. His low visual acuity could not be corrected with spectacle lenses. His central cornea was very thin and without signs of an ongoing or past hydrops. The aim of surgery was to achieve a useful visual acuity, normal corneal thickness, optimal peripheral wound strength, while preserving the healthy endothelium and lessening the chances of rejection. Therefore, it was decided to rule out penetrating keratoplasty, intracorneal rings and collagen cross-linking, and to perform DALK with the use of interrupted sutures in order to stimulate healing at the edge of the graft (9). A sudden edema of the graft appeared 14 months after surgery. In the absence of any diagnostic tests, it was diagnosed clinically as rejection (3). Herpes was excluded as the cause of the graft opacity because there had not been a history of ocular or labial herpetic infection, there were no obvious clinical signs of the disease, and a short topical corticosteroid treatment did not cause a progression of the corneal disease. The inconspicuous graft-host interface helped to rule out keratitis originating from that site. Vascularization and infiltrates in a graft, frequent but not necessary accompanying signs of rejection (4,5), were missing in this case. However, the retained interrupted suture was suspected to be the immune reaction trigger (10). Our case presented with both epithelial and stromal edema 14 months after the surgery, and five days after the beginning of the symptoms. The epithelial rejection would not be possible at that time because of the prior replacement of the donor epithelium by host epithelium (10,11). On the other hand, the first stromal rejection episode may happen even 41 months after DALK (4). Moreover, the epithelial edema in our case looked as if being caused, at least partially, by endothelial dysfunction. Watson, Tuft and Dart have already discussed this possibility, and have suggested inflammation in the stroma, stromal cellular infiltrates, and abnormalities in the endothelium of keratoconus patients as possible causes of endothelial decompensation (4). In our case, the 28% loss of endothelial cells during the rejection episode seemed to be one of the causes of the endothelial decompensation which took three months to clear, possibly by sliding of the host endothelial cell in the presence of a therapeutically suppressed immune reaction. It seems probable Acta Ophthalmologica 2015, 41(1) that this loss can be attributed to the inflammatory immune reaction based on the difference between pre- and post-rejection endothelial cell counts, from the estimate of the long-term endothelial loss after uncomplicated DALK to be up to 13% (12-15), as well as from the absence of contact lens wear, which proved to be harmful to the endothelium in keratoconus (16). The exactness of the method which we used has been shown by a recent comparison of the mean endothelial cell densities measured with an endothelial microscope (EM) and with RCM showing no significant differences, although EM counts had a lower standard deviation (17). In conclusion, we present a previously uncommon complication of DALK: high endothelial cell loss after a rejection episode. Its incidence can probably be lowered by a timely suture removal, while its reversal can be accomplished by medical therapy. References 1. Agarval R. Deep lamellar keratoplasty: an alternative for penetrating keratoplasty (editorial). Br J Ophthalmol 1997;81:178-9. 2. Benson WH, Goosey JD Lamellarke-ratoplasty. In: Krachmer JH, Mannis MJ, Holland EJ (Eds).) Cornea 2nd Edition; Volume 2, Elsevier Mosby, Philadelphia 2005, pp 1685-93. 3. Al-Torbak A, Malak M, Teichmann K et al. Presumed stromal graft rejection after deep anterior lamellar keratoplasty. Cornea 2005;24: 241-3. 4. Watson SL, Tuft SJ, Dart JKG. Patterns of rejection after deep lamellar keratoplasty. Ophthalmology 2006; 113:556-60. 5. Offret G, Pouliquen Y (1974) Les homogreffes de la cornee. Masson etCie, Paris p 93. 6. Borderie VM, Werthel AL, Touzeau O et al. Comparison of techniques used for removing the recipient stroma in anterior lamellar keratoplasty. Arch Ophthalmol 2008;126:31-7. 7. Chen W, Lin Y, Zhang X et al. Comparison of fresh corneal tissue versus glycerin-cryopreserved corneal tissue in deep anterior lamellar keratoplasty. Invest Ophthalmol Vis Sci 2010; 51:775-81. 8. Feizi S, Javadi M, Jamali H et al. Deep anterior lamellar keratoplasty in patients with keratoconus: big-bubble technique. Cornea 2010: 29:177-182 9. Abdelkader A, Elewah EM, Kaufman HE. Confocal micrscopy of corneal wounds healing after deep 10. 11. 12. 13. 14. 15. 16. 17. lamellar keratoplasty in rabbits. Arch Ophthalmol 2010;128:75-80. Dua HS, Jayaswal R, Said DG.Stitched up: full thickness corneal grafts. Editorial. Br J Ophthalmol 2008;92:869-70. Khodadoust AA, Silverstein AM. The survival and rejection of epithelium in experimental corneal transplants. Invest Ophthalmol 1969;8:169-79. Tham VM, Abbot RI. Corneal graft rejection: recent updates. Int Ophthalmol Clin 2002;42:105-13. van Dooren BTH, Mulder PGH, Neuwendaal CP et al. Endothelial cell density after deep anterior lamellar keratoplasty (Melles technique). Am J Ophthalmol 2004; 137:397-400. Fontana L, Parente G, Tassinari G, etal.Clinical outcomes after deep lamellar keratoplasty using the big-bubble technique in patients with keratoconus. Am J Ophthalmol 2007;143:117-24. Sarnicola V, Toro P, Gentille D et al. Descemetic DALK and predescemetic DALK: outcomes in 236 cases of keratoconus. Cornea 2010;29:53-9. Edmonds CR, Wung SF, Pemberton B. Corneal endothelial cell count in keratoconus patients after contact lens wear. Eye Contact Lens 2004;30:54-8. Rieth S, Engel F, Buehner E et al. Comparison of data from the Rostock Cornea Module of the Heidelberg Retina Tomograph, the Oculus Pentacam, and the endothelial cell microscope. Cornea 2010; 29:314-20. EPIZODAO ODBACIVANJA STROME KALEMA POSLE DUBOKE PREDNJE LAMELARNE KERATOPLASTIKE (DALK) Ljubiša Nikolić*, Vesna Jovanović**, Slađana Delević* *Specijalna očna bolnica Oculus **Stomatološki fakultet Univerziteta u Beogradu, Klinika za očne bolesti “Prof. dr Ivan Stanković”, KBC “Zvezdara” Cilj: Prikaz neuobičajene komplikacije duboke prednje lamelarne keratoplastike kod keratokonusa. Metod: Pacijentu sa odmaklin keratokonuson urađena je duboka prednja lamelarna keratoplastika u nivou neposredno iznad Descemetove membrane. Kornealna topografija i debljina rožnjače određivane su Orbskenom. Broj endotelnih ćelija rožnjače određivan je pomoću konreralnog modula Roštok. 21 Acta Ophthalmologica 2015, 41(1) Rezultati: Epizoda odbacivanja strome javila se 14 meseci posle operacije. Pošto je reakcija zaustavljena, kalem je ponovo postao providan,ali sa samo 1449+19 ćelija na mm2. Zaključak: Duboka prednja lamelarna keratoplastika je bezbednija od perforativne, ali ni ova operacija nije bez komplikacija. Međutim, komplikacije se često mogu zbrinuti medikamentnim lečenjem. Učestalost epizoda odbacivanja verovatno može da se smanji pravovremenim uklanjanjem svih sutura. Acta Ophthalmologica 2015;41(1):18-22. Key words: DALK, keratokonus, odbacivanje Kontakt: Prof. dr Ljubiša Nikolić, Specijalna očna bolnica Oculus, 11000 Beograd, Bulevar Mihaila Pupina 10 E-mail:[email protected] 22