Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
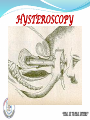
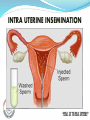
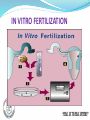
Presented by, Mrs.Kavitha Jasmine, Asst. Prof, Obstetrics & Gynecology Department, Annammal College Of Nursing, Kuzhithurai. Infertility is defined as a failure to conceive within one or more years of regular unprotected coitus. TYPES Primary Infertility Secondary Infertility PRIMARY INFERTILITY: It denotes those patients who have never conceived. SECONDARY INFERTILITY: It indicates previous pregnancy but failure to conceive subsequently. INCIDENCE Eighty percent of the couples achieve conception if they so desire,within one year of having regular intercourse with adequate frequency(4-5 times a week).Another 10 percent will achieve the objective by the end of second year.As such,10 percent remain infertile by the end of second year. CAUSES OF INFERTILITY MALE FACTORS Defective spermatogenesis Obstruction of efferent duct system. Failureto deposit sperm high in vagina. Errors in seminal fluid. FEMALE FACTORS Ovarian factor. Tubal & peritoneal factors. Uterine factors. Cervical factors. Vaginal factors. Combined factors. MALE REPRODUCTIVE SYSTEM DEFECTIVE SPERMATOGENESIS CONGENITAL FACTORS UNDESCENDED TESTES KARTARGENER SYNDROME HYPOSPADIAS THERMAL FACTORS INFECTION GENERAL FACTORS ENDOCRINE FACTORS GENETIC FACTORS IMMUNOLOGIC FACTORS CONGENITAL FACTORS: Undescended testes- The hormone secretion remains unaffected, but spermatogenesis is depressed.Vas deferens is absent in about 1-2 percent males. Kartagener syndrome- It is an autosomal disease in which there is loss of ciliary function and sperm motility. Hypospadiasis- Causes failure to deposit sperm high in vagina. THERMAL FACTOR: Scrotal temperature is raised in conditions such as varicocele,big hydrocele or filariasis. Other causes are using tight under garments or working in hot sun. In all these cases the depressed spermatogenesis may be temporary and reversible. INFECTION: Infections like mumps, bronchiectasis bacterial or viral infection of SEMINAL VESICLE OR PROSTATE depresses sperm count. GENERALFACTORS: Chronic diseases,malnutrition or heavy smoking reduce spermatogenesis.Alcohol also has the same effect. IATROGENIC: Radiation,cytotoxic drugs, nitrofurantoin,cimetidine, βblockers, anti hypertensives,anti convulsants and antidepressant drugs are likely to hinder spermatogenesis. OBSTRUCTION OF EFFERENT DUCTS The efferent ducts may be obstructed by infection like tubercular , gonococcal or by surgical trauma(herniorraphy) following vasectomy. FAILURE TO DEPOSIT SPERM HIGH IN VAGINA Ercetile dysfunction, Ejaculatory defectpremature ejaculation, retrograde or absence of ejaculation. Hypospadias: A developmental anomaly in the male in which the urethra opens on the underside of penis or in the perineum. ERRORS IN SEMINAL FLUID 1.Usually high or low volume of ejaculate. 2.Low fructose content. 3.High prostaglandin count. 4.Undue varicosity. DEFECTIVE SPERMATOGENESIS VARICOCELE OVARIAN FACTORS ANOVULATION OLIGOOVULATION LUTEAL PHASE DEFECT LUTEINISED UNRUPTURED FOLLICULAR SYNDROME ANOVULATION OR OLIGO-OVULATION: Ovarian function is likely to be linked with disturbed hypothalamopituitary-ovarian axis either primary or secondary from thyroid or adrenal dysfunction. Thus, the disturbance may result in anovulation, or even amenorrhoea.As there is no ovulation, there is no corpus luteum formation. LUTEAL PHASE DEFECT(LFD): In this condition there is inadequate growth and functioning of corpus luteum. There is inadequate progesterone secretion.The life span of corpus luteum is reduced to 10 days.As a result,there is inadequate secretory changes in the endometrium which hinders implantation Drug induced ovulation,decreased level of FSH and LH, elevated prolactin,subclinical hypothyroidism,older women,pelvic endometriosis,dysfunctional uterine bleeding are the important causes. LUTEINISE UNRUPTURED FOLLICULAR SYNDROME (trappedovum): In this condition the ovum is trapped inside the follicle which gets luteinized.The causes may be associated with pelvic endometriosis or with hyperprolactineamia. CERVICAL FACTORS OVARIAN & TUBAL FACTORS Tubal factors: Are responsible for about 30-40 percent cases of female infertility. It is due to obstruction in the tube due to; 1.Peritubal adhesions 2.Endosalpingeal damage 3.Previous tubal surgery or sterilization 4.Salpingitis 5.Tubal endometriosis 6.Polyps or mucous debris in the tubal lumen 7.Tubal spasm Peritoneal causes: Minimal endometriosis, dyspareunia, abnormal peritoneal fluid are the peritoneal factors. Uterine factors: The endometrium must be sufficiently receptive enough for effective nidation and growth of fertilized ovum.The possible factors that hinders nidation are:1.Uterine hypoplasia 2.Inadequate secretory endometrium 3.Fibroid uterus 4.Congenital malformation of the uterus Cervical factors: Congenital elongation of cervix,second degree uterine prolapse,acute retroverted uterus,abnormal composition of cervical mucous. Vaginal factors: It includes; 1.Atresia vagina 2.Transevrse vaginal septum 3. Septate vagina 4. Narrow introitus COMBINED FACTORS Apareunia And Dyspareunia Anxiety And Apprehension Use Of Lubricants During Intercourse Which Are Spermicidal Immunologic Factors Combined factors: These include the presence of factors both in male and female partners causing infertility. General factors: Advanced age of wife beyond 35 is related but spermatogenesis continues throughout life although ageing reduces the fertility in males. Infrequent intercourse, lack of knowledge of coital technique and timing of coitus to utilize the fertile period are common even among the literate couples. Apareunia and dyspareunia Anxiety and apprehension Use of lubricants during intercourse which may be spermicidal. INVESTIGATIONS OF INFERTILITY OBJECTIVES ; 1.To detect the etiological factors. 2.To rectify the abnormality in an attempt to improve the fertility. 3.To give assurance with explanation to the couples, if no abnormality is detected. INVESTIGATION IN MALES History collection: Age, duration of marriage,history of previous marriage,and proven fertility if any,are to be noted. A general medical history should be taken with special reference to sexually transmitted diseases,mumps orchitis after puberty, diabetes,& recurrent chest infection. Relevant surgeries such as herniorrhaphy, surgeries on testes or genital area are to be enquired. Occupational history should be directed towards exposure to excessive heat or radiation.Social habits,particularly heavy smoking and alcohol is to be collected. Examination: •A full physical examination is to be performed to determine the general health condition. •Examination of reproductive system includes inspection and palpation of genitalia. •Presence of varicocele should be elicited in upright position. VARICOCELE A.Routine Investigations include urine and blood examination including postprandial sugar. B.Seminal Fluid Analysis: This should be the first step in investigation because if some gross are detected like absence of sperm,the couple should be counselled for the need of assisted reproductive therapy. C.Collection: Collection of semen is done by masturbation failing which by coitus interruptus.The semen is collected in a clean wide mouthed jar.The sample must be send to lab as early as possible so that examination is conducted witnin 2 hours. INDEPTH EVALUATION: These are needed for the cases of –a)Azoospermia b)Oligospermia c)Low volume ejaculate d)Problems of sexual potency etc. .SERUM FSH,LH, TESTOSTERONE,PROLACTIN & TSH: Testicular hypogonadotropic hypogonadism.Elevated prolactin due to pituitary adenoma may cause impotency. .FRUCTOSE CONTENT IN SEMINAL FLUID: Its absence suggest congenital absence of seminal vesicle or portion of ductal system or both. .TESTICULAR BIOPSY: It is done to differentiate primary testicular failure from obstruction as a course of azoospermia or severe oligospermia.The biopsy material is to be sent in Bouin’s solution. Transrectal Ultrasound(TRUS): is done to visualize the seminal vesicles, prostate and ejaculatory duct obstruction. Indications of TRUS are-Azoospermia or oligospermia, abnormal digital examination, ejaculatory duct abnormality and genital abnormality like hypospadias. Vasogram: is a radiographic study done to evaluate the ejaculatory duct obstruction.It is mostly replaced by TRUS. karyotype analysis: This is done in case with azoospermia or severe oligospermia and raised FSH.Klinefelter’s syndrome (XXY) is the commonest. VASOGRAM INVESTIGATION IN FEMALES HISTORY COLLECTION EXAMINATIONS SPECIAL INVESTIGATIONS -INDIRECT DIAGNOSIS OF OVULATION -DIRECT DIAGNOSIS OF OVULATION DIAGNOSIS OF OVULATION 1.Direct method 2.Indirect method Indirect method includes collection of menstrual history, Basal body temperature, Cervical mucous study,endometrial pH and hormone study. Directmethod includes Laparoscopy Dilatation & Insufflation Test Hysterosalphingography Laparoscopy &Chromopertubation Sonohysterosalphingography LAPAROSCOPY; Laparoscopic visualization of recent corpus luteum or detection of ovum from the aspirated peritoneal fluid from the pouch of douglas is the only direct evidence of ovulation. The scope of diagnostic laparoscopy has been widened.It is an invasive investigation,so this is done after male factor and ovulatory functions have been fonud normal or corrected. The indications of its use are; a.Abnormal HSG findings. b.Failure to conceive after reasonable period(6 months) even with normal HSG. c.Unexplained infertility. d.Age above 35 years. INDICATIONS FOR LAPAROSCOPY IN INFERTILITY Diagnostic - Age above 35 years. - Abnormal HSG. - Failure to conceive after reasonable period with normal HSG. - Unexplained infertility. Operative Gift & Zift Procedures. -Ovarian diathermy -Reconstructive tubal surgery. - Fulguration of endometriotic implants. PROTOCOLS: A double puncture technique is to be applied.All the pelvic organs are to be properly visualized,of particular importance is to note the fimbrial end of fallopian tubes and their relation with the ovaries.Proper documentation with the aid of diagram is mandatory. Advantages Over Hsg: It can precisely diagnose peritubal adhesions,pelvic endometriosis or evidence of ovulation.Chromopertubation with methylene blue cannot only reveal patency of the tube but the nature of tubal motility. Drawbacks: It is more invasive than HSG.It cannot detect abnormality in the uterine cavity or lumen of tube. When to be done? It is preferably done in the secretory phase.Recent corpus luteum may be visualized and endometrial biopsy can be taken in the same setting. LAPAROSCOPY LAPAROSCOPY INSTUMENTS USED IN LAPAROSCOPY DILATATIONAND INSUFFLATION TEST(RUBIN’S TEST) Principle: The underlying principle lies with the fact that cervical canal is in continuity with the peritoneal cavity through the tubes.As such entry of air or CO2 into the peritoneal cavity when pushed transcervically under pressure gives evidence of tubal patency. When to be done? It should be done in the post menstrual phase atleast 2 days stopping of menstrual bleeding. LIMITATION: It should not be done in the presence of pelvic infection. OBSERVATIONS: The patency of the tube is confirmed by: 1.Fall in pressure when raised above 120mm hg. 2.Hissing sound heard on auscultation on eithr iliac fossa. 3.Shoulder pain experienced by the patient. Drawbacks: In about one third of cases it gives a false negative findings due to corneal spasm.It also cannot identify the side and site of block in the tube. HYSTEROSALPINGOGRAPHY HYSTEROSALPHINGOGRAPHY Principle: The principle is sams as that of insufflation test,instead of air or CO2,dye is instilled transcervically. When to be done? 2 days after stopping of menstrual bleeding. Advantages: It has got many advantages over insufflations test.It can precisely detect the side and site of block in the tube.It can reveal any abnormality in the uterus like congenital anomalies,fibroid etc. HYSTEROSCOPY CHROMOPERTUBATION SONOHYSTEROSALPHINGOGRAPHY Normal saline is pushed within the uterine cavity with a paediatric Foley catheter.The catheter balloon is inflated at the level of cervix to prevent fluid leak.USG of the uterus and fallopie tube is done.Ultrasound can follow the fluid through the tubes up to the peritoneal cavity and in the pouch of Douglas. Advantages: It is a non-invasive method . It can detect uterine abnormality and polyps. Tubal Pathology could be detected. There is no radiation exposture. PREVENTION OF INFERTILITY Assurance To The Couples Body Weight Should Be Adequate Smoking & Alcoholism Is Prevented Managing Coital Problems 1.ASSURANCE: The infertile couples remains psychologically disturbed right from the beginning, more so as the investigations proceeds.The couple in such cases should be tactfully handled to minimize psychologic upset. When minor defects are detected in both the husband and the wife,each of which alone could not cause infertility but in combination,they significantly reduce the fertility potential.As such,the faults should be treated simultaneously and not one afer the other. 2.BODY WEIGHT: Overweight or underweight of any partner should be adequately dealt with to obtain an optimal weight.Body mass of index of 20-24 is optimum. 3.SMOKING AND ALCOHOL: Excess smoking or alcohol consumption is to be avoided. 4.COITAL PROBLEMS: The coital problems must be carefully evaluated by intelligent interrogation.Advice to have intercourse during the midcycle too often gives a result early enough even prior to investigation.Using LH test kit,one can detect LH surge in urine by getting a deep blue colour of dipstick.The test should be performed daily between day 12 to day 16 of a regular cycle.Timed intercourse over24-36 hours after the colour change reasonably succeeds in conception.Minor psychosexual problems should be corrected accordingly. TREATMENT OF MALE INFERTILITY The treatment of male is indicated in: 1.Extreme oligospermia 2.Azoospermia 3.Low volume ejaculate 4.Impotency GENERAL MEASURES: Reduction of weight in obese. Avoidance of alchohol and heavy smoking. Avoidance of tight and warm undergarments. Avoidance of occupation that may elevate testicular temperature. Use of vitamins E,C,D,B12 and folic acid as antioxidants to improve spermatogenesis. Medications that interfere with spermatogenesis must be avoided like nitrofurantoin,cimetidine,antihypertensives,anti convulsants & anyidepressants. SURGICAL MEASURES When the patient is found to be azoospermic and yet testicular biopsy shows normal spermatogenesis, obstruction of vas must be suspected. This should be corrected by microsurgery-Vaso Epididymostomy or Vasovasostomy. The presence of varicocele is corrected by high ligation of spermatic vein and the hydrocele by surgey. Orchidopexy in undescended testes should be done between 2-3 years of age to have adequate spermatogenesis in later life. IMPOTENCY Psychosexual treatment may be of help Hyper prolactinaemia needs further investigation and treatment.For erectile dysfunction SILDENAFIL (25-100 mg) or TADALAFIL(10-20mg) is currently advised. A single dose is given orally one hour before sexual activity.In unresponsive cases,artificial insemination is to be adopted. ASSISTED REPRODUCTIVE TECHNOLOGY (ART) (FOR MALE INFERTILITY) Prospect of male infertility has improved significantly with the treatment available for infertile males. MANAGEMENT OF FEMALE INFERTILITY GENERAL MEASURES PHARMACOLOGICAL MANAGEMENT SURGICAL MANAGEMENT TREATMENT FOR ANOVULATION Anovulation is a common factor for female infertility. It may be present in otherwise normal menstrual cycle or may be associated with oligomenorrhoea or amenorrhoea. INDUCTION OF OVULATION 1.General Measures 2.Pharmacological Management 3.Surgical Management GENERAL MEASURES: -Psychotherapy to improve the emotional stability. -Reduction of weight in obesity as in PCOS cases is essential to have a good response of drug therapy in induction of ovulation. PHARMACOLOGICAL MANAGEMENT: 1.CLOMIPHENE CITRATE: Patient selection: Normogonadotrophic-normoprolactinaemic patients who are having normal cycles with absent or infrequent ovulation. PCOS cases with oligomennorhoea or amenorrhoea Hypothalamic amenorrhoea following stress or using oral contraceptive pills. Dose: Clomiphene citrate is simple,safe and at the same time costeffective.Initial dose of 50mg daily.Dose can be increased to a maximum of 250 mg daily if ovulation is not induced by lower dose.The actual starting day of its administration in the follicular phase varies between day 2 and day5 and therapy is given for 5 days.Ovulation is expected to occur about 5-7 days after the last day of therapy.Therapy for 6 cycle is generally given Mechanism of action of clomiphene citrate: Clomiphene citrate is an anti-oestogenic drug.It blocks the oestrogen receptors of hypothalamus.This results in increased GnRH pulse amplitude causing increased gonadotropin secretion from the pituitary. Side effects: 1.Hot flushes 2.Nausea 3.Vomiting 4.Headache 5.Visual disturbances 6.Ovarian hyperstimulation Couple Instructions: The couple is adviced to have sexual intercourse as per following guidelines: Daily or on alternative days beginning 5-7days after the last dose of clomiphene therapy. Several times for 24-48 hours after the colour change in urine when tested by LH kit. Number of times over 24-36 following hCG administration. 2.GONADOTROPHINS: Indications: Hypogonadotrophic hypogonadism Clomiphene failed or resistant cases Unexplained infertility Dose schedule: Dose schedule starts with a minimal dose of 75 IU IM/day. Follicular stimulation is started at any time from 2-5 days of the cycle and is continued for 7-10 days depending on the response. Follicular growth is monitored with serum estradiol estimation and follicular number and size are measured by transvaginal sonography. Serum oestradiol level of 500-1500 pg/ml and maximum follicular diameter of 18-20mm are optimum. When this optimum level is obtained,5000-10000IU of hCG is administered IM to induce ovulation. Ovulation is expected to occur approximately 36 hours after hCG administration. Side effects therapy: of gonadotrophin Primary ovulation failure with raised serum FSH. Uncontrolled thyroid and adrenal dysfunction. Sex hormone dependent tumour in the body. SURGICAL MANAGEMENT Laparoscopic Ovarian Drilling Wedge Resection Surgery Of Pituitary Prolactinomas Surgical Removal Of Ovarian And Adrenal Tumours Tubal Surgery 1.Laproscopic ovarian drilling(LOD) or laser vapourisation: This is done by multiple puncture of the cysts in polycystic ovarian syndrome by diathermy or laser.It reduces systemic and intraovarian androgen levels.This procedure is helpful in clomiphene resistant,hyperandrogenic anovulatory women.The woman ovulates spontaneously following LOD. 2.Wedge resection: This is not commonly done these days. Bilateral wedge resection of the ovaries is done in PCOS cases where clomiphene citrate fails to induce ovulation.It induces adhesions. 3.Surgery for pituitary prolactinomas. 4.Surgical removal of virilising or other functioning ovarian or adrenal tumours. 5.Tubal surgery TUBAL SURGERY Indications for tubal surgery: 1.Peritubal adhesions 2.Proximal tubal block 3.Distal tubal block 4.Mid tubal block Guidelines for tubal surgery: Tubal surgery may be considered in young women after previous tubal sterilization or in women with mild disease at the distal tubal segment. Tubal surgery may be tried for mild proximal tubal block. Preoperative assessment and planning for surgery has to be done by HSG or laparoscopy. Prior counseling of the couples about the hazards of surgery and prospect of future pregnancy should be done. IVF is considered as the best treatment option for any complicated tubal occlusive disease. Salphingectomy should be done before IVF when hydrosalpines are present. Methods of tubal surgery: Tuboplasty is the name given to finer surgery on the tubes to restore the anatomy and physiology as far as practicable. The operation can be done by conventional methods or by microsurgical techniques which may be employed following laparotomy. Microsurgical techniques gives better results due to minimal tissue handling and damage,perfect haemostasis and minimal adhesions. TUBOPLASTY OPERATIONS Salphingo-ovariolysis Separation or division of adhesions. Fimbrioplasty Separation of fimbrial adhesions to open up the abdominal ostium. Salphingostomy Creates a new opening in the completely occluded tube.It is called terminal or cuff at the abdominal ostium. Tubotubal Anastomosis When the segment of the diseased tube is resected following tubectomy,an end to end anastomosis is done. Tubocornual Anastomosis When there is corneal block, the remaining healthy tube is anastomosed to the patent interstitial part of the tube. ADJUVANT THERAPY Adjuvant procedures to improve the result of tubal surgery include prophylactic antibiotics,use of adhesion prevention devices(intercede,seprafilm) and postoperative hydrotubation. Hydrotubation: Hydrotubation is the procedure to flush the tubal lumen by medicated fluids passed transcervically through a cannula. The fluid contains antibiotics and hydrocortisone(Gentamicin-80mg and dexamethasone 4mg in 10ml distilled water). It should be done in postmenstrual phase. SALPHINGO OVARIOLYSIS TUBO TUBAL ANASTOMOSIS TUBOCORNUAL ANASTOMOSIS ARTIFICIAL INSEMINATION 1.IUI- Intrauterine Insemination 2.Fallopian Tube Sperm Perfusion 1.INTRA UTERINE INSEMINATION IUI may be either AIH(artificial insemination husband) or AID(artificial insemination donor).Husband’s sperm is commonly used.The purpose of IUI is to bypass the endocervical canal which is abnormal and to place increased concentration of mobile sperms as close to the fallopian tubes. INDICATIONS FOR IUI: 1.Hostile cervical sperm 2.Cervical stenosis 3.Oligospermia 4.Immune factor (Male & Female) 5.Male factor-impotency or anatomical defects 6.Unexplained infertility Washing,centrifuge and swim-up methods are commonly used.About 0.3ml of washed and concentrated sperm is injected through a flexible polyethylene catheter within the uterine cavity around the time of ovulation.Washing in culture media removes the proteins and prostaglandins from the semen that may cause uterine cramps or anaphylactic reactions. The processed motile sperm for insemination should be atleast 1 million. Fertilizing capacity of spermatozoa is 24-48 hours. The procedure may be repeated 2-3 times over a period of 2-3 days. TIMING OF IUI: Spontaneous cycles: IUI likely on day 12 and 14. Clomiphene Citrate induced cycles: IUI at 5-7 days after completion of cycles. Urinary LH detection: IUI done in 24 hours after colour change. COLLECTION OF SEMEN FOR IUI: 1.The total number of days since last ejaculation should be no longer than 4-5 days.Sperm cells are made and replaced rapidly after each ejaculation. 2.Collect the semen using sterile techniques.Bacterias that are normally found in the skin can contaminate the specimen. 3.Masturbation is the preferred method of collection.It ensures the cleanest possible sample. 4.Donot have intercourse for 2-3 days before the day of collection. 5.Your appointment of sperm collection will be 70-90 minutes before the insemination. 7.The specimen must reach the lab within 30 minutes after collection of specimen. 8.Only containers distributed by the ANDROLOGY LABORATORY must be used for collection. PREPARATION FOR IUI: 1.PREPARING THE SEMEN SAMPLE: The semen should be washed in a way that separates a highly active normal sperm from lower quality sperm. 2.MONITORING FOR OVULATION: Ovulation can be calculated using basal body temperature,LH kits and trans vaginal ultrasound. 3.DETERMINIG OPTIMAL TIMING: Most IUIs are done after one or two days of detecting ovulation. ADVANTAGES OF IUI: IUI is the least invasive,effective,simple,cheap and first line assisted conception treatment method for infertility couples. Woman’s cervicel mucus can sometimes kill the sperm,preventing the sperm from reaching the egg.Here IUI is the effective method. IUI helps to deliver much more motile sperms to the fallopian tubes at the critical times around ovulation. IUI is cost effective and simplest method in advanced infertility treatment. DISADVANTAGES OF IUI: High risk of generating OHSS-Ovarian Hyper Stimulation Syndrome. Stimulated ovarian cycle in IUI can cause multiple pregnancy. Ovarian cysts as the side effect of stimulated ovarian cycle. Possibility of using wrong semen samples. Noninfective salphingitis and allergic rection can occur. 70-80 percent chance for abortion or ectopic pregnancy. AFTER CARE OF IUI: Patient should be kept in Foot end elevated position after the procedure. She should be adviced to take rest for 10-20 minutes following the procedure. Vital signs should be monitored immediately after the procedure. Complete bedrest for 4-5 days after IUI. No exercise exept light walking for 2 weeks after IUI. Intake lot of protein rich foods like eggs,soya,chicken products ie atleast 75gm of protein per day. Keep a positive frame of mind and pray to GOD to help you at this time. After IUI,keep your stomach coverted and protected from wind for atleast 2 weeks since the womb needs to stay warm to aid conception. INTRA UTERINE INSEMINATION INDICATIONS OF IUI Hostile Cervical Sperm Cervical Stenosis • Oligospermia Immune Factor Male Impotency And Anatomical Defects Unexplained Infertility ASSISTED REPRODUCTIVE TECHNOLOGY(ART) ART encompasses all the procedures that involve manipulation of gamates and embryos outside the body for the treatment of infertility. PRINCIPAL STEPS IN ART REGULATION USING Gnrh AGONIST. Controlled Ovarian Hyperstimulation. Monitoring Of Follicular Growth. Oocyte Retrieval. Fertilization Invitro. Transfer Of Gamrates Or Embryo. Luteal Support With Progesterone. DIFFERENT METHODS OFART: IVF-ET: In Vitro Fertilisation and Embryo Transfer GIFT: Gamate Intra Fallopian Transfer ZIFT: Zygote Intra Fallopian Transfer POST: Peritoneal Oozyte & Sperm Transfer SUZI: Subzonal Insemination ICSI: Intra Cytoplasmic Sperm Injection INVITRO FERTILISATION AND EMBRYO TRANSFER(IVF-ET) The field of reproductive medicine has changed for ever with the birth of Louise Brown in 1978 by IVF-ET.Patrick Steptoe and Robert Edwards of England are remembered for their revolutionary work. INDICATIONS OF IVF: Tubal disease Unexplained infertility Endometriosis Male factor infertility Cervical hostility Failed ovulation induction Ovarian failure Woman with normal ovaries but no functional uterus. Woman with genetic risk PATIENT SELECTION: Age less than 35 years. Presence of ovarian reserve (serum FSH < 10 IU/L) Husband –normal seminogram Couple must be screen negative for HIV and hepatitis. Normal uterine cavity as evaluated by hystreroscopy. PRINCIPAL STEPS OF AN ART CYCLE: 1.Regulation using GnRH agonist. 2.Controlled ovarian hyperstimulation. 3.Monitoring of follicular growth. 4.Oocyte retrieval. 5.Fertilisation invitro (IVF,ICSI GIFT) 6.Transfer of gamates or embryos. 7.Luteal support with progesterone. IN VITRO FERTILIZATION IVF-ET TEST TUBE BABY-DISAMBIGUATION GAMATE INTRA FALLOPIAN TRANSFER-(GIFT) GAMATE INTRA FALLOPIAN TRANSFER GIFT was described by Asch and colleagues in 1984. It is a more invasive and expensive procedure than IVF but the result seems better than IVF.In this procedure both sperm and unfertilized oocyte are transferred into fallopian tubes.Fertilisation is then achieved in vivo. GIFT ZYGOTE INTRA FALLOPIAN TRANSFER ZIFT was first described by Devroey et al, in 1986. The placement of the zygote (following one day of in vitro fertilization) into the fallopian tube can be done either through the abdominal ostium by laparoscopy or through the uterine ostium under ultrasonic guidance. This technique is a suitable alternative of GIFT when defect lies in the male factor or in cases of failed GIFT. ZIFT ZIFT INTRA CYTOPLASMIC SPERM INJECTION ICSI was first described by Van Steirteghem and colleagues in 1992. Indications: 1.Severe oligospermia (less than 5million sperm/ml) 2.Presence of sperm antibodies 3.Obstruction of efferent duct system 4.Congenital absence of vas 5.Failure of fertilization in IVF Technique: One single spermotozoan or even a spermatid is injected directly into the cytoplasm of an oocyte by miropuncture of the zona pellucida.This procedure is carried out under a high quality inverted operating microscope Micropipette is used to hold the oocyte while the spermatozoan is deposited inside the ooplasm by an injecting pipette. INTRA CYTOPLASMIC SPERM INJECTION INTRA CYTOPLASMIC SPERM INJECTION HAZARDS OF ART Most of the ART are associated with increased chromosomal abnormalities of the offsprings. Increased number of pregnancy loss,multiple pregnancy and ectopic pregnancy have been observed. Perinatal mortality and morbidity are high. Psychological stress and anxiety of the couple are severe. Role Of Nurse Midwife In Infertility Management Nurse midwife comes from a variety of training backgrounds,but the vasy majority have previous experience in women’s health care. Nurses have to work diligently to help the specialist execute treatment plans and play an important role in supporting the patients through the complex journey of infertility treatment. The nurse will aid the patient in scheduling various investigations like Ovarian reserve testing ,Hysterosalphingogram, & Semen analysis.Infertility testing and treatment involves specific timing aroumd the menstrual cycle.For some patients this may be unpredictable,So it requires efficient and effective action from the nurse. The nurse have to instruct the couples about schedules far taking the medicines.Should provide teaching on self subcutaneous and intramuscular injection.For many patients this is the first time they have had to give self injections.Nurses do an outstanding job at making sure thattreatment plans are effectively delivered. The diagnosis and treatment of infertility involves significant stress that is comparable to being diagnosed with cancer.Added to this stress is the cost of the treatment.In the end an empathetic nursing team will work under stressful condition to ensure that patients are compassionately and effectively cared for.