Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Aortic stenosis wikipedia , lookup
Cardiac surgery wikipedia , lookup
Jatene procedure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
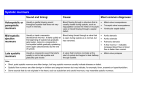
Do You Hear What I Hear Here? A Primary Care Approach to Murmurs, and Heart Sounds and Clicks, Oh My. Benjamin Hoffman MD, FAAP Assistant Professor of Pediatrics University of New Mexico OBJECTIVES Objectives • By the end of this talk, you should be able to: • Describe When and Where Blood Flows in the Heart • Discuss Basics of Cardiac Auscultation • Discuss Different Types of Murmurs – Pathologic – Innocent • Make Appropriate Referrals What is a Murmur • The Sound of Turbulent Flow – Whitewater! • Estimated 75-100% of children throughout their lifetime • Show Me the Blood Flow! Cardiac Cycle: End Systole Semi-lunar valves Closed Vent. Pressure= Great Artery Pressure No Blood Flow Cardiac Cycle:Early Diastole Vent. Relaxation= Isovolumetric Relaxation Closure of Semilunar Valves= S2 Atrial Filling (Silent) P2 A2 Cardiac Cycle: Diastole Increased Atrial Pressure Decreased Vent. Pressure Pa>Pv: AV Valves Open, Rapid Passive Filling (80%) Cardiac Cycle: Atrial Systole Atrial Systole 20% of Atrial Ejection Cardiac Cycle:Systole Ventricular Systole Rapid Increase Pv Pv>Pa: AV Valve Closure S1 THIS IS THE KEY ISOVOLUMETRIC Contraction Period After S1 NO BLOOD FLOW Cardiac Cycle: Systole Pv increases, SL valves open Ejection The Challenge • To Distinguish the Good, the Bad and the Ugly – What do we need to know? – When do we Refer? Characterizing Murmurs • Where – Is it loudest, Does it Radiate • When – Systolic, Diastolic • How – Pitch, Quality, Shape Levine Classification Levine Classification Where Do You Listen? Heart Sounds • S1: – Occurs at the onset of systole • Associated with A/V valve closure • Intensity of directly related to peak rate of rise of LV pressure Ode to a Second Heart Sound • S2: – The ability to hear this is crucial – Associated with closure of semilunar valves – Normally split with respiration, A2-P2 P2 A2 Splitting of S2 Expiration Inspiration Ode to a Second Heart Sound • Fixed: ASD • Loud: Increased Pulmonary Pressures • Single: – Truncus Arteriosis, – Transposition (Pulm. Valve Posterior) Miscellaneous Sounds •S3: low frequency sound at end of rapid filling •Ejection clicks: –sudden limitation to filling –bileaflet semilunar valve –normal or abnormal depending on context –dilated Ao or PA •S4: atrial kick into a noncompliant ventricle (abnormal) –Mid-systolic click –MVP •Opening Snap –MS Auscultation Helpers • Inspiration – Increased venous return to RV> increased right heart murmur • Expiration – Increased pulmonary blood flow and return to LV-> increased left heart murmur • Clicks are best appreciated sitting Auscultation Helpers • Evaluation in different positions – Supine: End-diast. volume is increased-> increased stroke-volume • Any outflow murmur that is dependent the amount of flow will be louder supine – EXCEPTION: Hypertrophic cardiomyopathy » When sitting, intracardiac volume is decreased-> increased outflow obstruction -> increased murmur. Auscultation Helpers • Valsalva: – Increased intrathoracic pressure->decreased venous return-> decreased end-diastolic volume. • Hypertrophic cardiomyopathy murmur increased • Mitral regurg. is increased, click of mitral valve prolapse is increased. – Release of Valsalva • increased blood flow to right heart-> accentuation of right-sided murmurs. • On 2nd or 3rd beat, increased blood flow to left heart, accentuating murmurs there. Murmurs Only 2 Types Systolic Innocent Diastolic Pathologic Diastolic Murmurs LATE Early Diastolic Late Diastolic Semi-Lunar Valves Regurg A-V Valves Stenosis EARLY P2 A2 Diastolic Murmurs • Low Pressure, Low Flow • Hard to Hear!!! • REFER!!!! Systolic Murmurs Only 2 Types Systolic Innocent Pathologic Systolic Ejection Ejection S1 Coincident (Holosystolic) Innocent Pathologic Systolic Murmurs: Pathologic • S1 Coincident • Regurgitation at AV valves • Occurs with, or Obscures S1 • REFER!!!!!!!! S1 Ejection Murmurs • Remember Isovolumetric Contraction – S1, then a break before opening of SL valves. • Occurs Mid-Late Systole – Can Clearly Differentiate S1 – Crescendo, Decrescendo S1 S1 Systolic Murmurs: Pathologic • Ejection • Occurs at the Outflow Tract – Subvalvular • IHSS/HOCM – Valvular • AS, PS – Opening Snap – Supravalvular • Coarctation – Pulses, 4 Ext BP HCM: A Special Case • Unregulated Proliferation of Septal Wall Muscle • Mobile Obstruction • Systolic Ejection Murmur Loudest When End-Diastolic Volume Smallest What about VSD’s, Einstein? • Most Common Congenital Lesion – 25% CHD – 90-95% Resolve by 1st Birthday • Remember: V=IR – I=V/R • Smaller= Louder, and Later • S1 Coincident, or Ejection S1 S1 And ASD’s?? • “Fixed Split” S2 – Increased End Diastolic Volume Right Ventricle • Pulmonic Flow Murmur – Low Pitched, Rumble-y • Rabbit Ears on EKG – RBBB A2 Systolic Murmurs: Innocent • Mumurs Not Associated with Anatomic or Physiologic Abnormalities • 50-100% of Children • Early Systolic Ejection, Short Duration, Grade I-III, DO Not Radiate Still’s Murmur • Age over 2 years • Gr. I-III, Short, MidSystolic • Apex, LLSB • Why? – Narrower than Ventricle – More Acute Angle – “Bottleneck around a Corner!” Still’s Murmur • Quality: – Musical, Harmonic, Vibratory – Low Frequency • Bell>Diaphragm – Loudest Supine – Fluid Flowing over a String? Pulmonic Flow Murmur • Any Age Group • Gr. I-III, Blowing, Mid-Systolic • Diaphragm>Bell • LUSB • May Radiate to Back • Loudest Supine Peripheral Pulmonic Stenosis • Newborns (2-6 Months) – Especially Premies • Gr. I-II, “breathy”, high pitched • As Loud, or Louder, in Axillae • Small Caliber, Acute Branching of Branch PA’s Other Innocent Murmurs • Venous Hum – Present Only Sitting – Disappears Supine – Clavicle/Neck • Carotid Bruit • Mammary Souffle Questions? So, What DO We Do? • Listen Carefully • Use Ancillary Tests to Help – EKG, CXR, Oximetry, 4 Ext. BP’s • Refer: – – – – – All Grade IV-VI All Diastolic All S1 Coincident Systolic Cyanosis, Decreased Pulses or LE BP’s Poor Feeding, Sweating, Poor Weight Gain Murmurs and Appy’s??? • No Shame in Referring an Innocent Murmur!!! • Phone/Fax your Friendly Cardiologist