Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
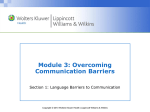
The Cardiovascular System: CORONARY ARTERY DISEASE (CAD) AND CARDIAC ARRHYTHMIAS Physiology • The heart requires oxygen to be delivered to its own cells. • Coronary arteries deliver this oxygenated blood to the heart. • Oxygen requirements of the heart increase as the heart pumps faster and works harder. • Oxygen demands of the heart also increase if the heart has to overcome peripheral resistance in the vessels (high afterload). Cardiac Glycosides The cardiac glycosides also are known as digitalis preparations Digoxin is used to maintain clinical stability and improve symptoms, quality of life, and exercise tolerance in patients with all phases of heart disease. Digoxin does not decrease mortality. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins The Foxglove Plant (Digitalis purpurea) Cardiac Glycosides (cont.) • Digoxin increases the force of cardiac contraction, increasing cardiac output and slowing heart rate. • Digoxin is used for patients with chronic heart disease and heart failure. Prototype drug: digoxin (Lanoxin) Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Digoxin: Core Drug Knowledge • Pharmacotherapeutics – Used in the treatment of CHF and atrial fibrillation • Pharmacodynamics – Exerts an indirect effect on the heart from stimulation of the autonomic nervous system (cholinergic agonist). • Side effects – Anorexia, N/V, diarrhea, headache, weakness, apathy, drowsiness, visual disturbances • Adverse effects – Dysrhythmias,, confusion, restlessness, disorientation, seizures, delirium, hallucinations, neuralgia, and psychosis Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Digoxin: Core Drug Knowledge (cont.) • Minimizing adverse effects – Digoxin has a narrow therapeutic index. It is important to monitor the serum levels of digoxin. – Check pulse rate and hold dose if <60 • Patient and family education – Explain the reason for taking digoxin and the adverse effects of the drug. Teach patient how to monitor pulse at home. – Discuss that many OTC drugs can interact with digoxin. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Pathophysiology: Ischemia • When the oxygen requirements of the heart are greater than the supply of oxygen it is getting, the heart muscle becomes ischemic. • Oxygen imbalance may be from: – reduced coronary blood flow – need for increased oxygen • Chest pain that results from ischemia is termed angina. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Pathophysiology: Coronary Artery Disease Major Risk Factors for CAD • Cigarette smoking • Diabetes • Elevated blood lipid levels • Hypertension. There are four types of angina: – Stable angina – Unstable angina – Variant angina – Microvascular angina Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Antianginal Agents • • • • Nitrates Beta adrenergic antagonists (Beta Blockers) Calcium Channel Blockers Other Drugs Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Nitrates • Nitrates dilate vascular smooth muscle in both venous and arterial vessels. • Venous dilation decreases the returning flow of blood to the heart (preload). • Arterial dilation reduces systemic vascular resistance and arterial pressure (afterload). These effects decrease the total workload on the heart and its oxygen needs – both preload and afterload. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Beta Blockers • Beta blockers prevent the beta-adrenergic (sympathetic nervous system) receptors from being stimulated. • These drugs have multiple effects on the heart and cardiovascular system. • These effects decrease the oxygen demands of the heart and thereby decrease angina. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Calcium Channel Blockers • Calcium is needed in the conducting cells of the heart to help create an electric action potential. • Calcium-channel blockers inhibit calcium from moving across cell membranes. • The effects are a decrease in contraction, depression of impulse formation (automaticity), and slowing of conduction. • These have the effect of decreasing the oxygen needs of the heart. • Calcium channel blockers also cause arteriolar dilation, decreasing afterload. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Adjunctive (Additional) Drug Therapies • Oher drugs are used as adjuncts to the main drug therapies for treating angina. • They are used to: – Slow down the progression of coronary artery disease, – Prevent complications that may arise with angina, or – Minimize symptoms. • Thrombus formation is an important concern with unstable angina, and some of these therapies specifically target this problem. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Adjunct Drug Therapies (cont.) • Lipid-lowering agents often are often used in conjunction to slow the progression of coronary heart disease. • An ACE inhibitor can be used in patients with coronary artery disease if they also have diabetes, systolic dysfunction, or both. • If the pain of unstable acute angina is not controlled by nitrates, morphine can be used to treat the pain. • Oxygen, although not a drug, is commonly used to provide an additional 02 supply to cardiac muscle tissue. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Question Nitrates dilate the vascular smooth muscle resulting in what effect? A. Increased systemic vascular resistance B. Decreased preload & afterload C. Increased afterload D. Increased ejection fraction Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Question Nitrates dilate the vascular smooth muscle resulting in what effect? B. Decreased preload & afterload Answer: Nitrates dilate vascular smooth muscle. Venous dilation decreases the returning flow of blood to the heart (preload) & arterial dilation decreases peripheral resistance (afterload) Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Nitrates Nitrates improve the circulation to the heart by redistributing blood flow to the collateral vessels and dilating both veins and arteries. Prototype drug: nitroglycerin (Nitrostat, Nitrodur) Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Nitroglycerin: Core Drug Knowledge • Pharmacokinetics – Administered: IV, topical, oral, sublingual, nasal. Pharmacokinetics vary with route of administration • Pharmacodynamics – Relaxes vascular smooth muscle and dilates both arterial and venous vessels Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Nitroglycerin: Core Drug Knowledge • Side effects – Headache, hypotension, postural hypotension, tachycardia, vertigo, anxiety, and weakness • Adverse effects – Syncope (fainting) • Minimizing adverse effects – Assess pulse and blood pressure before administering – Monitor for orthostatic hypotension and assist the patient to a standing position gradually when arising. – Treat any headache that develops with aspirin or acetaminophen. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Nitroglycerin: Teaching, Assessment, and Evaluations • Patient and family education – Explain the purpose and adverse effects of nitroglycerin. – Instruct patients to sit or lie down when experiencing angina. – Explain that postural hypotension may occur. – Keep PRN tablets in a dark and relatively cool place. Advise patient to not keep PRN tablets in a warm place, e.g. a pants pocket Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Question Which statement by the patient would indicate the need for additional teaching about proper administration of nitroglycerin? A. I will keep the sublingual tablets out of the sun or heat. C. I will apply the transdermal patch on my lower arm to prevent a headache. D. If the chest pain is not relieved after three sublingual nitroglycerin’s I will call EMS. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Question Which statement by the patient would indicate the need for additional teaching about proper administration of nitroglycerin? C. I will apply the transdermal patch on my lower arm to prevent a headache. Rationale: Transdermal nitro should be applied to an area of the body that does not have excessive hair, to promote absorption. Apply to the chest, upper arm, or upper thigh to promote absorption and increase onset of systemic action. Do not apply to distal parts of extremities. Headaches are a common side effect possible because of the vasodilation effects and are not related to administration route. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Cardiac Rhythm: Physiology • Contractions of the heart depend on the electrical conduction system of the cardiac muscle. • The conduction system connects to highly specialized cardiac cells that allow the heart to beat predictably and rhythmically. • The electrical system is composed of the: – Sinoatrial (SA) node – Atrioventricular (AV) node – Bundle of HIS – Bundle branches – Purkinje fibers Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Travel of Electrical Current Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Physiology (cont.) • The SA node, influenced by both the sympathetic and the parasympathetic nervous systems, is known as the pacemaker of the heart. • It is important to understand how potassium, sodium, and calcium ions bring about electrical changes in the cardiac cells that stimulate contraction of the cardiac cells. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Movement of Electrolytes – Cause of Depolarization of Cells Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Electrolytes • Alterations in potassium (K), sodium (Na) or calcium (Ca) levels - either too high or too low - will result in cardiac electrical abnormalities called cardiac arrthymias. • Some of these arrthymias are life-threatening and all can interfere with normal cardiac output. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Damage to the Myocardium • Any damage to the myocardium (muscles of the heart) causes scar tissue to form. • Scar tissue cannot transmit electrical activity, therefore the electrical impulses have to take a circuitous route. • This can be detected on an Electrocardiogram (ECG, EKG) tracing. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Electrocardiogram SA Node Fires > Depolarization Impulse travels to Atrium then Ventricles causing contraction Muscle cells return to a resting state > Repolarization Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Electrocardiogram Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Question It is possible to have electrical activity reflected on an EKG tracing but not to have a beating heart. 1. True 2. False Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Question It is possible to have electrical activity reflected on an EKG tracing but not to have a beating heart. This is True! Electrical activity is an indirect measure of cardiac health. The SA node will continue to fire for a while even if the heart muscle is too damaged to respond. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Pathophysiology • Arrhythmias, also called dysrhythmias, are a disturbance in the electrical activity of the heart. • Some are insignificant and do not create any problems for the patient. • Others disrupt the function of the heart, increase the oxygen demand of the heart, and/or interfere with cardiac output. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Examples of Arrhythmias Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Examples of Arrhythmias Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Examples of Arrhythmias Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Examples of Arrhythmias Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Drugs and Other Therapies to Treat Arrhythmias • Drug therapy previously was the mainstay for treating arrhythmias; now Implanted Cardiac Defibrillators (ICDs) are equally important in preventing sudden cardiac death. • Arrhythmias can also be treated by ablation (cauterizing). Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Class I Antiarrhythmic Drugs Prototype drug: Lidocaine (Xylocaine) • Pharmacotherapeutics – Treat all acute ventricular arrhythmias. • Pharmacokinetics – Administered: IV. Metabolism: liver. Excreted: kidneys. T1/2: 1.5 to 2 hours • Pharmacodynamics – Decreases automaticity, excitability and membrane responsiveness. Decreases action potential duration and effective refractory period of Purkinje fibers and ventricular muscle Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Lidocaine: Core Drug Knowledge (cont.) • Side effects – Hypotension, dizziness, lightheadedness, fatigue, drowsiness • Adverse effects – Cardiac arrhythmias • Drug interactions – Many classes of drugs • Environment – Should be given in hospital or emergency setting with continuous ECG monitoring Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Class II Antiarrhythmic Drugs • Antiarrhythmic class II drugs (beta blockers) depress depolarization. • Beta blockers slow heart rate by suppressing the SA node, slow the speed of conduction through the AV node, and decrease the force of contraction. • They effectively reduce mortality in patients who have had a recent MI, those with symptomatic heart failure, and those with congenital long QT syndrome. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Class III Antiarrhythmic Drugs • Class III antiarrhythmics produce a prolongation of repolarization. • Action potential duration and refractory periods are prolonged, leading to reduction in membrane excitability of all myocardial tissue. Prototype drug: amiodarone (Cordarone) Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Amiodarone: Core Drug Knowledge • Pharmacotherapeutics – Approved for use only in life-threatening arrhythmias • Pharmacodynamics – Prolongation of the refractory period, and noncompetitive alpha- and beta-adrenergic inhibition • Significant Drug interactions – Digoxin and warfarin Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Amiodarone: Core Drug Knowledge (cont.) • Adverse effects – Pulmonary toxicity, exacerbation of the arrhythmia, and liver disease – Occasionally causes an ocular symptom of colored rings around lights and gradually decreased vision. – Occasionally causes a cutaneous photosensitivity reaction that may be associated with a peculiar bluegray discoloration of the skin • Minimizing adverse effects – Correct electrolyte disturbances before beginning therapy. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Pulmonary Toxicity w/ Amiodarone • Amiodarone is an iodine-containing compound that tends to accumulate in several organs including lungs. • It can occasionally cause either hypo or hyperthyroidism • It has high lipid solubility & tends to accumulate extensively in adipose (fat) tissue and highly perfused organs such as the liver, lungs and spleen • It can produce lung damage directly by a cytotoxic effect and indirectly by an immunological reaction (2%-15%) • Most patients respond well to the withdrawal of the drug and the administration of corticosteroids, which are usually given for four to 12 months. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Amiodarone: Teaching, Assessment, and Evaluations • Patient and family education – Explain the purpose of the drug and possible adverse effects of the drug. – Emphasize the importance of returning for follow-up blood work and ECGs. – Teach patients to use appropriate protection when out in the sun and to limit sun exposure. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Class IV Antiarrhythmic Drugs • Class IV antiarrhythmics depress depolarization and lengthen phases 1 and 2 of repolarization. Prototype drug: verapamil (Calan) • Pharmacotherapeutics – Antiarrhythmic for chronic atrial flutter or fibrillation • Pharmacodynamics – Inhibits the movement of calcium ions across the cardiac and arterial muscle cell membrane • Side effects – Constipation, dizziness, headache, nausea, hypotension • Adverse effects – Peripheral edema Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Verapamil: Teaching, Assessment, and Evaluations • Patient and family education – Stress the importance of adequate fluid intake and dietary fruit and fiber to help prevent constipation. • Ongoing assessment and evaluation – It is important to monitor liver function periodically to detect elevated serum drug levels. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Physiology: Lipid Management • Serum lipids are fats found in the bloodstream. • These lipids include cholesterol, phospholipids, and triglycerides. • They are transported in the blood as part of large molecules called lipoproteins. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Physiology (cont.) • Cholesterol is a soft, waxy substance found among the lipids in the bloodstream and in all of the body’s cells. • The body, mostly in the liver, produces essentially all of the cholesterol needed for normal functioning— about 1,000 mg a day. • Cholesterol plays a role in forming cell membranes, some hormones, and other needed tissues. • Low Density Lipoprotein (LDL) is the major cholesterol carrier in the blood. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Pathophysiology • Hyperlipidemia is an elevation of blood lipid levels. • Hyperlipidemia is considered a risk factor for the following disorders: – Atherosclerosis – Coronary artery disease – Thrombosis (clotting) • When the amount of cholesterol within cells builds up, the number of these receptors on cell surfaces is reduced, preventing all of the lipids from entering the cells. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Pathophysiology (cont.) • Patients with narrowed arteries from atherosclerotic cardiovascular disease are more likely to have hypertension. • Ideal cholesterol levels: – Total cholesterol: less than 200 mg/dL – Low-density Lipoproteins = LDL: <100 mg/dL – High-density Lipoproteins = HDL: >40 to 59 mg/dL Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Lifestyle and Reduction of Low-Density Lipoprotein Levels Therapeutic Lifestyle Changes. • Lifestyle changes include: – Diet – Weight loss – Increased physical activity Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Antihyperlipidemics • Anti-hyperlipidemics are a group of medications that reduce cholesterol, reduce triglycerides or both. • Some non-prescription agents are now included in this grouping: – Fish oil (Omega 6 Fatty Acid) at 3000 mg/day has been shown to reduce triglyceride levels • Prescription formulation: Lovaza – Nicotinic acid (Niacin, Vitamin B3) • Prescription formulation: Niaspan Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Statins • Statins lower blood cholesterol levels. • Statin therapy can: – Lower LDL cholesterol by 20% to 55% – Raise HDL levels between 5% and 15% – Lower triglycerides between 7% and 33%. • Evidence suggests that statins work in other ways beside lowering cholesterol levels to decrease the occurrence of cardiovascular events, e.g. reducing inflammation. Prototype drug: atorvastatin (Lipitor) Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Atorvastatin: Core Drug Knowledge • Pharmacotherapeutics – Used for primary hypercholesterolemia and combined hyperlipidemia • Pharmacokinetics – High first-pass effect. Highly protein bound. Excreted primarily through the GI tract • Pharmacodynamics – Competitively inhibits an enzyme important in cholesterol biosynthesis (making cholesterol). Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Atorvastatin: Core Drug Knowledge • Contraindications and precautions – Active liver disease and pregnancy • Side effects – Muscle and joint aches, weakness, muscle cramps • Adverse effects – Muscle damage, liver damage, and rhabdomyolysis* *Potentially lethal muscle destruction • Drug interactions – Anti-fungal drugs, erythromycin, and grapefruit juice Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Atorvastatin: Planning and Interventions • Maximizing therapeutic effects – Most effective when administered in the evening – Immediate-release administered after evening meal – Extended-release administered at bedtime • Minimizing adverse effects – Liver function test (AST and ALT) results should be monitored before starting therapy. – Evaluate the patient carefully for muscle soreness, tenderness, or pain and CK levels. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Statins: Teaching, Assessment, and Evaluations • Patient and family education – Stress the importance of following a low-cholesterol and low-saturated-fat diet. – Instruct patients to report any unexplained muscle pain, tenderness, or weakness. – Photosensitivity may occur. • Ongoing assessment and evaluation – The patient should have liver function tests and CK measurement performed periodically throughout drug therapy. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Drugs Closely Related to Atorvastatin - Lovastatin (Mevacor) - Fluvastatin (Lescol) - Pravastatin (Pravachol) - Rosuvastatin (Crestor) - Simvastatin (Zocor) ____________________________________________ • All work similarly to lower LDL cholesterol and have similar adverse effects. • Pravastatin differs from the prototype lovastatin because it is not metabolized via the P-450 system and thus does not produce the drug interactions of lovastatin (best with liver disease) Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Drugs Significantly Different from the Statins: Fibric Acid Derivatives • These drugs lower triglyceride levels and increase HDL cholesterol. • These drugs can reduce triglyceride levels between 35% and 53%. • Effects on LDL cholesterol may be either to lower it between 6% and 20% or to raise it slightly. • Although in certain patients these drugs may be used alone, most frequently they are used in combination with statins. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Fibric Acid Derivatives (cont.) • The combined used of a fibrate and a moderatedose statin carries a somewhat increased risk of myopathy. • Contraindications include hepatic or severe renal dysfunction, including primary biliary cirrhosis, preexisting gallbladder disease, or hypersensitivity. • Serious adverse effects include abnormal liver function tests, rhabdomyolysis, and hyperglycemia. Prototype: fenofibrate (Tricor) Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Cholesterol Absorption Inhibitors • These drugs act in the small intestine, where they inhibit the absorption of cholesterol. • It is given orally once daily either as monotherapy or in combination therapy with a statin. • This drug decreases LDL about 17% but has no effect on HDL or triglycerides. Prototype: Ezetimibe (Zetia) Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Ezetimibe: Core Drug Knowledge • Pharmacotherapeutics – Used to reduce cholesterol, particularly LDL – Used in combination with statins • Pharmacokinetics – 90% protein bound, increased absorption with a high-fat meal, once daily oral dosing • Pharmacodynamics - Decreases cholesterol absorption in the small intestine Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Ezetimibe: Core Drug Knowledge • Contraindications – Severe liver disease • Side effects – Headache, Diarrhea • Adverse effects – Elevated liver enzymes, myopathy, angioedema • Drug Interactions – Minimal Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Nicotinic Acid (Niacin, Vitamin B3) • Nicotinic acid (niacin or vitamin B3) is used to treat hyperlipidemia. • Nicotinic acid reduces levels of triglycerides and LDL cholesterol levels and raises levels of HDL cholesterol. • Triglycerides and VLDL levels are reduced by 25% to 30% in 1 to 4 days. • LDL level reductions may be seen in 5 to 7 days, with the maximal effect seen in 3 to 5 weeks. Prototype: nicotinic acid (Niaspan) Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Adverse Reaction to Nicotinic Acid Although all B Vitamins are water soluble and safe in people with normal renal function, some people experience flushing (vasodilation), and a tingling, itching or the sensation of being pricked by cactus needles (paresthesia) and cannot tolerate this product. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Homework • Review your ATI Modules • Do Quiz #7: The Cardiovascular System (10 points) • Do Shadow Health DCE: Patient John Larsen (10 points) – This activity will take approximately one-hour to complete. – You will be asked to administer medications to Mr. Larsen including anti-hypertensive drugs. – Don’t forget to communicate with the patient and do patient education! – Do the questions at the end for my review. Copyright © 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins