Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
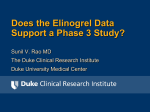
EFFECT OF PROTON PUMP INHIBITORS ON EFFICACY OF CLOPIDOGREL IN PATIENTS WITH ACUTE CORONARY SYNDROMES Introduction Clopidogrel is an antiplatelet prodrug, mainly indicated in acute coronary syndromes for prevention of further major adverse cardiac events like progression of Myocardial Infarction (MI), restenosis, stroke and death.[1, 2] GI bleeding is the major adverse effect of clopidogrel and observed more often. So, Proton Pump Inhibitors are used widely in co administration with clopidogrel.[3] Some recent studies suggest that concomitant use of PPI and Clopidogrel results in decreased efficacy of clopidogrel due to common enzyme (CYP2C19) involvement in their metabolic pathways.[4-9] Our aim was to establish the relation between efficacy of clopidogrel and concomitant PPI use. Background Metabolism of Clopidogrel: Clopidogrel is extensively metabolized by two main metabolic pathways: one mediated by esterases and leading to hydrolysis into an inactive carboxylic acid derivative (85% of circulating metabolites) and one mediated by multiple cytochrome P450 enzymes.[10] During this cytochrome P450 enzyme pathway, Clopidogrel is activated in a 2-step process mediated by oxidative biotransformation in the liver, in which CYP2C19, CYP3A, CYP2B6 and CYP1A2 have particularly important roles Cytochromes first oxidize clopidogrel to a 2-oxoclopidogrel intermediate metabolite. Subsequent metabolism of the 2-oxoclopidogrel intermediate metabolite results in formation of the active metabolite. The active thiol metabolite binds rapidly and irreversibly to platelet receptors, thus inhibiting platelet aggregation for the lifespan of the platelet.[11] Metabolism of PPI All PPIs (omeprazole, esomeprazole, pantoprazole, rabeprazole, lansoprazole, and dexlansoprazole) are metabolized by the hepatic cytochrome P-450 system, predominantly CYP2C19, and, to a lesser extent, CYP3A4. The degree to which different PPIs interact with CYP2C19 is responsible for Interaction with other agent metabolized through CYP2C19. [4] Concomitant use of clopidogrel with medications that inhibit the CYP2C19 pathway can potentially reduce its efficacy; agents with a high affinity for CYP2C19 can prevent other CYP2C19 substrates, like clopidogrel, from binding to it.[12] Genetic variants of other CYP450 enzymes may also affect the formation of clopidogrel's active metabolite. The CYP2C19*1 allele corresponds to fully functional metabolism while the CYP2C19*2, *3 and *4 alleles are nonfunctional and decrease active metabolite production compared with the most common CYP2C19 genotype. Individuals who are heterozygous for nonfunctional alleles are “intermediate metabolizers,” and those who are homozygous are “poor metabolizers”.[4] Studies have shown 51% to 55% of asians, 33% to 40% of african americans, 24% to 30% of caucasians, and 18% of mexican americans have CYP2C19*2 allele. Therefore when clopidogrel is given along with PPI there are chances for competitive drug interaction during metabolism by CYP2C19, and even more in Poor metabolizres which may result in reduced antiplatelet effect and higher rate of cardiovascular events.[13] Pharmacokinetic and pharmacodynamic studies, using platelet assays as surrogate endpoints, suggest that concomitant use of clopidogrel and a PPI reduces the antiplatelet effects of clopidogrel. The strongest evidence for an interaction is between omeprazole and clopidogrel. It is not established that changes in these surrogate endpoints translate into clinically meaningful differences.[14] Observational studies have shown inconsistent effects on Cardio vascular outcomes of concomitant use of clopidogrel and PPIs.[15] Study Methodology: A prospective as well as retrospective analysis of patients with Clinical diagnosis of ACS was carried out. Patients with Unstable Angina (UA), Non ST Elevation Myocardial Infarction (NSTEMI) or ST Elevation Myocardial Infarction (STEMI) who underwent surgical revascularization and took treatment at Life Care hospital, Ahmadabad were observed in two groups. (1) Patients receiving clopidogrel alone (n = 36) and (2) Patients receiving clopidogrel and PPI (n=39). Patients of age > 18 year with any of Index event (UA or STEMI/NSTEMI) with or without Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Grafting (CABG) after Jan 2010, managed with clopidogrel were enrolled. Patients having any history of GI bleeding, ulceration, impaired renal function or taking NSAIDs other than aspirin were excluded from study Study protocol, Case Record Form and Informed consent Form were approved by ethics committee of Life Care institute of medical sciences and research with protocol number RGR -1. Before enrolling patients, Informed consent process was carried out in presence of study investigator and signed informed consent forms were collected from the patients. Their follow up and maintenance therapy were observed for occurrence Major Adverse cardiac Events (MACE) including progression of MI, stroke, rehospitalization, revascularization or restenosis and death. Clopidogrel activity was measured in total 26 patients of which 14 patients had taken PPI (4 Patients received Omeprazole, 5 received Pantoprazole and 5 received Rabeprazole) against 12 patients had not taken any PPI during study period. Efficacy of clopidogrel was carried out by measuring maximum platelet aggregation before clopidogrel dosing (Baseline) and 2 hour after dosing Platelet aggregation was measured using VarifyNow analyzer in P2Y12 Reaction Unit (PRU) Efficacy of clopidogrel was represented as % Inhibition of Platelet aggregation (% IPA). % IPA was defined as following equation [7] (Maximum PRU at baseline− Maximum PRU at 2 Hr after dosing ) Maximum PRU at baseline X 100 Data were recorded in case record forms from Life Care Hospital, Ahmedabad and converted into Excel sheets. The data were compiled and analyzed as per ICH GCP guideline followed by Life Care Hospital. Results of % IPA were compared using one way ANOVA with 95% confidence level. Incidence of Major Adverse Cardiac Events (MACE) of both groups were compared and tested for their significances using chi square analysis using SPSS 17. Results A total of 75 patients diagnosed with ACS with or without revascularization (PCI or CABG) and had received clopidogrel were enrolled. Out of these 75 patients, 39 patients ( 74.36 % male) taking concomitant PPI had mean age of 59.95 ± 6.22 and mean BMI value of 25.84 ± 2.24 and in other group 36 patients (77.78% male) without concomitant PPI had mean age of 57.86 ± 5.39 and Mean BMI value of 26.10 ± 1.75 as shown in Table -1. Previous history and current comorbid conditions were recorded in both groups as mentioned in Table 1. Furthermore Concomitant medicines other than PPI taken by all patients during study period for management of cardiac condition were recorded as mentioned in Table 1 Inhibition of platelet aggregation was measure in total 26 out of these 75 patients. Of which 14 patients were taking concomitant PPI (4 Patients received Omeprazole, 5 received Pantoprazole and 5 received Rabeprazole) and 12 who had not taken any PPI. Inhibition of platelet aggregation was found significantly reduced in patients taking concomitant PPI administration against patients taking clopidogrel alone (Mean % IPA 16.04 ± 1.99 % Vs 23.79 ± 1.83 %, p value < 0.05) as mentioned in Table 2 & Figure 1 In addition, Inhibition of Platelet aggregation was found significantly reduced in patients taking Omeprazole (13.68 %) as compared to Pantoprazole (16.78 %) and Rabeprazole (17.18 %) as shown in Figure 2 At the end of study period, Efficacy endpoints of Major Adverse Cardiac Events (MACE) were measured and evaluated. Total incidence of rehospitalisation, reinfarction and restenosis was found greater in patients taking concomitant PPI as compared to patients not taking PPI as shown in Table 3 and Figure 3 Discussion Major finding of this study was that concomitant PPI use caused reduction in antiplatelet effect of clopidogrel. Though our finding suggested that concomitant use of PPI was associated with increased risk of major adverse cardiac events (MACE), it could not be proved statistically significant because of the limitation of smaller population size. Our results indicated that omeprazole interacted with clopidogrel resulting reduced efficacy, other PPIs also interact though to somewhat lesser extent resulting in reduced clopidogel efficacy. Effect of this reduced efficacy on rate of MACE is controversial and different studies have suggested confounding results about this scenario. Juurlink et al concluded that concomitant use of PPI with clopidogrel was associated with 40% increased risk of recurrent MI which is relevant to our study data.[16] In TIMI-TRITON 38 trial, Michelle L. O’Donoghue, found that use of PPI was not associated with increased cardio vascular events.[7] Regulatory authorities like UFFDA and EMEA also have given statements regarding PPI use. EMEA said “The product information for all clopidogrel‐containing medicines should be amended to discourage concomitant use of PPIs unless absolutely necessary."[17] And USFDA also supports this by “Healthcare providers should re‐evaluate the need for starting or continuing treatment with a PPI, including Prilosec (omeprazole) OTC, in patients taking clopidogrel."[18] Patients on dual anti-platelet therapy of aspirin clopidogrel often require gestroprotecction. The beneficial effect of PPI in preventing upper GI bleeding in patients taking antiplatelet therapy than H2 receptor antagonist has been proved.[19] Hence pantoprazole and rabeprazole should be preferred, which found inhibiting efficacy of clopidogrel in lesser amount than omeprazole as found in present study. Restriction of PPI use is very difficult because of their major part in ACS patients on clopidogrel, but separation of administration of clopidogrel and PPI including omeprazole decreases the risk of potential clinical interaction.[20] Andrzej Surdacki et al suggest that ADP induced platelet aggregation was found lower in subjects receiving clopidogrel dose after 15 hour of omeprazole administration as compared to both drug given at same time. It could be beneficial to adjust the dosing interval to administer one drug in the morning and the other one in the evening.[21] The overall risk balance between GI bleeding Vs MACE must be measured. Further studies on large population should be conducted using platelet assay as surrogate end point for entire pharmacokinetic profile or using more sophisticated analytical techniques like HPLC or LC-MS to determine effect of interaction on plasma clopidogrel level. Conclusion Our study concluded that concomitant use of PPI led to inhibition of antiplatelet effect of clopidogrel (measured by % IPA) This is expected to be due to inhibition of clopidogrel metabolism pathway by PPIs resulting in decreased prodrug formation and efficacy. Besides, the study also substantiated the reported data that omeprazole is more prone to interact with clopidogrel compared to other PPIs like pantoprazole and rabeprazole. Eventhough rate and risk of MACE was found greater in ACS patients taking concomitant PPI than patients taking clopidogrel alone, this could not be established statistically due to limited study population. Cohorts including large population are necessary to confirm the correlation between this drug interaction and to determine its fallout on frequency MACE like rehospitalization, reinfarction stroke, restenosis, revascularization and death. References: 1. Heeg B, Damen J, Van HB. Oral antiplatelet therapy in secondary prevention of cardiovascular events: an assessment from the payer's perspective. Pharmacoeconomics 2007; 25(12):1063-1082. 2. Yusuf S, Mehta SR, Zhao F, Gersh BJ, Commerford PJ, Blumenthal M, et al. Early and late effects of clopidogrel in patients with acute coronary syndromes. Circulation 2003; 107(7):966-972. 3. Manoukian SV, Feit F, Mehran R, Voeltz MD, Ebrahimi R, Hamon M et al. Impact of major bleeding on 30-day mortality and clinical outcomes in patients with acute coronary syndromes: an analysis from the ACUITY Trial. J Am Coll Cardiol 2007; 49(12):13621368. 4. Braunwald E. ACC/AHA Guideline Update for the Management of Patients with Unstable Angina and Non–ST-Segment Elevation Myocardial Infarction-2002: Summary Article: A Report of The American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients with Unstable Angina). Circulation 2002; 106:1893. 5. Zuern CS, Geisler T, Lutilsky N, Winter S, Schwab M, Gawaz M. Effect of Co medication With Proton Pump Inhibitors (PPIs) on Post-Interventional Residual Platelet Aggregation in Patients Undergoing Coronary Stenting Treated by Dual Antiplatelet Therapy. Thrombosis Research 2010; 125:E51–e54. 6. Huang CC. Risk of Adverse Outcomes in Taiwan Associated with Concomitant Use of Clopidogrel and Proton Pump Inhibitors in Patients who Received Percutaneous Coronary Intervention. Am J Cardiol 2010; 105:1705–1709. 7. O'Donoghue ML, Braunwald E, Antman EM, Murphy SA, Bates ER, Rozenman Y et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and Prasugrel with or without a proton-pump inhibitor: an analysis of two randomised trials. The Lancet 2009; 374:989-997. 8. Hulot JS, Collet JP, Silvain J, Pena A, Cayla G, Beygui F et al. Cardiovascular Risk in Clopidogrel-Treated Patients According to Cytochrome P450 2C19*2 Loss-of-Function Allele or Proton Pump Inhibitor Coadministration: A Systematic Meta-Analysis. J Am Coll Cardiol 2010; 56:134–143. 9. Ho PM, Maddox TM, Wang L, Fihn SD, Jesse RL, Peterson ED et al. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome. JAMA 2009; 301:937–944. 10. Gurbel PA, Antonino MJ, Tantry US. Recent developments in clopidogrel pharmacology and their relation to clinical outcomes. Expert Opin Drug Metab Toxicol 2009;5:989 – 1004. 11. Kazui M, Nishiya Y, Ishizuka T, Hagihara K, Farid NA, Okazaki O et al. Identification of the human cytochrome P450 enzymes involved in the two oxidative steps in the bioactivation of clopidogrel to its pharmacologically active metabolite. Drug Metab Dispos 2010; 38:92–99. 12. Price M, Schueler A. Understanding Clopidogrel’s Interaction with CYP2C19 Inhibitors. The Journal for Nurse Practitioners 2010; 6(9):715-720. 13. Mega JL, Close SL, Wiviott SD, Hockett RD, Brandt JT, Walker JR et al. Cytochrome p450 polymorphisms and response to clopidogrel. N Engl J Med 2009; 360:354–362 14. Laine L, Hennekens C. Proton pump inhibitor and clopidogrel interaction: fact or fiction? Am J Gastroenterol 2010; 105:34–41. 15. Mistry SD, Trivedi HR, Parmar DM, Dalvi PS. Imapct of proton pump inhibitors on efficacy of clopidogrel: Review of evidence. Ind J Pharmacol 2011; 43(2): 183-186 16. Juurlink DN, Gomes T, Ko DT, Szmitko PE, Austin PC, Tu JV et al. A population-based study of the drug interaction between proton pump inhibitors and clopidogrel. Canadian Medical Association Journal 2009; 180(7):713-718 17. Wathion N. Public statement on possible interaction between Clopidogrel and Proton Pump Inhibitors. May 2011 http://www.emea.europa.eu/humandocs/PDFs/EPAR/Plavix/32895609en.pdf 18. Early Communication about an Ongoing Safety Review of clopidogrel bisulfate, May 2011. http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandP roviders/DrugSafetyInformationforHeathcareProfessionals/ucm079520.htm 19. Nelson RS, Thorson AG. Risk of bleeding following hemorrhoidal banding in patients on antithrombotic therapy. Gastroenterol Clin Biol 2009; 33:463–465. 20. Cuisset T, Frere C, Quilici J, Poyet R, Gaborit B, Bali L et al. Comparison of omeprazole and pantoprazole influence on a high 150-mg clopidogrel maintenance dose: the PACA (Proton Pump Inhibitors And Clopidogrel Association) prospective randomized study. J Am Coll Cardiol 2009; 54:1149–53. 21. Chyrchel B, Surdacki A, Chyrchel M, Dudek D, Dubiel JS. Separate dosing of clopidogrel and omeprazole may improve platelet inhibition on dual antiplatelet therapy. Int J Cardiol 2011; 149(1):124-125. Tables and Figures Table 1: Demographic, history, co-morbod condition and Concomitant medication data Patients receiving clopidogrel Patients receiving clopidogrel and alone (n = 36) PPI (n=39) Male 28 (77.78%) 29 (74.36%) female 8 (22.22%) 10 (25.64%) Age 57.86 ± 5.39 59.95 ± 6.22 BMI 26.10 ± 1.75 25.84 ± 2.24 Demography History and Co-morbid condition UA 11(30.56 %) 12(30.77 %) NSTEMI 15 (41.67 %) 17 (43.59 %) STEMI 10 (27.78 %) 10 (25.64 %) Diabetes 18 (50.00 %) 19 (48.72 %) Hypertension 33 (91.68 %) 35 (89.74 %) PCI 25 (69.44 %) 24 (61.54 %) CABG 5 (13.89% ) 8 (20.51 %) Hyperlipidemia 25 (69.44 %) 26 (66.67 %) Smoking 0 5 (12.82 %) Concomitant Medication Aspirin 31 (86.11 %) 38 (97.44 %) β-blocker 30 (83.33 %) 28 (71.79 %) Ca blocker 14 (38.89 %) 16(41.03 %) ACEI/ARB 12 (33.33 %) 12 (30.77 %) Statins 25 (69.44 %) 26 (66.67 %) Table 2: Mean% inhibition of platelet aggregation Patients Mean % IPA receiving Patients receiving clopidogrel P Value clopidogrel alone (n = 12) and PPI (n=14) 23.79 ± 1.83 16.04 ± 1.99 p Value obtained by One way ANOVA <0.05 Table 3: Incidence of various MACE Patients receiving Patients receiving clopidogrel p clopidogrel alone (n = 36) and PPI (n=39) Value Hospitalizations 7 (19.44%) 10 (25.64 %) NS Reinfarction 4 (11.11 %) 7 (17.95 %) NS Restenosis 3 (8.33 %) 5 (12.82 %) NS p value obtained by chi square analysis Figure 1: Mean % Inhibition of Platelet Aggregation 25.00 Mean % IPA 20.00 15.00 10.00 5.00 0.00 Patients receiving Patients receiving clopidogrel alone (n clopidogrel and PPI = 12) (n=14) Figure 2: Mean % Inhibition of Platelet Aggregation for different PPI 20.00 18.00 Mean % IPA 16.00 14.00 12.00 10.00 8.00 6.00 4.00 2.00 0.00 Omeprazole Pantoprazole Rabeprazole Figure 3: Incidence of various MACE No of Patients 15 10 5 0 Hospitalizations Reinfarction MACE Restenosis Patients receiving clopidogrel alone (n = 36) Patients receiving clopidogrel and PPI (n=39)