Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Cardiac surgery wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Atrial septal defect wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
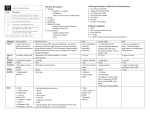
Mitral Facies Sometimes patients with mitral stenosis have a dusky red or purple tinge to their cheeks. This sign is neither sensitive (as many patients with mitral stenosis do not have it) nor specific (as there are many other reasons for this appearance). It results from dilated small blood vessels within the skin over the cheeks. When it does occur, it is usually associated with moderate or severe mitral stenosis and many believe it is a result of longstanding pulmonary hypertension, because other causes of pulmonary hypertension may also lead to this appearance. A chronically low cardiac output, associated with severe mitral stenosis may also contribute. Other causes of a “malar flush” “Weather-beaten” appearance- eg farmers working outside for prolonged periods Pulmonary arterial hypertension from other causes, sometimes associated with hypoxia causing secondary polycythaemia • Polycythaemia rubra vera • Idiopathic / constitutional • • Link with pulmonary hypertension Although referred to as “mitral facies” it is NOT associated with mitral regurgitation (MR), and this may help explain the aetiology because MR is not usually a cause of pulmonary hypertension. The mechanism by which mitral stenosis causes pulmonary hypertension is summarised in the diagram: Mitral stenosis High LA pressure Pulmonary venous hypertension Pulmonary arterial hypertension Right ventricular hypertrophy Dr R Clarke Loud HS1 Kerley B lines Loud P2 Prominent “a” wave in JVP +/- pulmonary regurgitation Left parasternal “heave” Tricuspid regurgitation “v” wave in JVP Right heart failure Raised JVP oedema, ascites www.askdoctorclarke.com 1 Why do vessels dilate? The precise reason why vessels in the skin dilate and form abnormal anastomoses is not clear, but may well be due to a combination of hypoxia, polycythaemia and reduced cardiac output. Clinical implications The main clinical implication is to note such skin changes over the cheeks and to make a careful check for mitral stenosis in such a patient, looking for: Pulse- atrial fibrillation (very common), sometimes reduced pulse volume in severe stenosis JVP- prominent “A” wave Apex- tapping due to loud first heart sound RV- may be prominent left parasternal impulse if pulmonary hypertension Auscultation: Diaphraghm: loud first heart sound + opening snap if valve still mobile + loud pulmonary second sound if pulmonary hypertension present. Bell: localised rumbling murmur at apex with bell lightly applied. NB: Graham Steele murmur: this is an early diastolic murmur of pulmonary regurgitation secondary to severe pulmonary hypertension. Dr R Clarke www.askdoctorclarke.com 2