Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
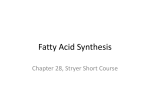
Inborn Errors of Metabolism Michael Marble, MD Associate Professor of Clinical Pediatrics Division of Clinical Genetics Department of Pediatrics, LSUHSC And Children’s Hospital A 3 day old male is brought to the emergency room with a history of lethargy progressing to unresponsiveness. You take an initial history which reveals that the baby had been feeding normally for 24 hours but thereafter became irritable and progressively less interested in feeding. On exam, you notice immediately that he is breathing fast and deep and is unresponsive. Along with other possible diagnoses, you suspect metabolic disease. (1) Which laboratory studies would you order to obtain quick evidence for or against metabolic disease? (2) You obtain a complete metabolic profile which shows a normal result. Urinalysis shows elevated specific gravity but is otherwise normal. Capillary blood gas shows respiratory alkalosis: 7.53/ pCO2 20/HCO3 nl, BE nl (3) Based on these results, what type of metabolic disease is most likely? Which test would you order next? Urea cycle disease; plasma ammonia (4) Plasma ammonia result is 1400 micromole/L (0-80). What is the most likely diagnosis? Which tests would you send to confirm a specific metabolic disorder? Plasma amino acids (5) You confirm that the patient has OTC deficiency. What is the recurrence risk in the next pregnancy? Who else in the family should be tested? X-linked inheritance therefore 50% recurrence risk if mother is a carrier. Urea Cycle Disorders DIET Protein NH4+ + Hyperammonemia without metabolic acidosis (usually have respiratory alkalosis) Ornithine •Carbamoyl phosphate synthase deficiency (AR) •Citrullinemia (AR) •Argininosuccinic acidemia (AR) •Argininemia (AR) OTC Citrulline UREA Urea cycle disorders: •Ornithine transcarbamylase deficiency (X-linked) Carbamoyl Phosphate HCO3 Arginine CYCLE urea(2N) Argininosuccinic Acid Asp (N) Headaches, recurrent vomiting, avoids meat X-linked inheritance, partially affected female A 3 day old male is brought to the emergency room with a history of lethargy progressing to unresponsiveness. You take an initial history which reveals that the baby had been feeding normally for 24 hours but thereafter became irritable and progressively less interested in feeding. On exam, you notice immediately that he is breathing fast and deep and is unresponsive. Along with other possible diagnoses, you suspect metabolic disease. (1) Which laboratory studies would you order to obtain quick evidence for or against metabolic disease? (2) You obtain a blood gas, basic metabolic profile, urinalysis and plasma ammonia which show the following: 136 101 26 96 4.8 10 0.7 UA 3+ ketones Capillary blood gas: 7.11/CO2 19, HCO3 9, BE - 11 Ammonia 646 (0-36) (3) Based on these results, what type of metabolic disease is most likely? Organic acidemias (4) How would you confirm a specific metabolic disorder in this case? Urine organic acids, plasma acylcarnitine profile Organic Acidemias Organic acids are intermediates in the catabolic pathways to break down amino acids, lipids and other compounds to acetyl CoA and succinyl CoA which are entry points into the Kreb cycle Isoleucine Valine biotin Methionine Propionyl CoA B12 Methylmalonyl CoA Succinyl CoA Cholesterol Odd chain fatty acids leucine Krebs Cycle Isovaleryl CoA 3MCC HMG CoA Acetyl CoA Lysine Tryptophan Glutaryl CoA Crotonyl CoA *Urine organic acid analysis will show elevation of organic acids proximal to the enzymatic block; the resulting pattern is interpreted by the metabolic laboratory Acetyl CoA Acylcarnitine analysis for organic acidemias: organic acidemias cause elevations of specific acylcarnitines Long chain fatty acid Fatty acid Detected by acylcarnitine profile Fatty acyl-CoA Free carnitine Fatty acyl-carnitine CPT1 Fatty acyl-carnitine Propionyl CoA propionylcarnitine Free carnitine acetyl CoA Fatty acyl-CoA Fatty acid oxidation Mitochondrion Plasma Cytoplasm ketones Krebs Selected Organic Acidemias Disease Cofactor Other features Propionic biotin Usually severe Methylmalonic B12 Some respond to B12 Isovaleric riboflavin Sweaty foot odor to urine Glutaric riboflavin Macrocephaly, dystonia, Abnormal MRI Maple syrup urine thiamine Maple syrup odor, elevated branched chain amino acids Glutaric Acidemia Type 1 Severe movement disorder Urea cycle disease versus organic acidemias UCD OA + + + ++ + +/- metabolic ketoacidosis - + primary respiratory alkalosis + - lethargy/coma vomiting hyperammonemia You are called to the newborn nursery regarding an 8 hour old female infant who is listless and not interested in feeding. On exam, the baby is severely hypotonic and lethargic but no other obvious abnormalities are noted. Accucheck shows normal glucose. Blood gas, complete metabolic profile, CBC, plasma ammonia, lactate and urinalysis all show normal results. Chest X-ray comes back normal. Along with other possibilities, you suspect a neuromuscular disorder and consult neurology. Maintenance IVFs are started. Pregnancy history is significant for decreased fetal movements. While awaiting neurology consult, the baby has apnea spells and develops myoclonic jerks. and is intubated. An EEG is performed and shows a “burst suppression” pattern. (1) What is the most likely diagnosis? Nonketotic hyperglycinemia (2) How would you confirm the diagnosis? CSF/plasma glycine ratio (3) What is the prognosis? Very poor, despite treatment Nonketotic hyperglycinemia *Defect in glycine catabolism •autosomal recessive •symptoms in first 24 hours •hypotonia/encephalopathy, seizures, burst suppression EEG •increased CSF/plasma glycine •Tx: benzoate, dextramethorphan •poor prognosis, diet ineffective *Diagnosis based on elevated CSF/Plasma glycine ratio Glycine NH3 + CO2 A 15 month old female, previously healthy, was brought to the emergency room after the mother had difficulty arousing her in the morning. Over the past 2 days, the child had had a low grade fever, cough, mild diarrhea and 3 episodes of vomiting. Due to poor appetite, the patient did not eat very much for dinner and missed her ususal bedtime snack the night before presentation. In the ER, she was noted to have a depressed mental status but was partially responsive. Initial lab testing showed the following: CBC: WBC mildly elevated CMP shows sodium 144, Cl 104, CO2 13 BUN 28 Cre 0.6, glucose 37, mild elevation of ALT and AST Urinalysis negative for reducing substances and ketones, specific gravity is elevated The ER physician starts an IV and gives a bolus of glucose to correct hypoglycemia. The physician also gives normal saline boluses for rehydration. Then IVFs with D5 ¼ normal saline is started at 1.5 maintenance fluids. Followup labs show normal serum glucose but no change in acid-base status. The patient’s mental status worsens and she becomes comatose. She is transferred to the PICU. Plasma ammonia level is found to be mildly elevated at 101 micromoles/L . Patient who presented with hypoglycemia and altered mental status Based on the above presentation and lab results, the patient most likely has a disorder within which category of inborn error of metabolism? Fatty acid oxidation defects How would you confirm a specific diagnosis? Plasma acylcarnitine profile Diagnosis of fatty acid oxidation disorders by acylcarnitine analysis Long chain fatty acid Fatty acid Detected by acylcarnitine analysis Fatty acyl-CoA Fatty acyl-carnitine Fatty acyl-carnitine Free carnitine + (C6-C12) fatty acyl CoAs (C6-C12) Fatty acyl-carnitine acetyl CoA Fatty acyl-CoA SCAD 18 16 14 12 8 6 4 MCAD Mitochondrion Plasma Cytoplasm ketones Fatty acid oxidation Brain CPT1/CPT2 Fatty acids VLCAD LCHAD MCAD fasting *key pathway for adaptation to fasting •Distinguishing feature of FAOD is hypoketotic hypoglycemia •MCAD deficiency is most common and has a 25% risk of death with first episode •LCHAD, VLCAD and carnitine uptake disorder are variably associated with, hepatomegaly, liver disease, hypertrophic cardiomyopathy and potential arrythmias •All are autosomal recessive SCAD ketones + acetyl CoA Krebs cycle LCHAD deficiency Hypoketotic hyoglycemia, hypotonia, failure to thrive At diagnosis On dietary treatment Variable Clinical presentations of fatty acid oxidation •Hyoketotic hypoglycemia in neonatal period •Later onset hypoketotic hypoglycemia •Sudden infant death syndrome •Hypertrophic cardiomyopathy, arrythmias •Liver disease •Adolescent or adult onset myopathy •Acute rhabdomyolysis •Asymptomatic Fatty acid oxidation disorders Disease Typical presentation SCAD Probably benign MCAD Hypoketotic hypoglycemia Most common FAOD, may be associated with “SIDS” VLCAD Variable: hypoketotic hypoglycemia, hypertrophic cardiomyopathy, myopathy, liver dz Extemely variable ranging from neonatal to adult onset LCHAD Variable: hypoketotic hypoglycemia, hypertrophic cardiomyopathy, myopathy, liver dz Extremely variable, need low fat diet Comments N/A Diagnosis is based on the specific pattern of acylcarnitine elevations Diagnosis of fatty acid oxidation disorders by acylcarnitine analysis Long chain fatty acid Fatty acid Detected by acylcarnitine analysis Fatty acyl-CoA Fatty acyl-carnitine CPT1 CPT2 CACT FC Fatty acyl-carnitine + (C6-C12) fatty acyl CoAs acetyl CoA Fatty acyl-CoA VLCAD LCHAD 16 14 12 10 MCAD SCAD 4 Mitochondrion Plasma Cytoplasm (C6-C12) Fatty acyl-carnitine ketones Disorders of carnitine metabolism (1) Carnitine transports long chain fatty acids into the mitochondria (2) Carnitine deficiency can be primary or secondary (3) Primary carnitine deficiency is caused by abnormal transport of carnitine itself into the cells (carnitine uptake disorder, AKA “systemic carnitine deficiency”) (4) Secondary carnitine deficiency is causes by other metabolic disorders through the formation of carnitine esters (acylcarnitines) by abnormal organic/fatty acids Primary (CUD) Plasma: Decreased total carnitine Decreased free carnitine Normal acyl/free ratio Urine: Normal total carnitine MCAD, organic acidemias etc Plasma: Decreased/normal total carnitine Decreased free carnitine Increased acyl/free ratio Urine: Decreased/normal total carnitine Normal or increased free carnitine Decreased free carnitine Normal acyl/free ratio Increased acyl/free ratio A 6 day old female who is breast fed is brought to the emergency room due to poor feeding, vomiting and jaundice? Initial laboratory studies show the following: Total Bilirubin 19 136 115 26 4.8 10 0.7 73 Direct bilirubin 5.2 AST 987 ALT 767 Which metabolic disorder do you suspect? galactosemia Which other routine tests should you order? PT, PTT, urine reducing substances How would you confirm the diagnosis? Enzyme assay, DNA How would you treat this patient? Galactose free diet What are the acute and long term complications of this disorder? Liver disease, E coli sepsis, cataracts, MR, speech delay, ovarian failure Galactose Metabolism glucose Breast milk, cow’s milk Lactose (galactose-glucose) Galactose (cataracts) galactokinase epimerase (benign) Treatment: galactose free diet, ophthalmology and developmental followup Gal-1-P UDP glucose galactose-1-P uridyltransferase UDP galactose (classical) Glucose-1-P Glucose-6-P glycolysis pyruvate A 9 year old male is brought to the emergency room due to acute vomiting and lethargy shortly after a birthday party. Past medical history is significant for failure to thrive in late infancy which resolved without determination of a diagnosis. He had had several bouts of vomiting in the past, usually after consuming candy or soft drinks at parties. He has had no dental cavities. Laboratory results in the ER are as follows: Total Bilirubin 6.4 136 115 26 4.8 10 0.7 73 Direct bilirubin 5.2 What is the most likely metabolic diagnosis? Hereditary fructose intolerance AST 767 ALT 987 A 3 month old female is found to have hepatomegaly on routine exam. She is asymptomatic. Lab testing shows hypoglycemia, lactic acidemia, hyperuricemia, hyperlipidemia and elevated AST and ALT. What is the most likely diagnosis? Glycogen storage disease How would you confirm the diagnosis? DNA, liver biopsy What is the treatment? dietary Glycogen Storage Disease 1a “Von Gierke disease” Glycogen Storage Disease 1b facial features weakness hepatomegaly Hypoglycemia, lactic acidosis, hyperuricemia, hyperlipidemia, neutropenia Sibling with same disorder Autosomal recessive Glycogen Krebs cycle Glycogen is a storage form of glucose: Lactic acidosis •Liver glycogen releases glucose into the circulation •Muscle glycogen is used locally Acetyl CoA Glucose – 1- P pyruvate Malonyl CoA gluconeogenesis glycolysis Pentose phosphate shunt Stimulates fatty acid synthesis and inhibits fatty acid breakdown (Hyperlipidemia) Glucose – 6- P ER (hyperuricemia) Glucose cytoplasm Glut 2 plasma glucose Glucose-6phosphatase GSD types 1a and 1b Selected glycogen storage diseases Disease Typical presentation Von Gierke (GSDIa) Hepatomegaly, lactic acidosis, hyperuricemia, hyperlipidemia GSDIb Hepatomegaly, lactic acidosis, hyperuricemia, hyperlipidemia Pompei (GSD II) Weakness, hypotonia, cardiomyopathy Other features Puffy cheeks Puffy cheeks, neutropenia Treatment Nocturnal NG feedings, avoid fasting Nocturnal NG feedings, avoid fasting, neutropenia precautions EKG: short PR intervals, wide QRS Enzyme replacement Debrancher deficiency (GSD III) Similar to Von Gierke but milder, normal lactate Muscle, including cardiac may be involved Similar to GSD1a Brancher deficiency (GSD IV) Fatal liver disease (amylopectinosis) Other organ involvement ? transplant McCardle disease (GSD VI) Only muscle involvement Risk of rhabdomyolysis Avoid excess excercise Patient with developmental regression An infant with apparently normal development for the first 6 months begins to slow down. She was able to sit unassisted by 1 year. She was very socially interactive and could grasp objects. After one year she gradually lost her ability to sit and she could no longer grasp objects. She became less and less interactive, and lost interest in eating and became emaciated. She had splenomegaly. Ophthalmology exam revealed a cherry red spot macula: •What type of disorder do you suspect? Lysosomal storage disease •How would you confirm a diagnosis? Enzyme assay •What is the differential diagnosis of cherry red macula? Lysosomal storage disease: ocular features Lysosomal lipid storage disorders associated with cherry red macula: •Niemann-Pick A •GM1 gangliosidosis •Tay-Sachs disease •Sandhoff disease •Farber lipogranulomatosis •Sialidosis Cell membranes, organelles Bone, connective tissue, skin, cornea,joints etc Mucoploysaccharides (glycosaminoglycans Sphingolipids, glycolipids etc Glycoproteins Glycogen Food particles Acid hydrolases Lysosome Abnormal lysosomal storage leads to developmental regression “The cells wrecking crew” Bacteria, viruses Metachromatic Leukodystrophy •Rapid developmental regression starting in late infancy •Lysosomal accumulation of sulfatides GM1 Gangliosidosis Neonatal presentation: hypotonia, ascites A 14 month old female presented with developmental delay to your clinic. She was reportedly normal at birth but at 8 months was noted to have mild kyphosis when sitting. She had a history of chronic rhinorrhea. Late in infancy, the parents noticed gradual changes in craniofacial features including thickening of the eyebrows, large tongue, prominence of forehead. The patient been pulling to stand but lost this ability and seemed to be regressing in overall development. On exam, you notice a scaphocephalic head shape, frontal bossing, relatively thick eyebrows, cloudy cornea and stiff elbows. The patient most likely has a disorder within which category of inborn error of metabolism? Lysosomal storage disease (mucopolysaccharidosis) How would you confirm a specific diagnosis? Enzyme assay Mucopolysaccharidosis • Hurler Syndrome: comparison with sibs Hurler syndrome Mucopolysaccharidosis • Hurler syndrome – alpha L-iduronidase def. organomegaly Sanfilipo Syndrome (MPS 3) • facial features •Sanfilipo (MPS III) •Less severe somatic features •Developmental delay •Behavioral problems •Neurological regression Maroteaux-Lamy (MPS VI) Maroteaux-Lamy (MPS VI) Morquio (MPS IV) Lysosomal storage disease: laboratory diagnosis •Urine mucopolysaccharides •Urine oligosaccharide •Enzyme assay •DNA (for genetic counseling and to rule out pseudoalleles) Disease Typical presentation Hurler (MPS1) Developmental regression, dysosotosis multiplex, cloudy cornea, organomegaly, cardiac valve disease Hunter (MPS2) Similar to Hurler but no cloudy cornea San Filippo (MPS3) Later onset, mild somatic features Inheritance Treatment Autosomal recessive BMT/ERT X-linked BMT/ERT Autosomal recessive Morquio (MPS4) Mainly skeletal involvement Autosomal recessive Maroteaux-Lamy (MPS6) Similar to Hurler but “CNS sparing” Autosomal recessive ?ERT BMT/ERT PKU Adult with Mental Retardation: born before newborn screening era PAH Dietary protein Phe Tyr Neurotransmitters, melanin etc •Phenylalanine hydroxylase defect •Autosomal recessive •Normal infant at birth Severe mental retardation, microcephaly, behavioural problems PKU: Clinical Problems if Untreated • mental retardation • seizures • hypopigmentation • rash Tx: low phenylalanine diet *Due to newborn screening, the above problems rarely occur. “Guthrie cards” Heel stick: •Obtain at about 48 hours •If obtained too early, false negative Filter paper with blood spots and demographic information Phenylketonuria Patients with PKU: low Phe diet, frequent monitoring of Phe, dietary counseling •Studies have shown that NBS has virtually eliminated mental retardation due to PKU Normal growth and development Selected Presentations/Diagnostic Considerations Lysosomal storage (glycolpids)) DEVELOPMENTAL REGRESSION ORGANOMEGALY CHERRY RED MACULA RESPIRATORY ALKALOSIS HYPERAMMONEMIA Lysosomal storage (MPS) DEVELOPMENTAL REGRESSION SKELETAL DYSPLASIA ORGANOMEGALY VARIABLE CLOUDY CORNEA ORGANIC ACIDEMIA HYPOGLYCEMIA HEPATOMEGALY INFANT/CHILD WITH SUSPECTED METABOLIC DISEASE GLYCOGEN STORAGE DISEASE (MUSCLE) GLYCOGEN STORAGE DISEASE (LIVER) HYPERCHLOREMIC METABOLIC ACIDOSIS LIVER DISEASE CATARACTS HYPERBILIRUBINEMIA REDUCING SUBSTANCES GALACTOSEMIA UREA CYCLE DISEASE WIDE ANION GAP METABOLIC ACIDOSIS, KETONURIA, HYPERAMMONEMIA WEAKNESS RHABDOMYOLYSIS KETONES NEGATIVE ENCEPHALOPATY < 24 HRS OLD, BURST SUPPRESSION EEG NON KETOTIC HYPERGLYCINEMIA METABOLIC ACIDOSIS HYPOGLYCEMIA INAPPROPRIATELY LOW KETONES FATTY ACID OXIDATION DEFECT