Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Baker Heart and Diabetes Institute wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
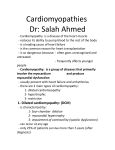
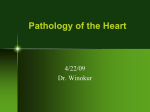
PHYSIOLOGY IN MEDICINE: A SERIES OF ARTICLES LINKING MEDICINE WITH SCIENCE Physiology in Medicine: Dennis A. Ausiello, MD, Editor; Dale J. Benos, PhD, Deputy Editor; Francois Abboud, MD, Associate Editor; William J. Koopman, MD, Associate Editor Review Annals of Internal Medicine: Paul Epstein, MD, Series Editor Adiposity of the Heart*, Revisited Jonathan M. McGavock, PhD; Ronald G. Victor, MD; Roger H. Unger, MD; and Lidia S. Szczepaniak, PhD Obesity is a major risk factor for heart disease. In the face of obesity’s growing prevalence, it is important for physicians to be aware of emerging research of novel mechanisms through which adiposity adversely affects the heart. Conventional wisdom suggests that either hemodynamic (that is, increased cardiac output and hypertension) or metabolic (that is, dyslipidemic) derangements associated with obesity may predispose individuals to coronary artery disease and heart failure. The purpose of this review is to highlight a novel mechanism for heart disease in obesity whereby excessive lipid accumulation within the myocardium is directly cardiotoxic and causes left ventricular remodeling and dilated cardiomyopathy. Studies in animal models of obesity reveal that intracellular accumulation of triglyceride renders organs dysfunctional, which leads to several well-recognized clinical syndromes related to obesity (including type 2 diabetes). In these rodent models, excessive lipid accumulation in the myocardium causes left ventricular hypertrophy and nonischemic, dilated cardiomyopathy. Novel magnetic reso- nance spectroscopy techniques are now available to quantify intracellular lipid content in the myocardium and various other human tissues, which has made it possible to translate these studies into a clinical setting. By using this technology, we have recently begun to study the role of myocardial steatosis in the development of obesity-specific cardiomyopathy in humans. Recent studies in healthy individuals and patients with heart failure reveal that myocardial lipid content increases with the degree of adiposity and may contribute to the adverse structural and functional cardiac adaptations seen in obese persons. These studies parallel the observations in obese animals and provide evidence that myocardial lipid content may be a biomarker and putative therapeutic target for cardiac disease in obese patients. T ing. In extreme obesity, this condition can progress to nonischemic dilated cardiomyopathy (2, 6). In contrast to these 2 rather traditional concepts, an emerging body of basic research is revisiting a previous hypothesis (7, 8): that fat is a direct cardiotoxin (9, 10). In 1933, the original autopsy studies of Smith and Willius (8) suggested that fatty degeneration of the heart is a common consequence of obesity and a possible cause of dilated cardiomyopathy in humans. After Alexander and colleagues (11) called this theory into question in the 1960s, the issue lay dormant for the next several decades (9). Now a growing body of evidence is revisiting the hypothesis that excessive deposits of lipids within myocardial tissue (that is, cardiac lipotoxicity) is an important but forgotten cause of nonischemic dilated cardiomyopathy in humans (12, 13). Under healthy conditions, most triglyceride is stored he unrelenting obesity epidemic is one likely explanation for the recent adverse secular trends in cardiovascular morbidity and mortality rates in the United States (1, 2). Hospitalizations for congestive heart failure have increased, and the steady decline in coronary heart disease– related deaths since the 1950s has leveled off (3). The recent obesity epidemic poses a major threat to human health in the United States because these persons will be predisposed to a burden of major chronic disease (1, 2). Obesity has both metabolic and cardiovascular health consequences; in particular, obese individuals are at much greater risk for type 2 diabetes and cardiovascular disease (3, 4). Obesity is traditionally considered to be an indirect cause of heart disease. Obese persons typically present with several Framingham risk factors, including hypertension, dyslipidemia, and diabetes mellitus. These risk factors predispose the patient to myocardial infarction that, in severe cases, results in ischemic cardiomyopathy (4). In addition to an elevated Framingham risk score, the hemodynamic hallmarks of obesity are increased heart rate and stroke volume (5). This hyperdynamic circulation is thought to be a compensatory adaptation to increased adipose tissue mass at the expense of eccentric left ventricular remodel- Ann Intern Med. 2006;144:517-524 www.annals.org For author affiliations, see end of text. *The title Adiposity of the Heart, Revisited was borrowed from an article by Smith and Willius that appeared in Archives of Internal Medicine in 1933. See also: Web-Only Conversion of figures into slides © 2006 American College of Physicians 517 Review Adiposity of the Heart, Revisited Figure 1. Concept of lipotoxicity. Lipotoxicity in humans originates from excessive release of free fatty acids from hypertrophied adipocytes in obese persons. Organ exposure to high levels of free fatty acids causes lipid droplets to accumulate within the cytosol of nonadipose tissues in proximity to mitochondria (white arrows, bottom). By-products of cytosolic triglyceride accumulation and of lipid metabolism may lead to organ dysfunction and failure. in adipocytes; the amount of triglyceride stored in nonadipocyte tissues (such as the pancreas, liver, and myocardium) is minimal and very tightly regulated. Various genetic rodent models of obesity have shown that cytosolic triglyceride accumulates excessively in these organs (termed steatosis) when this regulation is disrupted. This accumulation has been implicated in activating adverse signaling cascades that culminate in irreversible cell death (termed lipotoxicity) and lead to several well-recognized clinical syndromes (13). These include nonalcoholic hepatic steatosis; pancreatic -cell failure in type 2 diabetes; and most recently, dilated cardiomyopathy (Figure 1). The purposes of this article are to review recent basic animal research that demonstrates direct toxic effects of lipid accumulation on the myocardium and to highlight emerging efforts to translate this work into the clinical setting by using novel cardiac magnetic resonance imaging and spectroscopy technology. The results of this research could provide insight into the pathogenesis of heart disease in obese humans and guide the development of a novel biomarker and drug target for the prevention of heart failure in these persons. 518 4 April 2006 Annals of Internal Medicine Volume 144 • Number 7 STEATOSIS IN RODENTS The seminal research that showed a role for steatosis in obesity-related organ dysfunction was performed with the Zucker diabetic fatty rat, which is a genetic model of progressive type 2 diabetes (14 –16). In this obese rodent, type 2 diabetes developed secondary to a loss-of-function mutation in tissue receptors for leptin, the adipocyte-derived hormone that regulates appetite and body weight (17). This model of genetic obesity is more extreme than the milder leptin resistance that commonly accompanies dietary obesity in humans (17). Initial studies demonstrated that pancreatic steatosis directly caused islet cell failure and the subsequent hyperglycemia that characterized this model (14 –16). Although leptin was generally thought to act centrally to regulate caloric intake and energy expenditure (17), a series of studies provided experimental evidence that leptin also acts directly on the pancreatic islet cells to stimulate fatty acid oxidation, thereby limiting cellular triglyceride accumulation (18). These findings suggested that leptin signaling is also essential in regulating peripheral lipid stores. Furthermore, the investigators described a pathway whereby failure of the leptin receptor led www.annals.org Adiposity of the Heart, Revisited www.annals.org Figure 2. Myocardial lipotoxicity in the Zucker diabetic fatty rat. Myocardial Triglyceride Content, µg/mg Protein 1000 800 600 400 200 0 Control Zucker Rats 7 weeks 14 weeks 20 weeks + thiazolidinedione Left Ventricular Fractional Shortening, % to excessive cytosolic accumulation of triglyceride and its by-product, ceramide, within islet cells. This accumulation activated the inducible form of nitric oxide synthase, which accelerated cell death (apoptosis) and failure of the -cell (14, 15). Interventions that stimulated free-fatty acid oxidation, like restoration of leptin signaling or thiazolidinedione therapy, effectively attenuated triglyceride accumulation in islet cells and prevented the onset of type 2 diabetes (19). These findings provided evidence that steatosis is an integral determinant of -cell failure in the pathogenesis of obesity-associated type 2 diabetes. In addition to pancreatic -cell failure, the Zucker diabetic fatty rat experienced age-related cardiac dysfunction that was characterized by eccentric left ventricular remodeling, increased left ventricular pressure, and decreased systolic performance (9, 20). The abnormalities in cardiac structure and function are accompanied by a 2-fold increase in myocardial triglyceride content and ceramide that is similar to the accumulation seen in islet cells. Myocardial DNA laddering, which is a marker of apoptosis, is also increased (9). Of note, early administration of thiazolidinedione therapy is effective in attenuating myocardial triglyceride accumulation and normalizing left ventricular contractile performance (9, 20), as shown in Figure 2. Because reduced myocardial lipid content and improved cardiac structure and function were observed independent of changes in body weight, they strongly suggest a role for myocardial steatosis in obesity-related cardiomyopathy. The extreme obesity in the Zucker rat model makes it difficult to determine whether the cardiac maladaptations are related to excessive myocardial lipid accumulation or to increased expression of conventional risk factors for cardiovascular disease. To address this limitation, various lean genetic mouse models of cardiac-restricted steatosis have recently been developed (10, 21–29). These animals display diffuse myocardial lipid content in the absence of obesity or any other traditional cardiovascular risk factors, thereby allowing researchers to study the acute effects of myocardial steatosis on left ventricular structure and function. Overexpression of long-chain acyl-CoA synthetase, a key enzyme involved in triglyceride synthesis, produces an example of cardiac-restricted steatosis. Increased protein expression of acyl-CoA synthetase in the myocardium disrupts the balance between lipid import and export in the myocardium (Figure 3), which results in diffuse lipid accumulation and a greater than 2-fold increase in heart mass (10). The severe myocardial steatosis that is observed in this animal is associated with substantial left ventricular hypertrophy by 4 weeks of age that coincides with left ventricular dilatation and eventually progresses to heart failure. Of importance, the changes in cardiac lipid content, structure, and function develop without any change in lipid profile or body weight of the animal. This pattern of steatosis-induced heart failure has been reproduced by targeted overexpression of genes that are involved in lipid Review 70 60 50 40 30 20 10 0 Zucker Rats Top panel. Triglyceride content in the myocardium of Zucker diabetic fatty rats and lean controls at age 7 (white bars) and 14 weeks (light gray bars). The myocardial triglyceride accumulation is effectively prevented when thiazolidinedione therapy (troglitazone) is initiated at 7 weeks of age (dark gray bars). Bottom panel. Functional changes in left ventricular fractional shortening is reduced over time as rats become fat and diabetic, but it is restored by triglyceride-lowering therapy with troglitazone. (Reproduced with permission from Proc Natl Acad Sci U S A. 2000;97: 1784-9.) delivery (24, 26) and synthesis (10, 25) and by targeted deletion of genes that are involved in lipoprotein secretion (21) from the myocardium. Taken together, these data demonstrate that cardiac-specific steatosis, independent of systemic obesity, is a direct cause of dilated cardiomyopathy. The development of cardiac-restricted transgenic murine models have also shown the therapeutic potential of several countermeasures, including adenoviral administration of leptin (Figure 3) and apolipoprotein B (26, 28), dietary replacement of long-chain triglycerides with medium-chain triglycerides (22), and blockade of production of reactive oxygen species (29). Each of these interventions has effectively ameliorated the myocardial steatosis in these 4 April 2006 Annals of Internal Medicine Volume 144 • Number 7 519 Review Adiposity of the Heart, Revisited Figure 3. Myocardial-specific lipotoxicity. of left ventricular hypertrophy and dysfunction in animal models of obesity; until recently, however, few data from human research were available to support this theory. QUANTIFICATION Top panel. Substantial cardiac hypertrophy in a murine model of myocardial specific triglyceride accumulation, developed by overexpressing a key enzyme involved in triglyceride synthesis, acetyl-CoA synthetase. Middle panel. Transgenic animals displayed substantially higher heart weight (gray bars) and heart-to-body weight ratio (white bars). Bottom panel. The hearts of the transgenic mice are characterized by elevated myocardial triglyceride content. Administration of leptin in the transgenic mice attenuates cardiac hypertrophy and normalizes myocardial triglyceride content. (Reproduced with permission from Proc Natl Acad Sci U S A. 2004;101:13624-9.) mouse models and has rescued the myocardium from progression to dilated cardiomyopathy. These data reinforce the observations in the Zucker diabetic fatty rat that lipid accumulation is toxic in the myocardium. It is important to note that current thinking suggests that the cardiomyopathy is not a direct consequence of triglyceride accumulation alone, but that cardiomyopathy develops secondary to an accumulation of by-products of lipid metabolism, such as ceramide or other fatty acid derivatives that are known to interfere with intracellular signaling pathways (9, 30). This research provides convincing evidence for an acute role of steatosis in the development 520 4 April 2006 Annals of Internal Medicine Volume 144 • Number 7 OF LIPIDS IN HUMAN TISSUES To study the role of steatosis in the clinical setting, we and others have developed a magnetic resonance imaging and spectroscopy technique that permits the precise and reproducible quantification of intracellular triglyceride in various human organs, including skeletal muscle (31–33); the liver (34, 35); and most recently, the myocardium (36, 37). This method offers a technological advantage because it can distinguish the large compartments of triglyceride in adipose tissue cells (which contain very little water) from the triglyceride droplets that are stored in the cytosol of parenchymal cells to be used as a direct source of energy. Distinguishing between these 2 compartments is central to understanding the concept of lipotoxicity, which forms the basis for the theory that excessive cytosolic lipid leads to cellular dysfunction and occasionally to organ failure (13). By using in vivo spectroscopy, we can distinguish between lipids stored in intracellular and extracellular compartments because the frequency at which triglyceride molecules resonate depends on whether their local environment is aqueous (33, 34). In human skeletal muscle, this technique enables the quantification and distinction of triglyceride that is stored in layers of adipocytes that intersect muscle fibers (that is, marbling) and intramyocellular triglyceride that is stored in each myofiber. To accomplish this task, an area of muscle that is relatively devoid of marbling is identified as a volume of interest on magnetic resonance imaging, and localized spectroscopy is used to resolve the different resonances: 1.6 ppm for adipocytederived (extramyocellular) triglyceride and 1.4 ppm from cytosol-derived (intramyocellular) triglyceride (Figure 4). This technique was validated with in vivo and ex vivo studies by comparing values that were obtained from magnetic resonance spectroscopy with values obtained from direct biochemical technique (32). We also tested the method in patients with generalized congenital lipodystrophy, a rare autosomal disorder in which the genes involved in adipogenesis are mutated (38). These patients provided a human model of skeletal muscle that was devoid of adipose cells but displayed excessive lipid accumulation within parenchymal cells. As illustrated in Figure 4, the magnetic resonance spectra obtained from these patients confirmed a single resonance at 1.4 ppm (characteristic of intramyocellular lipid content), whereas no measurable peak could be observed at 1.6 ppm (33). The noninvasive nature and relative simplicity of this technique has made it a popular procedure among researchers who are interested in studying the role of muscle and hepatic steatosis in obesityrelated insulin resistance (39). Through use of this technique, the role of steatosis in the pathogenesis of type 2 diabetes has been rapidly elucidated; however, this technolwww.annals.org Adiposity of the Heart, Revisited Review Figure 4. Magnetic resonance spectroscopy to evaluate skeletal muscle steatosis. High-resolution images (left) of the calf muscle of a healthy patient (A) and a patient with lipodystrophy (B). The image was used to select a testing volume for spectroscopy within skeletal muscle away from adipose fat (boxes). In a localized spectroscopy setup, only a signal from the selected volume is collected. Any other signal is destroyed and is not acquired. In these images, fat appears very bright, muscles are gray, and bones are black. Blood flowing into vessels is highlighted, and blood flowing out of vessels is black. The calf of a healthy control has a layer of adipose tissue and white marble fatty spots between muscle fibers. The lipodystrophic patient has no adipose fat present. The magnetic resonance spectrum (middle) from the tested volume contains a strong signal from tissue water and a very intense signal from triglyceride. Enlarged resonance (right) of triglyceride region in a healthy patient and a patient with lipodystrophy. In the healthy patient, the fat spectrum contains 2 separate resonances: 1 from adipose fat between muscle fibers and 1 from triglyceride droplets within muscle cells. In the patient with lipodystrophy, the fat spectrum resonates exclusively from intramuscular triglyceride. ogy was only recently made available to study the role of myocardial steatosis in obesity-related cardiomyopathy. MYOCARDIAL STEATOSIS IN HUMANS In the early 19th century, Laennec (7) first described the concept of fatty degeneration of the heart, a phenomenon in which lipid accumulation in the myocardium produces a toxic effect; this condition later became known as myocardial steatosis and was used to explain the greater risk for heart disease and death in obese patients. The topic was revisited in 1933 when Smith and Willius (8) reported that, on autopsy, lipids had infiltrated the myocardium to some extent in nearly 40% of obese patients. These findwww.annals.org ings were called into question in 1965 when Alexander (11) described only 1 case of myocardial fatty infiltration in 12 morbidly obese patients who died of nonischemic heart failure and had no signs of coronary artery disease on autopsy. In the 4 decades since this observation, research has generated an overwhelming amount of cross-sectional evidence describing cardiac structure and function in obese humans (40 – 42); however, it has yet to be determined whether myocardial steatosis is an underlying mechanism for obesity-related cardiomyopathy in humans. Until recently, the primary obstacle to studying myocardial steatosis in humans was related to the difficulties associated with quantifying lipid content in the human 4 April 2006 Annals of Internal Medicine Volume 144 • Number 7 521 Review Adiposity of the Heart, Revisited Figure 5. Quantification of triglyceride within the human myocardium with magnetic resonance spectroscopy. In this high-resolution, 4-chamber cardiac magnetic resonance image (left), heart muscle appears dark gray; blood in myocardial chambers and epicardial and adipose fats are lighter. The volume for testing myocardial tissue (box) was placed within an intraventricular septum and away from epicardial fat. Magnetic resonance spectrum (right) with representative myocardial triglyceride resonance at 1.4 ppm. RA ⫽ right atria; LA ⫽ left atria; RV ⫽ right ventricle; LV ⫽ left ventricle. myocardium. To quantify triglyceride content in the human myocardium, we applied the same magnetic resonance imaging and spectroscopy technique that is used to measure triglyceride accumulation in muscle and liver cells (36, 37). Unlike the liver and muscle, however, quantification of lipid in the myocardium is difficult because the heart is perpetually in motion and is surrounded by a large depot of adipocytes (epicardial fat pad) that could interfere with the measurements. To overcome these limitations, the sample volume is placed in the interventricular septum (Figure 5) because it is the portion of the myocardium most distal from the large epicardial fat pad that envelops the heart. Furthermore, samples are obtained only during end-systole (when the heart is at its thickest diameter) and end-exhalation (when heart–lung interaction is minimal). 522 4 April 2006 Annals of Internal Medicine Volume 144 • Number 7 Initial studies in lean and otherwise healthy obese humans revealed that this method offers good test–retest reliability of myocardial triglyceride content in the same individual over hours, days, and months, which suggests that it could be a useful new clinical research tool in prospective intervention trials (36, 37). Furthermore, myocardial triglyceride content appears to increase progressively with body mass index, a measure of generalized obesity (36). This relationship seems to be continuous, and there is no apparent cutoff or deflection point at which triglyceride content increases dramatically (Figure 6). Because the interindividual variability is quite high, adiposity is not the sole determinate of lipid deposition in the human myocardium. Interestingly, research seems to indicate that a single fatty “western” meal does not change intramyocardial fat www.annals.org Adiposity of the Heart, Revisited Review novel mechanism that may act independently of coronary artery disease to cause dilated cardiomyopathy. The clinical implications of this research are exciting but have yet to be determined. Figure 6. Myocardial triglyceride levels correlate positively with body mass index. From the University of Texas Southwestern Medical Center, Dallas, Texas. Fat-to-Water Ratio, % Myocardial Triglyceride Content 1.5 Grant Support: This work was funded by grants from the Donald W. 1.0 Reynolds Foundation; National Institutes of Health/National Center for Research Resources (USPHS GCRC grant M01-RR00633); National Heart, Lung, and Blood Institute (K-25 award HL-68736); American Diabetes Association (Innovative Methodologies Award #7-04-IN-21); Veterans Affairs Medical Center, Dallas, Texas; National Institute of Diabetes and Digestive and Kidney Diseases; and by a Target Obesity Postdoctoral Fellowship from the Heart and Stroke Foundation of Canada, the Canadian Institutes of Health Research, and the Canadian Diabetes Association. 0.5 20 25 30 35 40 Body Mass Index, kg/m2 In healthy persons without diabetes or hypertension, myocardial triglyceride levels are low and gradually increase as the body mass index increases. levels; however, our method is able to detect a 3-fold increase in myocardial lipid levels that occurs in patients who fast for 48 hours (38). Normally, a compensatory increase in myocardial triglyceride levels accompanies increases in body mass index; we speculate that this increase is not toxic initially but becomes detrimental after decades of sustained substrate excess. Unfortunately, only invasive techniques are available for distinguishing between long-chain triglycerides and ceramide in humans. It is unclear whether a quantitative measurement of lipid content will serve as a useful biomarker of myocardial steatosis or whether steatosis is a causal factor in obesityrelated cardiomyopathy. Recently, a study of patients with heart failure who underwent cardiac biopsies demonstrated that patients who are obese or have type 2 diabetes have intramyocardial lipid levels that are 5 to 6 times higher than those of healthy controls (43). Of importance, the researchers observed a negative association between the degree of lipid deposition and the genes that control expression of proteins involved in contractile function. A direct association between myocardial lipid content and left ventricular performance has yet to be reported, however. Furthermore, it is unclear if thiazolidinedione therapy can prevent cardiac steatosis in humans (as animal studies have shown) or whether reducing myocardial steatosis will be an effective novel approach for interrupting the early pathogenesis of obesity cardiomyopathy. THE BOTTOM LINE For the physician who regularly diagnoses and treats ischemic cardiac disease in obese individuals, we present a www.annals.org Potential Financial Conflicts of Interest: None disclosed. Requests for Single Reprints: Lidia Szczepaniak, PhD, Department of Internal Medicine, Division of Hypertension, University of Texas Southwestern Medical Center at Dallas, Dallas, TX 75390-8899; e-mail, Lidia [email protected]. Current author addresses and author contributions are available at www .annals.org. References 1. Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, et al. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA. 2003;289:76-9. [PMID: 12503980] 2. Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, Larson MG, et al. Obesity and the risk of heart failure. N Engl J Med. 2002;347:305-13. [PMID: 12151467] 3. Roger VL, Weston SA, Redfield MM, Hellermann-Homan JP, Killian J, Yawn BP, et al. Trends in heart failure incidence and survival in a communitybased population. JAMA. 2004;292:344-50. [PMID: 15265849] 4. Wilson PW, D’Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch Intern Med. 2002;162:1867-72. [PMID: 12196085] 5. Alexander JK, Dennis EW, Smith WG, Amad KH, Duncan WC, Austin RC. Blood volume, cardiac output, and distribution of systemic blood flow in extreme obesity. Cardiovasc Res Cent Bull. 1962;1:39-44. [PMID: 14011956] 6. Vasan RS, Larson MG, Benjamin EJ, Evans JC, Levy D. Left ventricular dilatation and the risk of congestive heart failure in people without myocardial infarction. N Engl J Med. 1997;336:1350-5. [PMID: 9134875] 7. Bedford E. The story of fatty heart. A disease of Victorian times. Br Heart J. 1972;34:23-8. [PMID: 4551056] 8. Smith HL, Willius FA. Adiposity of the heart. Arch Int Med. 1933;52:811931. 9. Zhou YT, Grayburn P, Karim A, Shimabukuro M, Higa M, Baetens D, et al. Lipotoxic heart disease in obese rats: implications for human obesity. Proc Natl Acad Sci U S A. 2000;97:1784-9. [PMID: 10677535] 10. Chiu HC, Kovacs A, Ford DA, Hsu FF, Garcia R, Herrero P, et al. A novel mouse model of lipotoxic cardiomyopathy. J Clin Invest. 2001;107:813-22. [PMID: 11285300] 11. Amad KH, Brennan JC, Alexander JK. The cardiac pathology of chronic exogenous obesity. Circulation. 1965;32:740-5. [PMID: 4221214] 12. Montani JP, Carroll JF, Dwyer TM, Antic V, Yang Z, Dulloo AG. Ectopic fat storage in heart, blood vessels and kidneys in the pathogenesis of cardiovascular diseases. Int J Obes Relat Metab Disord. 2004;28 Suppl 4:S58-65. [PMID: 15592488] 13. Unger RH. Minireview: weapons of lean body mass destruction: the role of ectopic lipids in the metabolic syndrome. Endocrinology. 2003;144:5159-65. 4 April 2006 Annals of Internal Medicine Volume 144 • Number 7 523 Review Adiposity of the Heart, Revisited [PMID: 12960011] 14. Lee Y, Hirose H, Ohneda M, Johnson JH, McGarry JD, Unger RH. Beta-cell lipotoxicity in the pathogenesis of non-insulin-dependent diabetes mellitus of obese rats: impairment in adipocyte-beta-cell relationships. Proc Natl Acad Sci U S A. 1994;91:10878-82. [PMID: 7971976] 15. Hirose H, Lee YH, Inman LR, Nagasawa Y, Johnson JH, Unger RH. Defective fatty acid-mediated beta-cell compensation in Zucker diabetic fatty rats. Pathogenic implications for obesity-dependent diabetes. J Biol Chem. 1996;271: 5633-7. [PMID: 8621426] 16. Milburn JL Jr, Hirose H, Lee YH, Nagasawa Y, Ogawa A, Ohneda M, et al. Pancreatic beta-cells in obesity. Evidence for induction of functional, morphologic, and metabolic abnormalities by increased long chain fatty acids. J Biol Chem. 1995;270:1295-9. [PMID: 7836394] 17. Ahima RS, Flier JS. Leptin. Annu Rev Physiol. 2000;62:413-37. [PMID: 10845097] 18. Shimabukuro M, Wang MY, Zhou YT, Newgard CB, Unger RH. Protection against lipoapoptosis of beta cells through leptin-dependent maintenance of Bcl-2 expression. Proc Natl Acad Sci U S A. 1998;95:9558-61. [PMID: 9689119] 19. Shimabukuro M, Koyama K, Lee Y, Unger RH. Leptin- or troglitazoneinduced lipopenia protects islets from interleukin 1beta cytotoxicity. J Clin Invest. 1997;100:1750-4. [PMID: 9312173] 20. Paradise NF, Pilati CF, Payne WR, Finkelstein JA. Left ventricular function of the isolated, genetically obese rat’s heart. Am J Physiol. 1985;248:H438-44. [PMID: 3985169] 21. Bjorkegren J, Veniant M, Kim SK, Withycombe SK, Wood PA, Hellerstein MK, et al. Lipoprotein secretion and triglyceride stores in the heart. J Biol Chem. 2001;276:38511-7. [PMID: 11481337] 22. Finck BN, Han X, Courtois M, Aimond F, Nerbonne JM, Kovacs A, et al. A critical role for PPARalpha-mediated lipotoxicity in the pathogenesis of diabetic cardiomyopathy: modulation by dietary fat content. Proc Natl Acad Sci U S A. 2003;100:1226-31. [PMID: 12552126] 23. Yagyu H, Chen G, Yokoyama M, Hirata K, Augustus A, Kako Y, et al. Lipoprotein lipase (LpL) on the surface of cardiomyocytes increases lipid uptake and produces a cardiomyopathy. J Clin Invest. 2003;111:419-26. [PMID: 12569168] 24. Cheng L, Ding G, Qin Q, Huang Y, Lewis W, He N, et al. Cardiomyocyterestricted peroxisome proliferator-activated receptor-delta deletion perturbs myocardial fatty acid oxidation and leads to cardiomyopathy. Nat Med. 2004;10: 1245-50. [PMID: 15475963] 25. Chiu HC, Kovacs A, Blanton RM, Han X, Courtois M, Weinheimer CJ, et al. Transgenic expression of fatty acid transport protein 1 in the heart causes lipotoxic cardiomyopathy. Circ Res. 2005;96:225-33. [PMID: 15618539] 26. Nielsen LB, Bartels ED, Bollano E. Overexpression of apolipoprotein B in the heart impedes cardiac triglyceride accumulation and development of cardiac dysfunction in diabetic mice. J Biol Chem. 2002;277:27014-20. [PMID: 12015323] 27. Yokoyama M, Yagyu H, Hu Y, Seo T, Hirata K, Homma S, et al. Apolipoprotein B production reduces lipotoxic cardiomyopathy: studies in heart-specific lipoprotein lipase transgenic mouse. J Biol Chem. 2004;279:4204-11. [PMID: 14634011] 28. Lee Y, Naseem RH, Duplomb L, Park BH, Garry DJ, Richardson JA, et al. Hyperleptinemia prevents lipotoxic cardiomyopathy in acyl CoA synthase trans- 524 4 April 2006 Annals of Internal Medicine Volume 144 • Number 7 genic mice. Proc Natl Acad Sci U S A. 2004;101:13624-9. [PMID: 15347805] 29. Dewald O, Sharma S, Adrogue J, Salazar R, Duerr GD, Crapo JD, et al. Downregulation of peroxisome proliferator-activated receptor-alpha gene expression in a mouse model of ischemic cardiomyopathy is dependent on reactive oxygen species and prevents lipotoxicity. Circulation. 2005;112:407-15. [PMID: 16009788] 30. Schaffer JE. Lipotoxicity: when tissues overeat. Curr Opin Lipidol. 2003;14: 281-7. [PMID: 12840659] 31. Schick F, Eismann B, Jung WI, Bongers H, Bunse M, Lutz O. Comparison of localized proton NMR signals of skeletal muscle and fat tissue in vivo: two lipid compartments in muscle tissue. Magn Reson Med. 1993;29:158-67. [PMID: 8429779] 32. Szczepaniak LS, Babcock EE, Schick F, Dobbins RL, Garg A, Burns DK, et al. Measurement of intracellular triglyceride stores by H spectroscopy: validation in vivo. Am J Physiol. 1999;276:E977-89. [PMID: 10329993] 33. Szczepaniak LS, Dobbins RL, Stein DT, McGarry JD. Bulk magnetic susceptibility effects on the assessment of intra- and extramyocellular lipids in vivo. Magn Reson Med. 2002;47:607-10. [PMID: 11870849] 34. Browning JD, Szczepaniak LS, Dobbins R, Nuremberg P, Horton JD, Cohen JC, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004;40:1387-95. [PMID: 15565570] 35. Szczepaniak LS, Nurenberg P, Leonard D, Browning JD, Reingold JS, Grundy S, et al. Magnetic resonance spectroscopy to measure hepatic triglyceride content: prevalence of hepatic steatosis in the general population. Am J Physiol Endocrinol Metab. 2005;288:E462-8. [PMID: 15339742] 36. Szczepaniak LS, Dobbins RL, Metzger GJ, Sartoni-D’Ambrosia G, Arbique D, Vongpatanasin W, et al. Myocardial triglycerides and systolic function in humans: in vivo evaluation by localized proton spectroscopy and cardiac imaging. Magn Reson Med. 2003;49:417-23. [PMID: 12594743] 37. Reingold JS, McGavock JM, Kaka S, Tillery T, Victor RG, Szczepaniak LS. Determination of triglyceride in the human myocardium using magnetic resonance spectroscopy: reproducibility and sensitivity of the method. Am J Physiol Endocrinol Metab. 2005;289:E935-9 [PMID: 15972271] 38. Garg A. Acquired and inherited lipodystrophies. N Engl J Med. 2004;350: 1220-34. [PMID: 15028826] 39. Shulman GI. Unraveling the cellular mechanism of insulin resistance in humans: new insights from magnetic resonance spectroscopy. Physiology (Bethesda). 2004;19:183-90. [PMID: 15304632] 40. Peterson LR, Waggoner AD, Schechtman KB, Meyer T, Gropler RJ, Barzilai B, et al. Alterations in left ventricular structure and function in young healthy obese women: assessment by echocardiography and tissue Doppler imaging. J Am Coll Cardiol. 2004;43:1399-404. [PMID: 15093874] 41. Wong CY, O’Moore-Sullivan T, Leano R, Byrne N, Beller E, Marwick TH. Alterations of left ventricular myocardial characteristics associated with obesity. Circulation. 2004;110:3081-7. [PMID: 15520317] 42. Crisostomo LL, Araujo LM, Camara E, Carvalho C, Silva FA, Vieira M, et al. Left ventricular mass and function in young obese women. Int J Obes Relat Metab Disord. 2001;25:233-8. [PMID: 11410825] 43. Sharma S, Adrogue JV, Golfman L, Uray I, Lemm J, Youker K, et al. Intramyocardial lipid accumulation in the failing human heart resembles the lipotoxic rat heart. FASEB J. 2004;18:1692-700. [PMID: 15522914] www.annals.org Annals of Internal Medicine Current Author Addresses: Drs. McGavock and Szczepaniak: Univer- sity of Texas Southwestern Medical Center at Dallas, Department of Internal Medicine, Division of Hypertension, 5161 Harry Hines Boulevard, CS8.102, Dallas, TX 75390-8899. Dr. Victor: University of Texas Southwestern Medical Center at Dallas, Department of Internal Medicine, Division of Hypertension, 5323 Harry Hines Boulevard, J4.134, Dallas, TX 75390-8586. Dr. Unger: University of Texas Southwestern Medical Center at Dallas, Department of Internal Medicine, Touchstone Center for Diabetes, 5323 Harry Hines Boulevard, Y8.128, Dallas, TX 75390-8854. www.annals.org Author Contributions: Conception and design: R.G. Victor, R.H. Unger, L.S. Szczepaniak. Analysis and interpretation of the data: J.M. McGavock, L.S. Szczepaniak. Drafting of the article: J.M. McGavock, L.S. Szczepaniak. Critical revision of the article for important intellectual content: J.M. McGavock, R.G. Victor, R.H. Unger, L.S. Szczepaniak. Final approval of the article: R.G. Victor, R.H. Unger, L.S. Szczepaniak. Statistical expertise: J.M. McGavock. Obtaining of funding: J.M. McGavock, R.G. Victor, R.H. Unger, L.S. Szczepaniak. Collection and assembly of data: L.S. Szczepaniak. 4 April 2006 Annals of Internal Medicine Volume 144 • Number 7 W-87