Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Coronary artery disease wikipedia , lookup
Baker Heart and Diabetes Institute wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
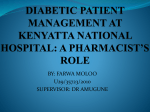
The European Journal of Heart Failure 8 (2006) 2 – 6 www.elsevier.com/locate/heafai Impaired left ventricular relaxation in type 2 diabetic rats is related to myocardial accumulation of N q-(carboxymethyl)lysine Stefan Schäfer*, Jochen Huber, Cornelia Wihler, Hartmut Rütten, Andreas E. Busch, Wolfgang Linz Therapeutic Department Cardiovascular Diseases, Aventis Pharma Deutschland GmbH, Building H 821, D-65926, Frankfurt am Main, Germany Received 2 February 2005; accepted 27 April 2005 Available online 8 August 2005 Abstract Myocardial dysfunction in the absence of myocardial ischemia is frequent in patients with diabetes mellitus but the underlying pathomechanism is unclear. We investigated whether accumulation of advanced glycation end products (AGEs) in the diabetic myocardium is related to its functional abnormalities. In 11 male homozygous Zucker diabetic fatty rats (ZDF/Gmi-fa/fa) aged 37 weeks (OBESE) and 11 non-obese, non-diabetic littermates (LEAN), we measured left ventricular function (pressure – volume catheter) and levels of N q-(carboxymethyl)lysine (CML), a prototypical AGE, in serum and the left ventricle (competitive enzyme linked immuno-assay). Overt diabetes mellitus (HbA1c > 9%) was present in all OBESE animals but not in LEAN. Systolic left ventricular function was not different between the groups, but the markers of left ventricular relaxation, dP / dt min and the relaxation constant s, were impaired in OBESE. In parallel, CML levels were increased in serum (273 T 15 vs. 197 T 10 ng/ml, p < 0.05) and in the left ventricle (18.4 T 1.1 vs. 12.5 T 2.0 ng/mg protein, p < 0.05) in OBESE compared to LEAN. There was a linear correlation between s and the left ventricular CML levels (r = 0.65; p < 0.05). We conclude that type 2 diabetes is associated with predominant left ventricular diastolic dysfunction. Myocardial accumulation of advanced glycation end products may contribute to relaxation abnormalities in type 2 diabetes. D 2005 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. Keywords: Zucker diabetic fatty rat; Diabetic cardiomyopathy; Advanced glycation end products 1. Introduction Diabetes mellitus is a risk factor for heart failure. Although a large proportion of the excess risk of heart failure in diabetic individuals can be attributed to coronary artery disease and its myocardial complications, several studies have indicated the existence of a nonischaemic, specific ‘‘diabetic cardiomyopathy’’. A recent survey in the US has revealed an independent association between diabetes and nonischaemic cardiomyopathy [1]. Based on the perturbations of glucose and lipid metabolism occurring * Corresponding author. Tel.: +49 69 30513391; fax: +49 69 30516394. E-mail address: [email protected] (S. Schäfer). in diabetes, a number of functional and morphological changes have been identified within the myocardium which may lead to heart failure in diabetic patients in the absence of coronary artery disease [2]. Chronic hyperglycaemia promotes the glycation of proteins, which may directly impair function and structure of the myocardium. In addition, the formation of advanced glycation end products (AGEs) can modulate myocardial function via activation of specific receptors (eg., RAGE) [3]. N q-(carboxymethyl)lysine (CML) is a prototypical AGE, which is derived from oxidative modification of glycated proteins. Serum levels of CML and other AGEs are increased in patients with type 2 diabetes [4], and accumulation of CML has been reported in the myocardium from diabetic patients [5]. In type 1 diabetic patients, serum levels of AGEs have been 1388-9842/$ - see front matter D 2005 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.ejheart.2005.04.011 S. Schäfer et al. / The European Journal of Heart Failure 8 (2006) 2 – 6 correlated to left ventricular (LV) diastolic dysfunction [6]. In rats with streptozotocin-induced, type 1 like diabetes, myocardial compliance was linked to myocardial collagen AGEs [7]. Aminoguanidine, an inhibitor of AGE formation, prevented both myocardial AGE fluorescence and LV stiffness in this model [7]. Interestingly, the role of AGEs for myocardial function in type 2 diabetes has received little attention despite the obvious differences between the two types of diabetes. Hyperinsulinaemia, obesity, and hyperlipidaemia may modulate the metabolism of AGEs and myocardial function independently. In the present study, we therefore investigated whether there is a link between myocardial function and AGE accumulation in type 2 diabetes. 2. Methods The animal experiments were performed in accordance with current Sanofi-Aventis Laboratory Animal Science and Welfare guidelines and the German law for the protection of animals. 2.1. Animals Eleven male Zucker diabetic fatty rats (ZDF/Gmi-fa/fa) and eleven heterozygous (ZDF/Gmi-+/fa) lean littermates were purchased from Charles River Germany GmbH (Sulzfeld, Germany) and kept in our local facilities in Frankfurt-Hoechst. The animals were housed individually in standard cages and received a standard chow diet (standard diet #1320, Altromin, Lage, Germany) and tap water ad libitum. Metabolic characterization was performed at age 10, 17, 27, and 37 weeks in haemolysate which was taken from the retro-orbital plexus under light anesthesia (3.5 vol.% isoflurane in 34/66 N2O/O2). Glycated haemoglobin (HbA1c) was measured in these samples using a standard kit (Cobas Integra, Roche diagnostics, Mannheim, Germany). 2.2. In vivo experiments At age 37 weeks, the animals were anaesthetized with thiopental (Narcoren, 100 mg kg 1 i.p., Merial, Hallbergmoos, Germany), intubated and artificially ventilated. For the assessment of pressure – volume relationships, the left 3 ventricle was catheterized retrogradely via the right carotid artery using a 1.4 F impedance-micromanometer catheter (Millar Instruments, Houston, Texas, USA). In brief, the method is based on measuring the time-varying electrical conductance signal of two segments of blood in the left ventricle, from which total volume is calculated. Raw conductance volumes were corrected for parallel conductance by the hypertonic saline dilution method. For absolute volume measurements, the catheter was calibrated with known volumes of heparin treated rat blood. Pressure – volume signals were recorded at steady-state and during transient preload reduction achieved by vena cava occlusion. Data were digitized with a sampling rate of 1000 Hz and recorded on a PC using specialized software (HEM, Notocord, Croissy, France). For subsequent analysis of pressure – volume loops, preload recruitable stroke work (PRSW), end-systolic pressure volume relationship (Ees), and end-diastolic pressure volume relationship (EDPVR), PVAN software (Millar Instruments, INC, Houston, Texas) was used. Specifically, LV systolic pressure (LVSP), LV dP / dt max, ejection fraction, cardiac output, the end systolic myocardial elastance constant Ees, and preload recruitable stoke work (PRSW) were determined as measurements of systolic LV performance. LV end diastolic pressure (LVEDP), LV end diastolic volume (LVEDV), and the slope of the end-diastolic pressure volume relationship (EDPVR) were determined as parameters primarily reflecting LV compliance. As measures of LV relaxation, LVdP/dtmin and the time constant of LV pressure decay (s, calculated according to Weisfeldt et al. [8]) were determined. After completion of haemodynamic measurements, the animals were sacrificed by quick excision of the hearts under continuing deep anaesthesia. 2.3. Measurement of CML CML was determined in serum and heart homogenates with a competitive enzyme-linked immunosorbent assay (ELISA) using a CML monoclonal antibody as described previously [9]. Heart samples were immediately frozen in liquid nitrogen and ground for 5 min in liquid nitrogen using a Freezer mill 6750 (C3 Analysetechnik GmbH, Haar, Germany). From the frozen organ powder, 10 mg were dissolved in 1 ml PBS buffer pH 7.4 containing 0.5 g/l Tween-20, 0.5 mM phenylmethanesulfonyl fluoride (Sigma- Table 1 Biometric and carboxy-methyl-lysine (CML) data LEAN OBESE Age 22 weeks 37 weeks 22 weeks 37 weeks Body weight (g) Heart weight (g) Heart / body weight ratio Serum CML content (ng/ml) Heart CML content (ng/mg protein) 404 T 24 462 T 17 396 T 11 373 T 14* 0.80 T 0.02 0.91 T 0.03 0.89 T 0.04 0.73 T 0.01* 0.20 T 0.01 0.20 T 0.01 0.22 T 0.01 0.20 T 0.01 249.7 T 12.8 197.4 T 9.6 279.4 T 20.2 273.3 T 14.7* 15.9 T 1.3 12.5 T 2.0 23.8 T 1.0* 18.4 T 1.1* N = 8 – 10, except for CML data at age 22 weeks (where n = 4). Data are mean T SEM. *p < 0.05 vs. respective LEAN. 4 S. Schäfer et al. / The European Journal of Heart Failure 8 (2006) 2 – 6 22 Table 3 Diastolic left ventricular haemodynamic parameters at age 37 weeks 20 τ, ms 18 16 LEAN OBESE 14 LVEDP (mmHg) LVEDV (Al) EDPVR (mmHg/ml) 5.1 T 0.6 4.8 T 0.4 312 T 61 317 T 36 22 T 5 16 T 2 LV dP / dt min (mmHg/s) 5932 T 504 4383 T 390* s (ms) 13.8 T 0.7 17.1 T 0.6* N = 8 – 10. Data are mean T SEM. *p < 0.05 vs. LEAN. LVEDV, LV end diastolic volume; EDPVR, slope of the (linear) end diastolic pressure – volume relationship; s, constant of LV pressure decay. 12 10 10 15 20 25 30 (OBESE) animals weighed less than their non-diabetic (LEAN) littermates. The lesser body weight in the homozygous compared to heterozygous Zucker diabetic fatty rats at an older age is a common finding, which is probably due to an excessive loss of calories (glucosuria, proteinuria), which cannot be compensated for by an increased food intake. Absolute heart weight was also less in OBESE compared to LEAN, but heart-to-body weight ratios were identical in both groups (Table 1). Blood HbA1c was 6.1 T 0.2%, 10.0 T 0.4%, 8.7 T 0.4%, and 10.1 T 0.3% in OBESE at age 10, 17, 27, and 37 weeks respectively, indicating long lasting diabetes mellitus. In LEAN, by contrast, HbA1c remained below 5 percent at all time points. Myocardial CML, ng/mg protein Fig. 1. Scatterplot illustrating the significant linear relationship between myocardial CML levels and the LV relaxation constant s in LEAN and OBESE rats (r = 0.65, p < 0.05). CML, N q-(carboxymethyl)lysine. Aldrich Chemie GmbH, Steinheim, Germany) and 1 Ag/Al aprotinin (Roche Diagnostics, Mannheim, Germany). Samples were vortexed and sonicated (Sonoplus HD 2070, Bandolin, Berlin, Germany) twice for five seconds to disintegrate cells. Cell debris was removed by centrifugation. The heart lysates were adjusted to a concentration of 1 mg/ml total protein and 50 Al lysate was used for the CMLELISA. Serum samples were digested with 2 mg/ml proteinase K (Roche Diagnostics) for 3 h at 37 -C to liberate CML epitopes. To stop the reaction, 4 mM phenylmethanesulfonyl fluoride was added and the mixture was incubated for 30 min at 37 -C. Digested serum samples were measured in triplicate (50 Al each). CML contents in serum and plasma were also determined in a subset of n = 4 animals per group, which were sacrificed for an interim analysis at age 22 weeks. 3.2. CML At the interim analysis at age 22 weeks, there were no differences in serum CML between the two groups, but myocardial CML content was higher in OBESE (Table 1). At the final analysis (age 37 weeks), both serum and myocardial CML contents were higher in OBESE compared to LEAN (Table 1). There was a linear correlation between myocardial CML content and the relaxation parameters s (cf. Fig. 1) and dP / dt min (r = 0.43, p < 0.05), but not between serum CML content and s or dP / dt min (each p > 0.1). Also, there were no significant correlations between CML and the indices of systolic or myocardial compliance function (data not shown). 2.4. Statistics Data are given as mean T SEM. Differences were tested for significance using unpaired two-sided t-tests. A p value of less than five percent was considered significant. 3. Results 3.3. Haemodynamics 3.1. Biometric and metabolic data Haemodynamic parameters at age 37 weeks are summarized in Tables 2 and 3. In OBESE, heart rate was lower than in LEAN. Indices of the LV systolic function were not different between the two groups, including LV dP / dt max, and the load independent indices, Ees and PRSW. In The biometric data are summarized in Table 1. At the interim analysis (age 22 weeks), there were no differences between groups regarding body weight, heart weight, or heart-to-body weight ratio. At age 37 weeks, the diabetic Table 2 General and systolic left ventricular haemodynamic parameters at age 37 weeks LEAN OBESE Heart rate (Beats per minute) LVSP (mmHg) LV dP / dt max (mmHg/s) Ejection fraction (Percent) Cardiac output (Al/min/g) Ees (mmHg/Al) PRSW (mmHg) 294 T 11 232 T 14* 111 T 6 103 T 8 6037 T 485 5123 T 454 54 T 3 51 T 5 116.0 T 19.0 100.3 T 14.6 0.73 T 0.17 0.69 T 0.18 84.7 T 10.0 83.2 T 17.7 N = 8 – 10. Data are mean T SEM. *p < 0.05 vs. LEAN. Ees, end systolic elastance; PRSW, slope of the (linear) preload recruitable stroke work relationship. S. Schäfer et al. / The European Journal of Heart Failure 8 (2006) 2 – 6 contrast, among the indices of diastolic function, those reflecting LV relaxation (i.e., dP / dt min and s) were significantly impaired in OBESE compared to LEAN. Interestingly, indices of LV compliance (LVEDP, LVEDV, and EDPVR) were not significantly different between the two groups. 4. Discussion The present study demonstrates a predominantly diastolic LV dysfunction in rats with type 2 diabetes mellitus. More specifically, we have shown that myocardial relaxation is prolonged when LV contractility and compliance are not (yet) significantly impaired in diabetic rats at age 37 weeks. The functional impairment is related to the myocardial accumulation of CML, a prototypical advanced glycation end product (AGE). Taken together, these data support the hypothesis that AGEs can impair myocardial function and potentially contribute to heart failure in type 2 diabetes even in the absence of myocardial ischemia. Based on early observations of structural alterations in postmortem diabetic hearts, a number of clinical and experimental studies have aimed to characterize the function of the diabetic heart. Systolic or diastolic dysfunction, or both, has been described inconsistently in patients with type 1 and type 2 diabetes mellitus, using non-invasive — mostly echocardiographic — methods [10,11], for review see Ref. [12]. Likewise, echocardiographic studies in experimental type 2 diabetes have revealed discrepant results. Earlier reports describing reduced myocardial systolic function in Zucker diabetic fatty [13] and Goto-Kakizaki rats [14] could not be reproduced by another group [15]. In addition, Ren et al. reported decreased contractility and relaxation properties in cardiomyocytes isolated from obese but non-diabetic Zucker rats [16]. The present study is the first to use pressure – volume data in an effort to measure load independent indices of LV systolic and diastolic function. Using this method, we were able to identify that prolongation of myocardial relaxation (as distinct from decreased myocardial compliance) seems to be the predominant feature of diabetic cardiomyopathy when systolic function is preserved. Few randomized clinical trials have addressed the effect of pharmacological treatments in diastolic heart failure, but interventions leading to bradycardia and angiotensin receptor blockade seem to be effective. Smaller studies indicate that glycemic control can also improve LV diastolic dysfunction in type 2 diabetes, but these findings have not always been reproducible (for review see Ref. [12]). The specific alterations in myocardial metabolism known to occur in diabetes may offer additional therapeutic targets for diabetic cardiomyopathy beyond normalizing blood glucose levels. Data from diabetic patients have demonstrated an accumulation of AGEs in different tissues, including the myocardium [17]. Moreover, serum AGE levels have been linked to LV diastolic dysfunction in type 1 diabetic patients 5 [6]. Together with the present study in type 2 diabetes, these data provide a strong rationale for a pathogenetic role of AGEs in diabetic cardiomyopathy. Of note, LV relaxation was linked to myocardial, but not serum, CML levels in the present study. Serum AGE levels are strongly dependent on liver and kidney function, indicating a major role of the two organs in metabolism and/or excretion of AGEs [18,19]. Also, a diet rich in AGEs can exacerbate diabetic and nondiabetic nephropathy [20,21]. Although obese rats develop massive proteinuria, creatinine clearance is not reduced until a very advanced age is reached [22,23]. Further studies are needed to determine the influence of renal or hepatic excretion on AGE levels and its consequences on the myocardium. Different mechanisms may be responsible for the detrimental effect of accumulating AGEs on myocardial structure and function. Firstly, modification of proteins promoting myocardial contraction or relaxation may occur, leading to impaired systolic or diastolic function and to structural alterations, depending on the proteins involved [24]. Secondly, AGEs may be able to promote transdifferentiation of epithelial cells to myofibroblasts via their specific receptors (e.g., RAGE) [25]. Finally, activation of RAGE promotes inflammation and oxidative stress, which can decrease the bioavailability of nitric oxide. Among many other effects, nitric oxide has been shown to improve myocardial relaxation [26]. Thus, activation of RAGE can have a direct functional impact on myocardial relaxation. It is interesting to note that in the diabetic myocardium both accumulated AGEs and their receptors seem to be predominantly localized in the coronary vasculature rather than in the cardiomyocytes [17,27]. Thus, apart from the left ventricular functional effects analysed in the present study, the AGE – RAGE interaction may at least in part be accountable for the accelerated rate of coronary artery disease in diabetic patients [28]. Interestingly, the novel AGE crosslink breaker ALT-711 has improved many morphological features of cardiomyopathy in rats and dogs with hypo-insulinaemic diabetes [29,30], further strengthening the concept of AGE-induced myocardial dysfunction as an underlying cause of diabetic cardiomyopathy. In summary, using load independent indices of LV function, we have shown that functional impairment of the type 2 diabetic myocardium is characterized by a predominant prolongation of relaxation. The correlation between myocardial AGE content and LV relaxation supports a specific pathogenetic role of AGEs in diabetic cardiomyopathy. Acknowledgements The authors wish to thank Gerald Fischer for excellent technical support. The present study is part of the ‘‘Cardiovascular and Renal Endpoints in Diabetes (CARED)’’ preclinical study program. 6 S. Schäfer et al. / The European Journal of Heart Failure 8 (2006) 2 – 6 References [1] Bertoni AG, Tsai A, Kasper EK, Brancati FL. Diabetes and idiopathic cardiomyopathy: a nationwide case-control study. Diabetes Care 2003;26:2791 – 5. [2] Hayat SA, Patel B, Khattar RS, Malik RA. Diabetic cardiomyopathy: mechanisms, diagnosis and treatment. Clin Sci (Lond) 2004;107:539 – 57. [3] Ahmed N. Advanced glycation endproducts — role in pathology of diabetic complications. Diabetes Res Clin Pract 2005;67:3 – 21. [4] Kilhovd BK, Berg TJ, Birkeland KI, Thorsby P, Hanssen KF. Serum levels of advanced glycation end products are increased in patients with type 2 diabetes and coronary heart disease. Diabetes Care 1999;22:1543 – 8. [5] Schleicher ED, Wagner E, Nerlich AG. Increased accumulation of the glycoxidation product N(epsilon)-(carboxymethyl)lysine in human tissues in diabetes and aging. J Clin Invest 1997;99:457 – 68. [6] Berg TJ, Snorgaard O, Faber J, Torjesen PA, Hildebrandt P, Mehlsen J, et al. Serum levels of advanced glycation end products are associated with left ventricular diastolic function in patients with type 1 diabetes. Diabetes Care 1999;22:1186 – 90. [7] Norton GR, Candy G, Woodiwiss AJ. Aminoguanidine prevents the decreased myocardial compliance produced by streptozotocin-induced diabetes mellitus in rats. Circulation 1996;93:1905 – 12. [8] Weisfeldt ML, Frederiksen JW, Yin FC, Weiss JL. Evidence of incomplete left ventricular relaxation in the dog: prediction from the time constant for isovolumic pressure fall. J Clin Invest 1978;62: 1296 – 302. [9] Boehm BO, Schilling S, Rosinger S, Lang GE, Lang GK, KientschEngel R, et al. Elevated serum levels of N(epsilon)-carboxymethyllysine, an advanced glycation end product, are associated with proliferative diabetic retinopathy and macular oedema. Diabetologia 2004;47:1376 – 9. [10] Zabalgoitia M, Ismaeil MF, Anderson L, Maklady FA. Prevalence of diastolic dysfunction in normotensive, asymptomatic patients with well-controlled type 2 diabetes mellitus. Am J Cardiol 2001;87: 320 – 3. [11] Poirier P, Bogaty P, Garneau C, Marois L, Dumesnil JG. Diastolic dysfunction in normotensive men with well-controlled type 2 diabetes: importance of maneuvers in echocardiographic screening for preclinical diabetic cardiomyopathy. Diabetes Care 2001;24:5 – 10. [12] Cosson S, Kevorkian JP. Left ventricular diastolic dysfunction: an early sign of diabetic cardiomyopathy. Diabetes Metab 2003;29: 455 – 66. [13] Zhou YT, Grayburn P, Karim A, Shimabukuro M, Higa M, Baetens D, et al. Lipotoxic heart disease in obese rats: implications for human obesity. Proc Natl Acad Sci U S A 2000;97:1784 – 9. [14] Iltis I, Kober F, Desrois M, Dalmasso C, Lan C, Portha B, et al. Defective myocardial blood flow and altered function of the left ventricle in type 2 diabetic rats: a noninvasive in vivo study using perfusion and cine magnetic resonance imaging. Invest Radiol 2005;40:19 – 26. [15] Fredersdorf S, Thumann C, Ulucan C, Griese DP, Luchner A, Riegger GA, et al. Myocardial hypertrophy and enhanced left ventricular contractility in Zucker diabetic fatty rats. Cardiovasc Pathol 2004;13: 11 – 9. [16] Ren J, Sowers JR, Walsh MF, Brown RA. Reduced contractile response to insulin and IGF-I in ventricular myocytes from genetically obese Zucker rats. Am J Physiol Heart Circ Physiol 2000;279: H1708 – 14. [17] Schalkwijk CG, Baidoshvili A, Stehouwer CD, van Hinsbergh VW, Niessen HW. Increased accumulation of the glycoxidation product N epsilon-(carboxymethyl)lysine in hearts of diabetic patients: generation and characterisation of a monoclonal anti-CML antibody. Biochim Biophys Acta 2004;1636:82 – 9. [18] Sebekova K, Kupcova V, Schinzel R, Heidland A. Markedly elevated levels of plasma advanced glycation end products in patients with liver cirrhosis — amelioration by liver transplantation. J Hepatol 2002;36: 66 – 71. [19] Sebekova K, Blazicek P, Syrova D, Krivosikova Z, Spustova V, Heidland A, et al. Circulating advanced glycation end product levels in rats rapidly increase with acute renal failure. Kidney Int, Suppl 2001;78:S58 – 62. [20] Sebekova K, Faist V, Hofmann T, Schinzel R, Heidland A. Effects of a diet rich in advanced glycation end products in the rat remnant kidney model. Am J Kidney Dis 2003;41:S48 – 51. [21] Zheng F, He C, Cai W, Hattori M, Steffes M, Vlassara H. Prevention of diabetic nephropathy in mice by a diet low in glycoxidation products. Diabetes Metab Res Rev 2002;18:224 – 37. [22] Schäfer S, Linz W, Bube A, Gerl M, Huber J, Kürzel GU, et al. Vasopeptidase inhibition prevents nephropathy in Zucker diabetic fatty rats. Cardiovasc Res 2003;60:447 – 54. [23] Erdely A, Freshour G, Maddox DA, Olson JL, Samsell L, Baylis C. Renal disease in rats with type 2 diabetes is associated with decreased renal nitric oxide production. Diabetologia 2004;47:1672 – 6. [24] Cooper ME. Importance of advanced glycation end products in diabetes-associated cardiovascular and renal disease. Am J Hypertens 2004;17:31S – 8S. [25] Oldfield MD, Bach LA, Forbes JM, Nikolic-Paterson D, McRobert A, Thallas V, et al. Advanced glycation end products cause epithelialmyofibroblast transdifferentiation via the receptor for advanced glycation end products (RAGE). J Clin Invest 2001;108:1853 – 63. [26] Paulus WJ, Vantrimpont PJ, Shah AM. Acute effects of nitric oxide on left ventricular relaxation and diastolic distensibility in humans. Assessment by bicoronary sodium nitroprusside infusion. Circulation 1994;89:2070 – 8. [27] Sun M, Yokoyama M, Ishiwata T, Asano G. Deposition of advanced glycation end products (AGE) and expression of the receptor for AGE in cardiovascular tissue of the diabetic rat. Int J Exp Pathol 1998;79:207 – 22. [28] Naka Y, Bucciarelli LG, Wendt T, Lee LK, Rong LL, Ramasamy R, et al. RAGE axis: animal models and novel insights into the vascular complications of diabetes. Arterioscler Thromb Vasc Biol 2004;24: 1342 – 9. [29] Candido R, Forbes JM, Thomas MC, Thallas V, Dean RG, Burns WC, et al. A breaker of advanced glycation end products attenuates diabetes-induced myocardial structural changes. Circ Res 2003;92: 785 – 92. [30] Liu J, Masurekar MR, Vatner DE, Jyothirmayi GN, Regan TJ, Vatner SF, et al. Glycation end-product cross-link breaker reduces collagen and improves cardiac function in aging diabetic heart. Am J Physiol Heart Circ Physiol 2003;285:H2587 – 91.