Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac surgery wikipedia , lookup
Jatene procedure wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
The Splitting of the Second Heart Sound in Normal
Subjects and in Patients with Congenital Heart Disease
By MAURICE M. AYGEN, M.D.,
AND
EUGENE BRAUNWALD, M.D.
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
with other forms of congenital heart disease
(2) to provide hemodynamic-phonocardiographic correlations in these patients, (3) to
demonstrate the effects of successful surgical
closure of ASD on the splitting of the second
heart sound, and (4) to present observations
that provide an explanation for the mechanism of splitting of the second heart sound in
normal subjects and in patients with ASD.
Clinical Material
ROUANET, in 1832, demonstrated that the
second heart sound results from closure
of the semilunar valves.1 In 1865, on the basis
of clinical observations, Potain indicated that
the second heart sound may be split into two
components and that the degree of this splitting may vary with respiration.2 More recently the studies of Leatham and collaborators3 4 have focused considerable attention on
the splitting of the second heart sound and,
at the present time, precise characterization
of this sound is of prime importance in auscultation of the heart. A physiologic basis for
the interpretation of this auscultatory finding
was first provided by Katz, in a study in
which the timing of the dynamic events of the
cardiac cycle in the two sides of the heart was
determined, and slight asynchronv in the closure of the semilunar valves was noted.5 These
observations were subsequently extended to
human subjects with normal cardiovascular
systems, in whom it was observed that pulmoniic valve closure followed aortic valve
closure by 0.028 + 0.010 second.6
It is now well established that in normal
subjects as well as in patients with many
forms of heart disease, the time initerval between the sounds of aortic and pulmonary
valve closure inereases with inspiration.3 4 7
It has been reported that in patients with
atrial septal defects (ASD) this time interval
is longer than in normal subjects during expiration and shows relatively little change
during the respiratory cycle.8-10 The mechanisms responsible for these abnormalities are
still under debate. The purpose of the present
report is (1) to supply measurements of the
effects of respiration and of the Valsalva
maneuver on the second heart sound inl normal subjects, in a large series of patients
proved to have ASD, as well as in patients
F'rom the Cardiology Branch, National Heart Insti-
This study is based on an analysis of the phonocardiograms obtained from 350 patients studied
at the National Heart Institute between 1958 and
1961. The diagnosis was considered to be firmly
established in every instance by means of detailed
clinical examination and specialized studies. Right
heart catheterization was performed on all patients
with functional heart murmurs and congenital
heart disease. In these patients the presence of
a left-to-right shunt was detected by either the
nitrous oxide1' or the inhaled Kr85 test.'2 In
addition, all patients had dye-dilution curves further to characterize their circulatory shunts. The
patients with aortic stenosis were all studied by
left heart catheterization, which was generally
carried out by the transbronchial, transseptal, or
anterior percutaneous technic.13 The diagnosis was
confirmed at operation in 194 of the 350 patients.
The age range for each group of patients reported
is presented in table 1.
As indicated above, particular attention was
directed to the effects of operation on the behavior
of the second heart sound of patients with ASD.
Preoperative and postoperative phonocardiograms
were available for analysis in 31 patients, all of
whom were operated upon with the aid of extracorporeal circulation; 29 had the ostium secundum
or sinus venosus type of defect, while two had
ostiumn primunii defects, i.e., a low atrial septal dedect with a cleft in the mitral valve. The postoperative phonocardiographic and cardiac catheterization studies were carried out 3 to 12 months
after the operation.
All phonocardiograms were taken on a SanbornTwin beam photographic recorder at a paper speed
of 75 mm. per second ultilizing a logarithmic amplifying system. The recordings were obtained from
the four valvular areas, and the tracing in whieh
the second heart sound was most clearly defined
tute, Bethesda, Maryland.
328
Circulation, Volume
XXV, February 1962
329
SPLITTING SECOND HEART SOUND
A2-P2 INTERVAL
J+60
(mta I
INSPI RATORY
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
-P2
1
+40
CHANGE OF
INTERVAL
-10
-lo
-20
INSPIRATORY
+10
CHANGE
OF
+20
+30
Q-A2 INTERVAL (msec)
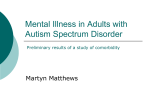
Figure 1
Effects
the
of
inspiration
abscissa,
ordinate.
snplitting
normal
with
and on
The
of
the
who
second
from
had
the
duration
duration
diagnoal
subjects
ASD
on
the
of
left
of right
ventricular
systole
of
lines
demonstrate
the
hea!rt
sound.
broken
patients
with
pulmonary
The
ASD.
artery
puronary/systemic flow ratios less
than
was employed in the analysis. An electrocardiographic lead and indirect carotid pressure pulse
were utilized for timing reference. Recordings were
obtained during continuous spontaneous respiration and in many patients during and immediately
Circulation, Volume XXV, February 1962
systole
ventricular
effects
The
mean
solid
triangles
pressures
1.t/f.0,
or
line
in
along
on
width
the
separates
represent
eA.cess
allong
plotted
inspiration
diagonall
plotted
(Q-A2)
(Q-P2)
of
most
of
the
of
the
those patients
50
rm.
Hg
or
both.
after the Valsalva maneuver. In determining the
time intervals between aortie and pulmonic valve
closure, the longest interval recorded during
inspiration and the shortest interval recorded
during expiration in a single respiratory cycle
AYGEN, BRAUNWALD
330
500
400
Table 1
Diagnosis and Age Distribution of Patients Studied
I1
Number
operNumber Ages (years)
studied Range Average ated
-
51
Normal
I118
Atrial septal defect
Pulmonic stenosis
30
Ventricular septal defect 68
Ventricular septal defect
with pulmonic stenosis
Tetralogy of Fallot
Aortic stenosis
Patent ductus arteriosus
Total
(msec)
300
200 _
100 _A2- P2
O,L_
14.2
27.1
14.1
20
11.9
40
2 23
12.0
5.8
13.7
12.8
3
3-9
4-32
2-41
0
80
6
30
13
194
I
mr-
v,
400
4-49
3-65
1-36
2-40
600
800
1000
1200
1400
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
PRECEEDING R-R INTERVAL (msec)
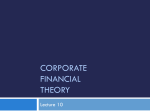
Figure 2
Relationship between the preceding R-R interval
and Q-P2, Q-A2, and A2-P2 in patient with ASD
and atrial fibrillation.
a
were utilized for analysis. All measurements were
made from the onset of the QRS and of each
component of the second sound. The error of
measurement was considered to be below 0.005
second.
In the performance of the Valsalva maneuver
the subject was asked to expire against a closed
glottis with the chest in the mid-respiratory position for a period of several seconds, and then to
relax without inspiring. The phonoeardiographic
observations were carried out during and immediately after the Valsalva maneuver for a total of
8 to 10 cardiac cycles.
Results
Effect of Respiration on Q-A2, Q-P2, and A,-P2
In the 51 normal subjects the changes in
the duration of the interval from the onset of
ventricular depolarization to the aortic valve
closure sound (Q-A2) during inspiration
ranged from -20 msec. to +10 msee. and the
average change was -5.2 msec. (fig. 1). Q-P2
increased during inspiration in all but one of
these subjects. The maximum increase was 50
msec. while the average increase was 32.6
msee. The time interval between aortic and
pulmonic valve closure (A2-P2) increased in
all of the normal subjects, these increases
ranging from 10 to 60 msee., with an average
increase of 37.8 msec.
In the patients with ASD a pattern differwas observed. The inspiratory increase of Q-P2 averaged only 4.6
msee. for the entire group, with an increase
less thIan 20 msee. in 112 patients. Q-A2
showed no change during respiration in eight
of the 118 patients, and in the remainder it
increased or decreased up to 20 msec. The
change in A2-P2 was much less during respiration than in the normal subjects. In 87
patients there was no change, and in 28 there
was an increase of only 10 mnsee. In three patients the increase of A2-P2 equaled 40 msee.,
and they had either pulmonary hypertension
(pulmonary artery mean pressure greater
than 50 mm. Hg) or small left-to-right shunts.
with pulmonary to systemic flow ratios less
than 1.5/1.0 (fig. 1).
Although Q-P2 and A2-P2 showed little
change with respiration in patients with ASD,
alterations in the duration of the preceding
R-R interval resulted in significant changes
in these time intervals. Phonocardiogramns
were recorded at a constant respiratory position in four patients with ASD in whom atrial
arrhythmias resulted in marked beat-to-beat
variations in the R-R intervals. A representative result is plotted in figure 2 in which it is
evident that as the preceding R-R interval
lengthened, Q-P2 increased more than Q-Ao
and, therefore, A2-P2 increased.
ent from the normal
Relationship between Heart Rate and the Duration
of Systole
The relationship between heart rate and the
Circulation, Volume XXV, February 1962
331
SPLITTING SECOND HEART SOUND
,
~~~I
,
1
500
A
4501
_
0-
P2
~~
A
_
AM
~~~~~~~~A4
^~~
INTERVAL 4001
DURING
EXPIRATION
(MSEC)
A^aM
A~~~~~~~~~
A
A
~ ~~~A
~
A
~ ,
A
Ab A
_
/A
AAA^t~AA
@.
A
A~ AA
AsA
A< b
*
MA
A
A
AAK ^
A/ a
&//.
A
*
A4
0
-
@
*
0
A
A
A
_
a
350[
A__-
A
<
A
*
~
*
A
A
A
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
NORMAL
1 ASD
300
0
~~~~~~~~~~
130
120
100
110
90
80
60
70
50
HEART RATE/MIN
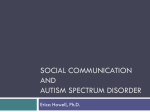
Figure 3
Relationship between heart rate and
and patients with ASD.
Q-PI, recorded during expiration
time interval from the onset of ventricular
depolarization to the pulmonic valve closure
sound (Q-P2) in normal subjects and in patients with ASD during expiration is shown
in figure 3. It is clear that there is an inverse
relationship between heart rate and Q-P2 in
both groups of patients. The broken line outlines the highest values for Q-P2 encountered
in the normal subjects. Although at any given
heart rate there was considerable overlap between the values for Q-P2 in the normal subjects and in the patients with ASD, 62 of the
118 patients with this malformation had values of Q-P2, which exceeded the highest values
observed in normal subjeets at similar heart
rates. Similarly, 16 of the 30 patients with
pure pulmonic stenosis (PS), 12 of the 67
patients with ventricular septal defect (VSD)
and eight of the 10 patients with combined
VSD and PS also had prolongation of Q-P2
above the greatest normal values. The other
patients with the malformations listed above
had values in the normal range. The Q-P2 and
Q-A2 intervals in patients with congenital
Circulation, Volume XXV, February 1962
in normal subjects
aortic stenosis (CAS) and patent ductus arteriosus (PDA) also tended to be related inversely to the heart rate but showed no consistent deviation from the normal.
Effect of Valsalva Maneuver
A2-P2
on
Q-A2, Q-P2, and
In general, release of the Valsalva maneuexaggerated the effects of inspiration in
normal subjects (fig. 4) but had relatively
little effect on Q-P2, Q-A2, and A2-P2 in patients with ASD (fig. 5). In the normal subjects release of Valsalva increased Q-P2 by 15
to 75 msee. (av. = 40.7 msec.) ; Q-A2 changed
by -30 to +10 msec. (av. = -9 msec.); A2-P2
increased by 20 to 80 msee. (av. = 49.7 msec.).
In contrast, in the 42 patients with ASD studied, the change of Q-A2 after release of the
Valsalva maneuver ranged from -20 to +20
msee. (av. = +1.4 msec.) ; the change of Q-P2
ranged from -10 to 50 (av. = +4.7 msec.)
and A2-P2 increased by an average of only
3.3 msec. (fig. 6). Thus, it is evident that
analysis of changes in Q-A2 and Q-P2 following release of Valsalva permits separation of
ver
332
.L@sve t,;e>/'\+_^-
A2
:LT.4 laCes.
E
NoE1
'.."
:1
t"
I
.A
AP
S1
.
r- -r ~~~~~~~~~-
1.
-1 U
.
-- -.
-
. . . -N
'.
S
--
- --N
-1
7-1.4-
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
A2
LT. 4 t.C.S.
:...
J.1
-iNA
_..I
kA 6&
I
_1VOilk
_- --
--
I
rw
-VP
Iv"rm
vr-I
--
-
I Ir
y
w
...
1.
w _o. ;
4 :::.4::
Aa arrI
A_ _+
.
5_
,"
b:!
*
8
A.. t
s° wL
t
.....
I
SL
-
L
.
AI A--
L
f
8
A
...........
.VA
v
-I
rep)res(utatire phonocardl(fio('(firlrecorde(d
i
lrs.,left fourthi intercostal
_T4
t..+.._...
4.ALV_A
Figure 4
fromn
a
normal
(top) aind the Valsalra mnurneuver (bottomii). SI, 1st heart
x
+
ffi
t
0
r
-. t-
I
..
i
+
?
._+_..
:PS. *03-06-51
A
J
5_._ e
3
is
F v
i
4
4
s
W
.w
_
-
Y
Ar
--. ,}----5 ---- - -
-Y A
-
e
I.
...
J
ft
CE :: ;:tv
..
_
I~ _.
.- -1.'i -.- 44
__48.z.... .A..
+,
^
;i_
.1
-,
-
M--- rP
,
--1
I
I
1.
... a
* .
A2 P2
E
J
AP2
A Pt
St.
It
717..-i-i
._°+AV: w;S-E
AYGEN, BRAUNWALD
s
+.
e ^4
t;
.. ._.f, ,i,t X
g
subject during respiration
sound;
F,,
ejection sound, LT.
spa(e.
normal subjects fromn patients with ASD.
Again the )atieLlts with this malformation
whose values were similar to those encountered in niormal subjects had severe pulrnonlary hypertenision or a very small left-to-right
shunt.
A2-P2 during the Respiratory Cycle
Normal Subjects
During expiration in normal subjects A2-P2}
ranged from 0 to 40 msec., with anl average
of 10.6 insee. (fig. 7). As already indicated,
this time interval increased during inspiration in all these subjects. In general there
was an inverse correlationl between A2-P2 dur-
ing expiration and the augmenitation of this
iinterval durinig inspiration (fig. 7).
ASD, Preoperative
In patieents with ASD the expiratory A2-P2
tended to be greater than in the normal subjects and averaoed 50.2 msee. The inspiratory
augmentation of this interval was less than
in normal subjects. One hundred and thirteen
of the 118 patients with ASD had expiratory
A2-P2 intervals of at least 30 msece. and an
inspiratory auglmentation of less than 20 msee.
but only one normal subject had an A2-P2 interval that fell withlin these limits. Of the five
patients with ASD who did not fall into these
Circulation. Volume XXV, February 1962
s
-rrv
33
SPLITTING SECOiND HEART SOUND
*~~~~E
E
il
Ii -M
rUT1fl7TTfflTTt~~~~LIii.tI
7
010
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
2
S M
-Ak
LT. S I
S.
i . im4w
O'
,1.
...
.... ....
...
v
VA
J.
11 S m
0m
A
R
S
S m
D
-00A"
.1
44
T.7-
A
%AI
Figure 5
Phoi,iocai-diogram, recorded iiz the secoiid le ,ft intercostal space (LT. 2 i.c.s.) in a patient
with ASD du?-iizg respiration (top) (iiid the Valsalra maiw?tcer (eenter). I'he bottom
tracing shows a simitltaizeous iizdirect carotid pulse trachig ajid the broken vei-tical Iiiie
above the incisura identifies A2- S-11, systolic ?nu)-?)zu?,; D.11, diastolic murmur.
limits three had severe pulmonary
y
sion
both
or
as
small
defined above
oill
a
hyperten-
left-to-right shunt,
(flo,. 7).
Circulation, Volume XXV, February 1962
or
A2-P2duringr iiorirnal
and immediately after release of
The averacre values for
n
respiration,
the Valsalva
maneuver
in the normal
subjects
334
3AY GEN, BRAUNWALD
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
CHANGE OF
Q -P2 INTERVAL 40
AFTER RELEASE
OF VALSALVA
|
0
0/
I0
-20 2
-0
+30
+20
0
+ t0
-20
-30
-10
CHANGE OF Q-A2 INTERVAL AFTER RELEASE OF VALSALVAI(MSEC)
Figure 6
Effects of release of the Valsalva maneuver on Q-A2, Q-P2, and A 2-P2. For explanation see
legend of figure 1.
and in the patients with ASD are summarized
in figures 8 and 9.
A SD, Effect of Operation
At the time of the postoperative catheterizations it was observed that the left-to-right
shunts had been completely abolished in 29
of the 31 patients with ASD. In the other two
patients the magnitude of the shunit was reduced from the preoperative level but it had
not been completelv eliminated. There was a
distinct tendency for A2-P2 to return to normal limits following successful surgical dloCirculation, Volume XXV, February
1962
335
SPLITTING SECOND HEART SOUND
INSPIRATORY
INCREASE OF
A2-P2 INTERVAL
(msec)
40I&
A,A
*
A.S.D.
Normol
30
20
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
I0
I AA
A
0
0
10
50
60
70
80
30
40
A2P2 INTERVAL DURING EXPIRATION (msec)
20
9( 0
100
Figure 7
A2-P2 during expiration, plotted along the abscissa, and the increase of this interval during
inspiration, plotted along the ordinate. The absolute duration of A2-P2 during inspiration
is equal to the sum of the two values plotted.
sure (figs. 10 and 11). A decrease in A2-P2
during expiration occurred in 29 of the 31
patients; one of the two exceptions had pulmonary hypertension and normal splitting of
the second heart sound prior to operation.
Following complete closure of the defect the
inspiratory increase of A2-P2 exceeded 10
msee. in 26 of the 29 patients. The two patients with residual left-to-right shunts exhibited a decrease in the expiratory A2-P2 interval from that observed preoperatively, but
showed an augmentation of only 0 and 10
msec. respectively during inspiration (fig. 10).
Thus, in the postoperative period both of these
patients exhibited splitting of the second
heart sound, which was indistinguishable from
that observed in patients with unoperated
ASD (fig. 7) but which could be differentiated
from the pattern of splitting observed in those
patients whose defects had been successfully
closed.
Circulation, Volume XXV, February 1962
Pulmonic Stenosis
The expiratory A2-P2 interval and its augmentation during inspiration in the normal
subjects and in the patients with pulmonic
stenosis (PS) is plotted in figure 12. During
expiration A2-P2 was less than 40 msee. in 46
of the 51 normal subjects and in all six of
the patients with PS whose peak systolic pressure gradients between the right ventricle
and pulmonary artery were less than 20 mm.
Hg. In contrast A2-P2 during expiration
equaled 40 msee. or more in all 24 patients
with PS whose pressure gradients exceeded
20 mm. Hg. During inspiration the augmentation of A2-P2 was within normal limits in
these patients (fig. 13).
Aortic Stenosis, Patent Ductus Arteriosus
During expiration A2 and P2 were fused
and occurred synchronously in 38 of the 44
patients with congenital aortic stenosis (AS).
In the other six patients A2 followed P2 by
AYGEN, BRAUNWALD
336
Table 2
Systemic and Pulmonary Arterial Oxygen Saturation in Patients with ASD
Patients
Age
(years)
Arterial
02 sat.
_
NORMAL
P.A. 02 sat. P.A. 02 sat.
during insp. during exp.
91.4
85.0
94.6
13
G.G.
82.7
77.2
93.2
7
F.D.
85.9
83.0
93.0
39
P.S.
91.5
90.0
22
99.0
H.J.
88.8
85.8
19
97.0
K.E.
90.0
88.8
8
92.9
M.M.
12
90.0
88.0
96.0
M.A.
88.0
94.0
84.0
9
L.B.
88.8
85.2
95.0
Mean
ASD, atrial septal defect; Insp., inspiration; Exp.,
expiration.
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
20 to 40 msee., i.e., the A2-P2 interval was
negative (fig. 14). In 21 patients with AS
there was no inspiratory increase of A2-P2.
In the others this increase ranged from 10 to
60 msee., as in the normal subjects. When the
combination of A2-P2 during expiration and
the change of this interval during ilnspiration
are considered, it was observed that 29 of the
44 patients with congenital AS fell ontside
the range encountered in the normal subjects
(fig. 14). In 12 of the 15 patients with AS
in whom A2-P2 fell into the normal range, the
peak systolic pressure gradients between the
left ventricle and brachial artery measured
at left heart catheterization was less than 75
mmn. Hg.
The behavior of the second heart sound in
patients with PDA resembled that observed
in patients with congenital AS. During expiration A2 and P2 were fused in eight patients, neaative in four, and positive in only
one patient. When the combination of the expiratory A2-P2 and its change during inspiration was considered, seven of the 13
patients with PDA fell outside the range
encountered in the normal subjects (fig. 14).
Other Malformations
In patients with ventricular septal defect
(VSD), the relationship between the two components of the second heart sound was observed to fall into the normal range with only
an occasional exception. There was a lower
incidence of a single second heart sound dur-
j
*-EXPIRATION-|- - INSPIRATION
MSECI
20
1--4
Q--p2
.
~
St.4I0.6
,1
~~
lo|
o
I
ASD
-EXPIRATION
M
II
SECl_4-
*
-
I
-
INSPIRATION
t
2
3
4
5
6
HEART BEAT
Figure 8
Average values for A2-P2 during respiration in
normal subjects and patients with ASD.
ing expiration in the patients with VSD and
large left-to-riaht shunts than in the normal
subjects.
In 16 patients with PS, VSD, and a rightto-left shunt (tetralogy of Fallot) only one
component of the second heart sound could
be recorded; simnultaneous carotid pulse tracings ilndicated that this was the sound of
aortic valve closure (A2).
Effect of Respiration on Pulmonary Arterial
Satur.-Ition in Patients with ASD
Oxygen
In order to elucidate the mechanism responsible for the relative constancy of A2-P2 during respiration in patients with ASD, blood
samples were withdrawn from the pulmonary
artery first during inspiration and then during expiration. Several respiratory cycles
were required to obtain each sample, and the
oxygen saturatiolns were determined by the
manometric method of Van Slyke and Neill.
In each of the eight patients studied, the pulmonary arterial oxygen saturation during
expiratioln exceeded the saturationl during inspiration (table 2); the average difference in
saturation was 3.6 per cent. The oxygen saturation of mixed venous blood proximal to
the entry of the left-to-right shunt was calculated from the arterial oxygen saturation and
Circulation, Volume XXV, February 1962
33S7
SPLITTING SECOND HEART SOUND
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
the pulmonary/systemic flow ratio determined
by the Kr85 test.'4 Assuming the durations of
inspiration and expiration to have been equal,
it was then possible to calculate the shunt/
systemic flow ratio during both phases of the
respiratory cycle. In each of the patients this
ratio was greater during expiration (av. =
1.80/1.00) than during inspiration (av. =
0.64/1.00).
Discussion
In the present study the onset of ventricular depolarization (the Q wave of the electrocardiogram) was chosen as the reference
point for all measurements, since this point
can be easily recognized on all tracings. The
time interval between the onset of ventricular
depolarization and of closure of either of the
semilunar valves (Q-A2 and Q-P2) actually
represents the sum of three periods: (1) the
interval between the onset of ventricular depolarization and the onset of ventricular contraction, (2) the duration of isometric ventricular contraction, and (3) the duration of
ventricular ejection. The first two of these
periods remain virtually constant under a
wide variety of conditions and constitute only
a small fraction of the total interval between
the Q wave and the second heart sound. It is
considered that in the absence of gross abnormalities of intraventricular conduction,
changes in Q-P2 and Q-A2 represent changes
in the duration of right and left ventricular
ejection respectively.
Consideration of the well-established fact
that the duration of ventricular ejection varies directly with the stroke volume15 permits
explanation of the observed effects of respiration and of the Valsalva maneuver on the
splitting of the second heart sound in normal
individuals. Inspiration augments the inflow,16
the effective filling pressure,'7 the end-diastolic volume,18 and the stroke output'9 of the
right ventriele and has an opposite but
smaller effect on the left ventricle.'9 This
explains the prolongation of Q-P2 and the
simultaneous shortening of Q-A2 during inspiration, resulting in an increase in A2-P2. It
has been suggested by Boyer and Chisholm20
and more recently by Shafter2' that in normal
Circulation, Volume XXV, February 1962
I
I
ASD
-VALSALVA-1-POST
VALSALVA-
r--<
1~20 _
M SEC (gPZ
-
.
I_
51.9
56.2
*0
1
_
0-
4
5
6
_
.1
I
2
3
HEART BEAT
Figure 9
Average values for A2-P2 during and immediately
after release of Valsalva in normal subjects and
patients with ASD.
individuals the inspiratory abbreviation of left
ventricular systole is approximately equal to
the prolongation of right ventricular systole.
The observations on normal subjects presented
in figure 1 are not consonant with these views.
Of the average inspiratory increase of A2-P2
of 37.8 msee., 32.6 msec. or 86 per cent was
contributed by prolongation of right ventricular systole and only 5.2 msee., or 14 per cent,
by shortening of left ventricular systole. In
only seven of the 51 subjects did the shortening of left ventricular systole during inspiration equal or exceed the prolongation of
right ventricular systole. The observation that
during respiration the duration of left ventricular systole is altered far less than the
duration of right ventricular systole is also
consistent with the experimental observations
that the respiratory variations in the filling
and stroke volume of the right ventricle exceed those of the left.'9
The abnormally wide splitting of the second
heart sound in patients with ASD is a wellknown clinical sign.8 9, 22 It was suggested
that the alterations in the pattern of right
ventricular depolarization commonly observed
in patients with this anomaly may account for
AYGEN, BRAUNWALD
338
INSPI RATORY
INCREASE OF 4
A -P INTERVAL
(msec)
30
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
20
0
l0
50
80
60
70
40
(msec)
AP2 INTERVAL DURING EXPIRATION
20
30
9l 0
100
Table 10
interval during expiration and the increase of this interval during inspiration in
patients with ASD prior to and following operation.
A2-P2
the delay in pulmonic valve closure. However,
hemodynamic studies in patients with ASD
and so-called "incomplete right bundle-branch
block" have clearly established that there is
no prolongation of the time interval between
the onset of ventricular depolarization and
of right ventricular contraction.9 23 In addition, the observations of Leatham8 and of
Perloff and Harvey,24 have shown that following surgical closure of ASD the splitting of
the second heart sound often demonstrates a
normal pattern while the electrocardiographic
changes characteristic of this malformation
persist.
As shown in figure 3, at any given heart
rate, right ventricular systole tends to be
longer in patients with ASD than in normal
subjects. In patients with this malformation
the stroke volume of the right ventricle is
abnormally large and exceeds that of the left
ventricle. All these considerations suggest
that prolongation of right ventricular ejection
is responsible for the abnormally wide split-
ting of the second heart sound in these patients.
Another important characteristic of the
second heart sound in patients with ASD is
that the wide splitting tends to show little variation during the respiratory cycle. Leatham
and Gray observed no measurable change in
the time interval between the two components of the second heart sound in 21 of 30
patients with ASD,8 whereas Shafter found
that among 16 patients the maximum change
with respiration was 29 msee.A In the present
series of patients with ASD it was observed
that in 87 there was no measurable change in
A2-P2, and that in 30 there was an increase of
5 to 10 msec. The three patients with larger
changes had severe pulmonary hypertension
and only small left-to-right shunts (figs. 1
and 7).
The mechanism for this tendency of the
splitting of the second heart sound to show
little, if any, variation during the respiratory
cycle is not clear. Leatham and Gray considCirculation, Volume XXV, February 1962
339
SPIjITTING SECOND HEART SOUND
MM
Al
Agl fP
.T
'TTIM rrrTqM'W "I
-ITIT -V-" "
i L LiSui.
T 'FM
- -LA
-A
AA.
f 44000-- --pON
POST OP
Vtu{-;:0Ii
"Opt1'
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
1 I I-
I Vp..A
-
±AliLInAHLLLHnLd Inso
1
mm .- -
"|
Pa'
Aa
i I.--h
nt
-AiW.L-
-
a
Vf]-'
11PPP1
-II
7l11F.
,.A -
iFui971
I]
.w
I0
I1
TTIT,Fj
Figure 11
Phonocardiogram recorded prior to (top) and folloving (center and bottom) szccessful
surgical closure of an ASD. Preoperatively there is wide, fixed splitting of the second
sound. Postoperatively the second sound is single during expiration and the Valsalva
maneuver.
ered the inequality of right and left ventricular outputs to be the responsible factor.8 It
has also been suggested that in these patients
the "overfilled" right ventricle cannot further au(gment its filling during inspiration
and therefore does not inerease its stroke volume.24 If this hypothesis were correct, however, it would be anticipated that the duration
of right ventricular ejection would be shortened when the systemnic venous return is impeded by prolonged expiration or by the Valsalva maneuver.
It has been shown by Perloff and hTarvey24
as well as in figure 2, that the duration of
right ventricular systole in patients with ASD
does not always remain constant. Tn the presence of changes in the duration of diastole (lue
Circulation, Volume XXV, February 1962
to atrial arrhythmias, Q-P2 and A2-P2 were
found to increase with the R-R interval. In
the same patients no variation in A2-P2 was
observed throughout the respiratory eycle.
Thus it is apparent that when changes in
right ventricular fillinlg do occur in patients
with ASD the duiration of righlt ventr-icular
ejection and the degree of splitting of the
second heart sound may be altered.
Au alternative explanation for the tenideney
to fixation of splitting of the, second heart
sound in patients with ASD is that (duiring
the respiratory cycle the two venous systems
(systemic and pulmonary) that contribute
blood to the right ventriele vary the manitude of their contributions reciprocally. As
already mientioned, in normial subjects the in-
AYGEN, BRAUNWALD
QA0
7rl.
r
.
.I
19 ^
l
I lI
I
I
'I.~~~~~~~~~~~~~~~~~~~~~~~~~~~
50
I
* Normal
Pulmonic Stenosis
Gradient>20mm Hg
0 Pulmonic Stenosis
Gradient < 20 mm Hg
I
60
I
@00
I NSPIRATORY 40
INCREASE OF
AiPINTERVAL
RMSEC)
30
*
*
l0
_
°-
ON
oW
we
*t
@0
20
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
10
I
0
0
0
000
0
000
0
0
0
00
0
0
0
0
000
OSO
@0
O
00
II
I
I.
0
10
20
30
40
50
60
70
80
90
100
A2-P2 INTERVAL DURING EXPIRATION (MSEC)
Figure 12
A2-P2 during expiration and increase of this interval during inspiration in normal subjects and patients with PS. The broken vertical line separates the majority of these
patients.
flow of blood into the right heart from the
systemic venous bed is augmented during inspiration and a decline in filling of the left
side of the heart takes place simultaneously.
It is suggested that this sequence of events is
not disturbed in patients with ASD. If one
considers that in these patients the two atria
form a common reservoir for the filling of the
ventricles, then the effect of inspiration on
the stroke volume of the ventricles would be
determined by the net effect of inspirations
on the inflow into this common atrial reservoir. When the inspiratory augmentation of
the systemic venous return is balanced by an
equal decrease in pulmonary venous return,
no significant inspiratory change of inflow
into the atrial reservoir, of ventricular filling
and discharge and, therefore, of Q-P2, Q-A2,
and A2-P2 would be expected. Indeed, no
change in these intervals was observed in 63
of the patients with ASD studied. However,
if there is a net augmentation of inflow into
the atrial reservoir during inspiration, an increase of the filling and discharge of the ventricles and a prolongation of both Q-A2 and
Q-P2 would be expected; in 25 of the patients
with ASD there was an inspiratory increase
of both Q-P2 and Q-A2. If the inspiratory
decline in pulmonary venous filling exceeds
the simultaneous augmentation of right ventricular filling, then a shortening of the
duration of ventricular ejection would be expected; this occurred in only two patients.
Under all circumstances, the exact distribution of blood between the two ventricles depends on the relative compliance of these
chambers during diastole.25
If, as described above, respiratory variations in the magnitude of the inflow of blood
from the systemic and pulmonary venous beds
into the atria takes place, it would be anticipated that variations in the magnitude of the
left-to-right shunt would also occur. Suggestive evidence that the left-to-right shunt actuCirculation, Volume XXV, February 1962
341
SPLITTING SECONI) HEART SOUND
Az00030000: A2V82
s P2
LT. 2:
S,i.
t9t
.
C4Sp
' 2
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
: .I.
P2
'
SI
$;M ::P* 00-87-67:
:N
Figure 13
A representative phonocardiogramn -ecordled from a patient with PS. AlIthough there tz
signtificant splittinzg of the second sounid during expiratio, A 2-P2 increases further
during inspiration.
ally diminishes duringr inspiration and becomes augmented duLring expiration xwas
provided by the observation that in patielnts
with ASD the oxygetn saturationi of blood
withdrawn from the pulmonary artery during
expiratioln exceeds the saturation of blood
withdrawn duringc inspiration (table 2). In
conclusion, these considerations woould suggest
that the relative constaiicy of the splitting of
the secoind heart sound ini patienits witlh ASD
is not due to ani inability of the right ventricle
to augment its stroke output during inspiration,24 but it is postulated that the conistancy
of splittincr is due to reciprocal changes in
the magnitude of the left-to-right shunt and
Circulation, Volume XXV, February 1962
the systemic venous inflowv into the right ventriele duLring respiration.
Reg,ardless of the exact meehanism underlying the variations in the splitting of the
seconid heart souncd, precise auseultatory anid
phonocardiographic analyses of the effects of
niormal respiration and of the Valsalva maneuver on this sounid are of areat clinieal
value. In additionl to indicatin-g the time of
closure of the pulmonic alid aortic valves, the
relative intenisities of the two compolnen-ts of
the seconid heart sounld provide some informatioln regardingr the relative levels of pressure
in the pulmonary artery and aorta. The width
of splitting, duriin expiration and the mag-
AYGEN, BRAUNWALD
342
7n
IU
--
60
I
I
I
I
I
II
* Normal
A A.S.
o P.D.A.
-
*
I.
50
INSPIRATORY
INCREASE OF 401
A2-P, INTERVAL D.
(msec)
301
II
A.
0
0
0
~~~~I
AA
1
A
0
* *0
L__
.----'
20 m
AO
A
A
A
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
1l-
I
so
I
I
XI.
a
&£
*
S! i:
MAAI
As
-50
I
IIa
I
-30
-10
-40
-20
Ai P. INTERVAL
A)
I
10
20
I
i
30
40
50
DURING EXPIRATION (msec)
Figure 14
A2-P2 interval during expiration, and the increase of this interval during inspiration
in normal subjects and in patients wtith AS and PDA. WVhen A2 followed P2 the A2-P2
interval was considered to be negative. All values to the left and below the broken line
were outside of the normal range.
nitude of the changes in this time interval
during inspiration can generally be appreciated by careful auscultation, but pholiocardiographic tracings are necessary for precise
measurements. In the vast majority of patients with ASD the inspiratory increase o
A2-P2 is 10 msee. or less. An increase of 10
msec. was found in only two of 51 normal
subjects, and it would seem appropriate to
designate a change of A2-P2 up to 10 msee.
during normal respiration as "fixed splitting" of the second heart sound. It is of interest that the three patients with ASD who
did not demonstrate fixed splitting did not
have the hemodynamic features that are typical for ASD; all three had very small left-toright shunts and one also had severe pulnmonary hypertension.
In normal subjects the Valsalva maneuver
tends to exaggerate the changes in Q-P2, Q-A2.
and A2-P2 observed during quiet respiration
(figs. 4, 6, and 9), but this maneuver does ilot
abolish the "fixed splitting" of the second
sound in patients with ASD (fig. 5). In the
normal subjects the mean increase of A2-P2
during inspiration equaled 37.8 msec.: this
time interval increased to an average of 49.7
msec. followinlg the Valsalva maneuver. In
conitrast, A2-P2 increased by a mean value of
only 3.3 msee. both during inspiration and
following the Valsalva maneuver in patients
with ASD. During auscultation this maneuver
has been found to be helpful in distinguishing
patients with ASD from those subjects who
on clinical examination tend to show little
variation in A2-P2 during normal respiration.
We have encountered five patients without
ASD, includinog two subjects without cardiovascular disease, who demonstrated "fixed
splitting" of the second heart sound during
normal respiration phonocardiographically
and in whom greater changes in A,-P. were
Circulation, Volume XXV, February 1962
SPLITTING SECOND HEART SOUND
343
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
RSS 03-39-46
Figure 15
phonocardiogroim recorded from a potifrt with sevecre A-S. There is
paradoxicual splitting of the seco U]c heart sotmd, wcih issi.iigle during inspirationz but
sRplit: dar iM, etpitrotion. Thle carotid pulse (l()w(owi trajing) shows thait A2 follows' P2.
A representative
observed following the Valsalva manieuver.
Exaggeration of the chainge in splitting of
the second hieairt sounid by this mnaneuver has
also beeni of conlsiderable aid during cardiac
auseultation of patients witlh unlusuiallyv wide
splitting of this sounid during expiration. In
such patients any given change in A%-P2 is
far more difficult to appreciate by auseultation than a simailar chalnge iln patients Awitl
shorter A2-P2 initervals.
In the iilmmediate postoperative period following repair of an ASD somne patients show
little, if any, change of A2-P2 during, nornail]
resliration. These patienlts also showed a norinal increase of A2-P2 followingr the Valsalva
maneuver. When studied 3 to 12 mnonths following operation the seconid heart sound
tended to exhibit a normal patternii during
quiet respiration in those latients in whioi
the defects Awere closed. In two patients wvithi
residual slhun-ts, however, distinctly ahbnormal
splittingy persisted. Thlus, phonocardiocraphic
study in the posto)erative period is a useful
technici itl the elinical iassessm-iient of patienits
with ASD (fig. 10).
In the patients with moderate or severe PS
and an initact ventricular septum, A2-P2 durCirculation, Volume XXV, February 1962
iLglr expiratioil tended to be prologlmd al(li iti
the samne racrne as observed in patients with
ASD. The patients with PS showed a greater
increase in this initerval during inspiration,
however, than did those with ASD. In both
patients with PS and fixed splitting of the
seconid heart sound, illustrated in figure 12 a
nornmal increase of A2-P2 occurred following,
the Valsalva maneuver. These results are in
agrreement with those of Leathamn and Weitzman26 and of other inivestigators.27 9 As in
patients with ASD with a small shuint, muildl
degrees of PS generally result in nornial
splitting of the second heart souiid. The increased resistance to riglht ventricular ejeetioni in these patients is apparently the cause
of the prolongation of Q-P2 and the abnrormnally wide splittinig of the second heart
sournd. When a VSD is associated wit]l obstructioi-i to right ventricular outflow, tliere
is only a tendency to abnormnal prolongationi
of A2-P1 durinicg expiration in those patienits
with a large left-to-right shunit. When the obstruetion to right ventricular ejection is severe anid there is a large right-to-left slhunt
(tetralogy of Fallot) tlhe pulmonarv elosuire
sotund eaninot usually be recorded.
344
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
In patients with obstruction to left ventricular outflow, there is a tendency to prolongation of left ventricular ejection,30 and this is
reflected either in reversal of the normal sequence of semilunar valve closure or simultaneous valve closure during expiration (figs.
14 and 15). In those patients in whom the
sequence is reversed, prolongation of Q-P2
and abbreviation of Q-A2 occur during inspiration, resulting in narrowing of the P2-A2
interval. This abnormality has been termed
"paradoxical" splitting of the second heart
sound, and it is also evident in some patients
with patent ductus arteriosus (fig. 14) in
whom the prolongation of left ventricular
ejection is presumably related to the increased
stroke volume of the left ventricle.
Summary
The characteristics of the second heart
sound were analyzed in 350 phonocardiograms
recorded from patients in all of whom the
diagnosis was proved either at operation or by
detailed catheterization studies. A2-P2 during
expiration averaged 10.6 msec. in normal subjects. Q-A2 changed little during inspiration,
with an average decrease of only 5.2 msee.,
while Q-P2 increased by an average of 32.6
msec. The average increase of A.-Po during
inspiration was therefore 37.8 msec. In patients with ASD, A2-P2 during expiration
averaaed 50.2 msee. and the inspiratory
change in Q-P2 averaged only 4.6 msec. In
115 of 118 patients with ASD the inspiratory
inerease of A2-P2 ranged from 0 to 10 msee.
Following successful surgical closure 29 patients with ASD developed the normal inspiratory augmentation of A2-P2; in the two
patients in whom the defect was not completely closed the relatively constant A2-P2
noted preoperatively persisted.
Release of the Valsalva maneuver exaggerated the inspiratory increase of A2-P2 observed in normal subjects but did not modifv
this interval in patients with ASD. Analysis
of the effect of release of the Valsalva maneuver on A2-P2 was helpful in separating patients with ASD from normal subjects.
Evidence was presented that the relative constancy of the splitting of the second heart
AYGEN, BRAUNWALD
sound in patients with ASD is due to reciprocal changes in the magnitude of the left-toright shunt and the systemic venous inflow
into the rigrht ventricle during respiration.
In patients with moderate or severe pulmonary stenosis, A2-P2 during expiration was
longer than in normal subjects and in the
same range as in patients with ASD. However, patients with PS showed a normal augmentation of A2-P2 during expiration. In patients with congenital AS, and those with
PDA, left ventricular ejection tended to be
prolonged with reversal of the normal sequence of semilunar valve closure or simultaneous closure of these valves during expiration.
Acknowledgment
The cooperation of Dr. Andrew G. Morrow and
of the staff of the Clinic of Surgery, National Heart
Institute, is gratefully acknowledged.
References
1. ROUANET, J.: Analyse des bruits du coeur. Paris
thesis, No. 252, 1832.
2. POTAIN, M.: Note sur les dedublements normaux
des bruits du coeur. Bull. et m6m. Soc. med.
hop. Paris 3: 138, 1866.
3. LEATHAM, A., AND TOWERS, M.: Splitting of the
second heart sound in health. Brit. Heart J.
13: 575, 1951.
4. LEATHAM, A.: Splitting of the first and second
heart sounds. Lancet 2: 607, 1954.
5. KATZ, L. N.: The asynchronism of right and left
ventricular contractions and the independent
variations in their duration. Am. J. Physiol.
72: 655, 1925.
6. BRAUNWALD, E., FISHMAN, A. P., AND COURNAND,
A.: Time relationship of dynamic events in
the cardiac chambers, pulmonary artery and
aorta in man. Circulation Research 4: 100,
1956.
7. MCKUSICK., V. A., REAGAN, W. P., SANTAS, G. W.,
AND WEBB, G. N.: The splitting of heart
sounds. Am. J. Med. 19: 849, 1955.
8. LEATHAM., A., AND GRAY, I.: Auscultatory and
phonocardiographic signs of atrial septal defect. Brit. Heart J. 18: 193, 1956.
9. WOOD, P.: Discussion of splitting of P2 in ASD.
Brit. Heart J. 20: 267, 1958.
10. McKusicK, V. A.: Cardiovascular Sound in
Health and Disease. Baltimore, The Williams
and Wilkins Company, 1958.
11. SANDERS, R. J., AND MORROW, A. G.: The diag-
nosis of circulatory shunts by the nitrous
oxide test. Circulation 18: 856, 1958.
Circulation, Volume XXV, February 1962
SPLITTING SECOND HEART SOUND
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
12. SANDERS, R. J., AND MORROW, A. G.: The identification and quantification of left-to-right circulatory shunts. A new diagnostic method
utilizing the inhalation of a radioactive gas,
Krm. Am. J. Med. 26: 508, 1959.
13. MORROW, A. G., BRAUNWALD, E., AND ROSS, J.,
JR.: Left heart catheterization: An appraisal
of techniques and their applications in cardiovascular diagnosis. Arch. Tnt. Med. 105: 645,
1960.
14. SANDERS, R. J., CoopyR, T., AND MoRRow, A. G.:
An evaluation of the nitrous oxide method for
the quantification of left-to-right shunts. Circulation 19: 898, 1959.
15. BRAUNWALD, E., SARNOFF, S. J., AND STAINSBY,
W. N.: Determinant of duration and mean
rate of ventricular ejection. Circulation
Research 6: 319, 1958.
16. BRECHER, G. A., AND HUBAY, C. A.: Pulmonary
blood flow and venous return during spontaneous respiration. Circulation Research 3: 210,
1955.
17. LAUSON, H. D., BLOOMFIELD, R. A., AND
COURNAND, A.: The influence of the respiration on the circulation in man. Am. J. Med.
1: 315, 1946.
18. BOYD, T. E., AND PATRAS, If. C.: Variations in
filling and output of the ventricles with the
phases of respiration. Am. J. Physiol. 134:
7, 1941.
19. SHULER, R. H., ENSOR, C., GUNNING, R. E., Moss,
W. G., AND JOHNSON, V.: The differential
effects of respiration on the left and right
ventricles. Am. J. Physiol. 137: 620, 1942.
345
20. BOYER, S. H., AND CHISHOLM, A. W.: Physiologic
splitting of the second heart sound. Circulation 18: 1010, 1958.
21. SHAFTER, H. A.: Splitting of the second heart
sound. Am. J. Cardiol. 6: 1013, 1960.
22. BARBER, J. M., MAGIDSON, O., AND WOOD, P.:
Atrial septal defect. Brit. Heart J. 12: 277,
1950.
23. BRAUNWALD, E., DoNoso, E., SAPIN, S. O., AND
GRISHMAN, A.: Riglht bundIle branch block.
Hemodynamic, vectorcardiographic and electrocardiographic observations. Circulation 13:
866, 1950.
24. PERLOFF, J. K., HARVEY, W. P.: Mechanisms of
fixed splitting of the second heart sound.
Circulation 18: 998, 1958.
25. DEXTER, L.: Atrial septal defect. Brit. Heart J.
18: 209, 1956.
26. LEATHAMT, A., AND WEITZMAN, D.: Auscultatory and phonocardiographic signs of piulmonary stenosis. Brit. Heart J. 19: 303, 1956.
27. ABRAHAMS, D. G., AND WOOD, P.: Pulmonary
stenosis with normal aortic root. Brit. Heart
J. 13: 519, 1951.
28. CREVASSE, L., AND LOGUE, R. B.: Valvular pulmonic stenosis: Auscultatory and phonocardiographic characteristics. Am. Heart J. 56: 898,
1958.
29. VOGELPOEL, L., AND SCHRIRE, F.: Auscultatory
and phonocardiographic assessment of pulmonary stenosis with intact ventricular septum.
Circulation 22: 55, 1960.
30. GRAY, I. R.: Paradoxical splitting of the second
heart sound. Brit. Heart J. 18: 21, 1956.
The Early History of Instrumental Precision in Medicine
The true rate of advance in medicine is, however, not to be tested by the work of
single men, but by the practical capacity of the mass. The truer test of national medical progress is what the country doctor is. How useful, how simple, it seemed to count
the pulse and respiration, or to put a thermometer under the tongue, and yet it took
in the one case a cantury, and in another far more, before the mass of the profession
learned to profit by the wisdom of the few.-S. WEIR MITCHELL, MD., Transactions of
the Congress of American Physicians and Surgeons held at Washington, D.C., 1891.
New Haven, The Congress, 1892, p. 180.
Cfrcuiation. Volume XXV. February
196*
The Splitting of the Second Heart Sound in Normal Subjects and in Patients with
Congenital Heart Disease
MAURICE M. AYGEN and EUGENE BRAUNWALD
Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017
Circulation. 1962;25:328-345
doi: 10.1161/01.CIR.25.2.328
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1962 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://circ.ahajournals.org/content/25/2/328
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles
originally published in Circulation can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of
the Web page under Services. Further information about this process is available in the Permissions
and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/