Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Middle East respiratory syndrome wikipedia , lookup
Ebola virus disease wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Marburg virus disease wikipedia , lookup
Oesophagostomum wikipedia , lookup
History of biological warfare wikipedia , lookup
Cross-species transmission wikipedia , lookup
Leptospirosis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
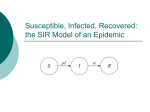
Why Canadian fur trappers should stay in bed when they have the flu: modeling the geographic spread of infectious diseases Lisa Sattenspiel Department of Anthropology University of Missouri-Columbia Major approaches to modeling the transmission of infectious diseases • Deterministic compartmental models (systems of differential equations) • Statistical approaches (e.g., regression analysis, time series analysis, generalized linear models, spatial statistics) • Stochastic compartmental models (e.g. chain binomial model) • Individual-based mathematical models • Computer-based models – Microsimulations – Agent-based models General structure of a deterministic epidemic model with three linked communities + a disease process Susceptible Infectious infection Recovered recovery a mobility process Community 1 Community 2 The chance of infection is a function of both contact (a social process) and transmission (a biological process) Community 3 , the rate of leaving a community , the distribution of destinations , the rate of return Community composition as a result of the mobility process AA B B C A B A C mobility process B BCC A A A B B B C C C C B C C A A C C Transmission of infection occurs only between an infectious person and a susceptible person who happen to be in the same region at time t. The risk of infection is a function not only of the personal characteristics of the susceptible and infectious individuals, but also of the place where they come into contact with one another. dSii ik Sik i Sii i iji dt k dSik dt Sik I jk N k* j ik I ik i I ii i iji dI ik dt dRii dt dRik dt N i* j i ik Sii ik Sik k ijk dt dI ii Sii I ji k Sii I ji j i ik I ii ik I ik k ijk j ik Rik i Rii I ii k i ik Rii ik Rik I ik N i* I ii Sik I jk N k* I ik The Keewatin District The environment at and near Norway House Mortality before, during, and after the flu epidemic Anglican burials at Norway House, 1909 to 1929 50 burials 40 30 20 10 0 1909 1914 1919 year 1924 1929 Mortality among communities within Manitoba 300 Deaths per 1000 250 200 150 100 50 0 Norway House Fisher River Berens River Fort Alexander Oxford House God's Lake Distribution of deaths by family Norway House 1919 237 families 180 Observed Expected number of families 160 140 120 significantly fewer observed 100 80 60 40 20 0 0 1 2 3+ number of deaths G-value = 17.33, p < 0.05, df = 2 Families with three to five deaths Norway House 1919 6 number of individuals 5 4 Alive 1918 Dead 1919 3 2 1 0 Salmon Robin Robin Marten family Moose Fisher Muskrat Initial questions a) b) How do changes in the rates and patterns of mobility affect epidemic spread? How do changes in rates of contact within communities affect epidemic spread? Changes in rates and patterns of mobility do not significantly affect the size of epidemic peaks although they do affect the timing of epidemic spread 180 160 140 NH—w ° cases 120 NH—s° 100 OH—w ° 80 OH—s° GL—w ° 60 GL—s° 40 20 0 0 50 100 150 day 200 250 300 Changing social organization by varying the contact rate within communities DOES lead to significant changes in the size and timing of epidemic peaks 200 NH, both equal and unequal contact 180 Number of cases 160 140 120 100 OH, equal contact 80 GL, equal contact 60 40 OH, unequal contact 20 GL, unequal contact 0 0 50 100 150 Day 200 250 300 Some of the questions addressed in the project 1) 2) 3) 4) 5) How do changes in frequency and direction of travel among socially linked communities influence patterns of disease spread within and among those communities? How do differences in rates of contact and other aspects of social structure within communities affect epidemic transmission within and among communities? What is the effect of different types of settlement structures and economic relationships among communities on patterns of epidemic spread? What was the impact of quarantine policies on the spread of the flu through the study communities? Do we see the same kinds of results with other diseases and in other locations and time periods? BUT the real study populations are so small that the deterministic models presented so far are not really the best ones to use. Solution: Develop an individual-based epidemic model that can deal with the variability of individual behaviors and the stochasticity that results when populations are small Seasonal differences in social organization in the northern fur trade • • • • • • • Social group size and composition Dispersal on the land Resource availability Modes of travel Travel routes Numbers traveling Time to complete a journey Stage 1 Develop a single-post agentbased model that captures significant aspects of the community structure at the main post, Norway House 150 NH—w° 100 OH—w° NH—s° OH—s° 50 GL—w° GL—s° 0 0 100 200 300 day Comparison of a Summer & Winter Epidemic at Infectious Periods of 5 & 7 600 Summer Epidemics: short duration, high peak, peak quickly 500 Number of People Infected cases Changes in rates and patterns of mobility do not significantly affect the size of epidemic peaks 400 300 Winter Epidemics: long duration, low peak, peak slowly 200 100 0 0 20 40 60 80 100 120 140 Infectious Period (Days) Winter - 5 Winter - 7 Summer - 5 Summer - 7 160 180 200 Stage 2 Extend the Stage 1 model to three posts so that results can be compared directly to those from the deterministic model An Epidemic at all Three Communities 450 NH Infected 400 Number 350 300 OH Infected 250 GL Infected NH Dead 200 150 OH Dead 100 GL Dead 50 0 0 20 40 60 80 100 Day 120 140 160 180 200 NHOHGL Model NHODE Model Predicted Number Infected at NH 717 190 Predicted Number Infected at OH 7 7 Predicted Number Infected at GL 0 7 Predicted Extent of Epidemic Spread Rarely reaches OH, never reaches GL Epidemic routinely reaches both OH and GL Shape of the Epidemic Curve an initial case building up to a rather short and defined epidemic peak. an initial case building up to a rather short and defined epidemic peak. Timing of the epidemic peaks First at NH First at NH Predicted Impact of Seasonality Summer epidemic has earlier and more severe peak Summer epidemic has earlier and more severe peak Result of the Introduction of the flu at OH or GL instead of NH Epidemic fails to spread; nearly all epidemic totals are impacted Epidemic spreads more readily; timing of the epidemic is affected but not the severity Parameters that influence the timing of the epidemic mobility, travel patterns, contact rates, and population parameters Mobility, travel patterns, and contact rates Parameters that Influence the spread of the epidemic mobility, travel patterns, contact rates, and population parameters Mobility and travel patterns Parameters that Influence Epidemic severity mobility, travel patterns, contact rates, and population parameters Contact rates Major potential contributions of mathematical models to human disease research • Focus research efforts on factors most likely to have a significant impact on patterns of epidemic spread. – Simulation results illuminated relative roles of population mobility and social contact within communities on infectious disease spread and shifted focus to factors influencing social contact. • Identify critical areas with insufficient data. – Results stimulated new archival searches to find data on settlement structure and seasonal activities. • Help to understand conditions under which infectious diseases emerge and spread across a landscape. – Simulations showed, for example, that patterns of mobility influence the timing of epidemic peaks and the patterns of an epidemic’s spread across space. Major potential contributions of mathematical models to human disease research (cont.) • • • May help to identify potential hot spots for the evolution of new diseases. – Simulations indicated the importance of communities taking a central role in a region, suggesting that these communities are potential hot spots in their regions. Allow for “experimentation” on human populations that would be impossible or unethical in the real world. – Infectious disease simulations follow the progress of potential epidemics within communities. Well-structured models that are grounded in high quality data provide valuable inferences with which to predict the impact of future epidemics within communities. Can be used to evaluate the efficacy of potential control strategies before attempting costly and/or risky field trials. – Simulations pointed out the difficulty of achieving success with quarantine measures alone. Acknowledgements Collaborators and colleagues: McMaster University — Ann Herring, Dick Preston University of Manitoba — Rob Hoppa University of Missouri — Carrie Ahillen, Connie Carpenter, Nate Green, Suman Kanuganti, Melissa Stoops, Emily Williams Funding: The National Science Foundation The Canadian Social Sciences and Humanities Research Council Special thanks to the Norway House First Cree Nation who generously gave permission to work with their historical documents. Leonard McKay, in particular, was a constant source of encouragement and assistance.