Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Clostridium difficile infection wikipedia , lookup
Sarcocystis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Cryptosporidiosis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Diagnosis of HIV/AIDS wikipedia , lookup
Trichinosis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Leptospirosis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Neonatal infection wikipedia , lookup
Onchocerciasis wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
History of tuberculosis wikipedia , lookup
Mycobacterium tuberculosis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Hepatitis B wikipedia , lookup
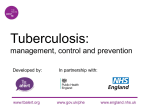
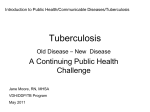
® infectious diseases Board Review Manual Statement of Editorial Purpose The Hospital Physician Infectious Diseases Board Review Manual is a study guide for fellows and practicing physicians preparing for board examinations in infectious diseases. Each man ual reviews a topic essential to current prac tice in the subspecialty of infectious diseases. PUBLISHING STAFF PRESIDENT, Group PUBLISHER Bruce M. White editorial director Debra Dreger SENIOR EDITOR Bobbie Lewis associate EDITOR Diagnosis and Treatment of Latent Tuberculosis Infection Contributors: Edward D. Chan, MD Department of Medicine National Jewish Medical and Research Center Denver, CO Kathryn Chmura, BA Department of Medicine National Jewish Medical and Research Center Denver, CO Tricia Faggioli EDITORial assistant Farrawh Charles executive vice president Barbara T. White executive director of operations Jean M. Gaul PRODUCTION Director Suzanne S. Banish PRODUCTION associate Kathryn K. Johnson ADVERTISING/PROJECT director Patricia Payne Castle sales & marketing manager Deborah D. Chavis NOTE FROM THE PUBLISHER: This publication has been developed with out involvement of or review by the Amer ican Board of Internal Medicine. Endorsed by the Association for Hospital Medical Education Table of Contents Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Case Study. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Summary. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Cover Illustration by May Cheney Copyright 2007, Turner White Communications, Inc., Strafford Avenue, Suite 220, Wayne, PA 19087-3391, www.turner-white.com. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, electronic, photocopying, recording, or otherwise, without the prior written permission of Turner White Communications. The preparation and distribution of this publication are supported by sponsorship subject to written agreements that stipulate and ensure the editorial independence of Turner White Communications. Turner White Communications retains full control over the design and production of all published materials, including selection of appropriate topics and preparation of editorial content. The authors are solely responsible for substantive content. Statements expressed reflect the views of the authors and not necessarily the opinions or policies of Turner White Communications. Turner White Communications accepts no responsibility for statements made by authors and will not be liable for any errors of omission or inaccuracies. Information contained within this publication should not be used as a substitute for clinical judgment. www.turner-white.com Infectious Diseases Volume 10, Part 2 Infectious Diseases Board Review Manual Diagnosis and Treatment of Latent Tuberculosis Infection Edward D. Chan, MD, and Kathryn Chmura, BA “[I]n the treatment of Consumption, . . . in the commencement [it] is easy to cure and difficult to understand; but when it has neither been discovered in due time nor treated upon a proper principle, it becomes easy to understand and difficult to cure.” –Niccolo Machiavelli (1469–1527) Introduction The World Health Organization estimates that one third of the world’s population is latently infected with Mycobacterium tuberculosis.1 From this pool, approximately 9 million active tuberculosis (TB) cases emerge annually, resulting in 2 to 3 million deaths and making TB the second most common cause of death by a single infectious agent in the world.2 The AIDS epidemic is responsible for the rise in TB cases in many parts of the world (in approximately 1.5 million active TB cases per year there is co-infection with HIV), and co-infection with both agents contributes significantly to TB-related mortality. Ninety-five percent of cases of TB occur in the developing world. Annual incidence rates exceed 300 cases per 100,000 persons in much of sub-Saharan Africa, the Indonesian and Philippine archipelagos, Afghanistan, Bolivia, and Peru.1,3 Areas with the highest incidence include the most populous nations of India (1.9 million cases/yr) and China (1.4 million cases/yr). In North America, cases occur disproportionately among foreign-born individuals from TB-endemic countries, HIV-infected persons, institutionalized persons, and minorities. The United States saw a decline in TB cases up to the early 1980s due mostly to public health programs, but HIV/AIDS, immigration, and waning TB programs led to a resurgence of TB in the late 1980s and early 1990s.4 The annual incidence is now declining again, but as TB becomes less frequent in this country, decreased awareness of disease manifestations may lead to delays in diagnosis and treatment. As indicated by the opening quotation, hundreds of years before the cause of TB was elucidated it was recognized that TB may exist in 2 different forms: infection and disease. Infection occurs by airborne transmission Hospital Physician Board Review Manual of tubercle bacilli from person to person. Primary infection is usually asymptomatic but may present with mild nonspecific symptoms, symptoms of acute pneumonia, or severe disseminated disease. After primary infection, M. tuberculosis spreads from the lungs to hilar lymph nodes and then throughout the bloodstream, generally resulting in latent TB infection (LTBI) (Figure 1). Most cases of active TB are due to reactivation of latent infection. Reactivation TB is typically a chronic destructive pneumonia with cavitation and fibrosis involving the lung apices and superior segments of lower lobes. This paper focuses on the diagnosis and treatment of LTBI as opposed to management of active disease. Treatment of active TB is discussed in a recent publication and the latest (2003) guidelines from the American Thoracic Society (ATS)/Centers for Disease Control and Prevention/Infectious Diseases Society of America.5,6 CASE STUDY INITIAL PRESENTATION A 50-year-old woman who works as a nursing assistant at a nursing home receives a tuberculin skin test using 5 units of purified protein derivative (PPD) as part of an annual screening program. After 72 hours, the diameter of the induration is 14 mm, whereas it was 3 mm the previous year. She is asymptomatic, healthy, and does not use tobacco or alcohol. She is not on any medications and is HIV-negative. • What are the exogenous risk factors for TB infection? • What are the endogenous risk factors for reactivation TB? RISK FACTORS Close contact with a person who has pulmonary TB represents the single most important risk factor for TB transmission. Factors associated with a high burden of tubercle bacilli further increase this risk and include www.turner-white.com D i a g n o s i s a n d Tr e a t m e n t o f L a t e n t Tu b e r c u l o s i s I n f e c t i o n Alveolus Tubercle bacilli are ingested by alveolar macrophages and proliferate in them Intracellular bacilli spread to hilar nodes Occult dissemination resulting in latent infection Active TB Figure 1. Graphic representation of a primary tuberculosis (TB) infection and occult dissemination. After ingestion of Mycobacterium tuberculosis by mononuclear phagocytes in the alveoli, a largely asymptomatic dissemination of the tubercle bacilli occurs when infected cells migrate throughout the body, particularly to the lung apices, kidneys, bone growth plates, and the vertebrae, resulting in latent infection. In normal hosts, the risk of progression to active TB in a newly infected individual is ~ 5% for the first year and ~ 5% for the remaining lifetime. exposure to individuals with cavitary pulmonary TB, laryngeal TB, and untreated or inadequately treated TB. Surroundings that facilitate TB transmission include places with indoor crowding such as nursing homes, schools, and prisons. In otherwise healthy individuals, the lifetime risk for progression from LTBI to active TB is approximately 5% within the first year of infection and 5% for the remainder of the lifetime of the individual. However, certain individuals are at significantly increased risk for reactivation TB. Perhaps the single most important host risk factor for reactivation TB is co-infection with HIV, where the estimated rate of reactivation is approximately 5% to 10% per year.7 Nursing home residents also are at increased risk for reactivation due to waning immunity from aging, malnutrition, comorbid illnesses, and/or use of immunosuppressive medications.8 Other particularly high-risk individuals include those with upper lobe fibronodular scarring, suggesting evidence www.turner-white.com of prior untreated TB, recent immigrants from regions endemic for TB, and subjects with silicosis, chronic kidney disease, gastrectomy, malnutrition, diabetes mellitus, organ transplantation, certain malignancies, and immunosuppressive drug use, in particular, prednisone (≥ 15 mg/day for ≥ 1 month) and tumor necrosis factor-a (TNF-a) antagonists.7 • Who are candidates for tuberculin skin testing? CRITERIA FOR SCREENING Testing should be performed on groups with a high risk for TB infection. The most important individuals to test are close contacts of an active case of TB, especially if the exposure occurred prior to treatment of the index case. Others include HIV-infected persons, recent immigrants from countries with high rates of TB infection, homeless persons, health care workers, residents or employees of long-term care facilities, as well Infectious Diseases Volume 10, Part 2 D i a g n o s i s a n d Tr e a t m e n t o f L a t e n t Tu b e r c u l o s i s I n f e c t i o n Table. Criteria for Selecting Individuals for Isoniazid Preventive Therapy Based on Diameter of Tuberculin Reaction Criteria for Positivity Patient Groups ≥ 5 mm Recent close contacts to an active case of TB HIV-positive persons Persons with apical fibronodular disease consistent with prior healed TB Organ transplant recipients ≥ 15 mg/day of prednisone use for ≥ 1 month TNF-α antagonists ≥ 10 mm Recent skin test converters (≥ 10 mm increase within 2 yr) Foreign-born persons in U.S. < 5 yr from highprevalence regions such as Asia, Africa, and Latin America High-risk groups (alcohol abusers, intravenous drug abusers, homeless persons, nursing home patients, prisoners, employees of hospitals or other health care facilities, children) Persons with medical risk factors (diabetes, silicosis, immunosuppressive therapy, prolonged corticosteroid therapy, chronic kidney disease, gastrectomy, jejunalileal bypass, malnutrition, certain malignancies) ≥ 15 mm All others; essentially, those who are considered low risk. In general, these individuals should not be tested in the first place. TB = tuberculosis; TNF-a = tumor necrosis factor-a. as other individuals with the endogenous and exogenous risk factors described previously.9 While there are no prospective studies for screening diabetic patients for LTBI, they are clearly at increased risk and thus it is prudent to perform tuberculin skin testing on diabetic patients, especially those who are insulin-dependent, poorly controlled, and/or in a population where TB is relatively more prevalent. In patients who are considered for treatment with anti-TNF-a agents (eg, infliximab, an antibody directed against TNF-a, or etanercept, a soluble form of p75 TNF-a receptor), tuberculin skin testing should be performed.10 If positive, probably at a criteria of 5 mm or greater, patients should be treated for LTBI prior to receiving anti-TNF-a therapy. Even with this preventive measure, reactivation TB has been described in patients who received anti-TNF-a agents. In recently exposed individuals who are historically known to be PPD-positive, preventive therapy can probably be withheld unless the subjects are HIV-positive. The rationale for this is that a number of case studies have shown that previous LTBI appears to protect individuals from developing TB from a new infection. All persons with LTBI should be clinically monitored for Hospital Physician Board Review Manual signs and symptoms that would indicate progression to active disease, such as fever, anorexia, weight loss, and any unexplained respiratory symptoms, whether they are treated or not. • What is the general algorithm for screening for latent infection? APPROACH TO POSITIVE SKIN TEST RESULT One important tenet in testing for LTBI is that if the skin test result is positive, treatment usually is indicated (ie, “the decision to test is a decision to treat”). Thus, low-risk individuals (Table) should not be tested because the likelihood that a positive test represents a true TB infection is small based on the combined effects of low pretest probability and the observation that infection with nontuberculous mycobacteria can cause a false-positive PPD result. The tuberculin skin test should be performed by injecting intradermally 0.1 mL of 5 tuberculin units of PPD into the volar surface of the forearm (Figure 2A). In many countries outside the United States, a tuberculin formulation known as RT-23 at a dose of 2 tuberculin units is often used. A 27-gauge needle is used to produce a wheal 6 to 10 mm in diameter. The diameter of the induration and not erythema is measured after 48 to 72 hours (Figure 2B), although it can be accurately read up to a week later. Only trained personnel should determine the degree of induration, as it has been shown that patients’ own evaluations of their test results are generally inaccurate.11 Three different diameters of induration are used as threshold values for treatment depending on host risk factors (Table). If both skin test result and review of symptoms are negative, treatment is not indicated (Figure 3) except in 2 instances. One exception is in children aged younger than 5 years or any children with additional risk factors for development of TB and known exposure to an active case (ie, even if the initial PPD skin test and chest radiograph are negative, empiric prophylactic therapy is recommended for at least 3 months).12 The tuberculin skin test is then repeated after 3 months and if negative, treatment can be discontinued; if the second tuberculin skin test is positive, isoniazid treatment should be continued for a total of 9 months. The other exception is the HIVpositive individual with a negative PPD test who has had a close contact exposure to an active case (ie, because the risk of progression to active disease is so high, these patients should be treated for LTBI despite a negative tuberculin skin test). If either skin test or symptom review is positive, a chest radiograph should be obtained and if abnormal, the individual should be ruled out www.turner-white.com D i a g n o s i s a n d Tr e a t m e n t o f L a t e n t Tu b e r c u l o s i s I n f e c t i o n Induration diameter Erythema diameter Tense tuberculin wheal Epidermis Needle 1.2 mm approx Dermis A B Subcutaneous tissue Figure 2. (A) The tuberculin skin test is performed by injecting 0.1 mL of 5 tuberculin units of purified protein derivative intradermally. (B) An example of a positive tuberculin skin test on the volar surface of a forearm. The diameter of the induration should be measured and recorded in millimeters. Erroneously measuring the diameter of the erythema instead will overestimate the true reaction size. (Photos obtained and slightly modified from a poster published by the Centers for Disease Control and Prevention.) for active TB with serial sputum for acid-fast staining and culture for mycobacteria (Figure 3). If the chest radiograph is normal in an asymptomatic person with a positive PPD test, then the patient is a candidate for LTBI treatment. The tuberculin skin test is not 100% sensitive for TB infection, and even among individuals with documented TB and no immunosuppression, up to 20% will have negative results on tuberculin skin testing. Testing with control antigens such as mumps and candida is not recommended since anergy testing lacks standardization, reproducibility, and positive predictive value for risk of M. tuberculosis infection and because reactivity to control antigens but not to PPD does not exclude TB infection.13 • What is the effect of previous bacille CalmetteGuerin (BCG) vaccine on the tuberculin skin test and its interpretation? The BCG vaccine was developed in 1924 from an attenuated strain of Mycobacterium bovis. It is used in many parts of the world but not in the United States. While BCG may cause a false-positive tuberculin skin test, most noninfected persons vaccinated with BCG are in fact skin test–negative to PPD, especially if they were vaccinated during infancy or early childhood.14 Thus, it has been recommended that prior BCG vaccination should not be a factor in either initiating or interpreting the skin test (ie, if the tuberculin skin test is positive, it is attributed to M. tuberculosis infection and the history of prior BCG is ignored). In patients with prior BCG vaccination, more recently developed bloodbased assays for interferon-γ (IFNγ) appear to have www.turner-white.com increased specificity for diagnosing LTBI.15–17 These IFNg-release assays are based on the principle that memory T cells in the blood, if they have been exposed to M. tuberculosis in the past, release larger amounts of IFNγ upon in vitro stimulation with M. tuberculosis– specific antigens (eg, ESAT-6 or CFP-10) than T cells from individuals who have not been previously exposed to M. tuberculosis. Two IFNγ-release assays are commercially available and both are based on the principle outlined above. The new tests are Quantiferon-TB (Cellestis Limited, Australia) and T-SPOT.TB (Oxford Immunotec, UK). The newest generation of the Quantiferon uses an “intube” method wherein either the ESAT-6 or CFP-10 antigen is already present in the blood-drawing tube. After the drawn blood is incu bated with an M. tuberculosis antigen for 16 to 24 hours at 37oC, IFNγ levels are measured by ELISA (enzyme-linked immunosorbent assay). The test result is considered positive if the IFNγ level in the tube containing M. tuberculosis antigen minus the IFNγ level in the control tube containing no antigen is 0.35 IU/mL or greater. As shown in Figure 4, the technique for T-SPOT.TB as compared with Quantiferon is different, although the principle is the same. For T-SPOT.TB, 250,000 peripheral blood mononuclear cells are aliquoted into each well of a 96-well tissue culture plate and performed as described in the Figure 4 legend. After incubation for 16 to 24 hours, the test result is considered positive if the patient sample stimulated with M. tuberculosis antigen has 6 or more spots (cells) compared with the unstimulated patient sample. Both IFNγ-release assays have sensitivities that are similar to tuberculin skin test, although T-SPOT.TB is likely to be Infectious Diseases Volume 10, Part 2 D i a g n o s i s a n d Tr e a t m e n t o f L a t e n t Tu b e r c u l o s i s I n f e c t i o n At-risk adult Tuberculin skin test (TST) + symptom review (ROS) Negative TST and negative ROS Positive TST or positive ROS High-risk exposure within 3 mos? Chest radiograph No Yes Treatment not indicated Normal Abnormal Candidate for treatment of latent tuberculosis infection Evaluate for active tuberculosis Figure 3. Tuberculosis screening flowchart. more sensitive than either tuberculin skin test or Quantiferon in patients who are lymphopenic due to advanced HIV infection or to cytotoxic agents. Specificities for Quantiferon and T-SPOT.TB in BCG-vaccinated persons with low risk of TB exposure are excellent, on the order of 96% to 99% and 86% to 99%, respectively.18,19 Similar to the tuberculin skin test, neither Quantiferon nor T-SPOT.TB are able to distinguish active TB from LTBI. • Can one induce induration in an uninfected person with serial PPD skin testing? No. PPD is not sensitizing. • What is the booster phenomenon? • What is the epidemiologic basis for treatment of LTBI? The booster phenomenon describes an initial negative skin test that upon subsequent testing is positive even though the person is not newly infected. This apparent conversion is actually a reflection of a prior LTBI in which waning immunity resulted in a falsenegative initial skin test. Two-step testing, in which a negative test is followed by a second test 1 week later, helps reduce the likelihood that boosted reactions will be interpreted as a new conversion should the person be retested at a later date (as in annual screening programs). Tuberculin positivity only after boosting is more common in the elderly, BCG vaccinees, and in persons exposed to nontuberculous mycobacteria. Persons with a booster response are at lower risk of reactivation than recent converters. Persons who will undergo annual tuberculin skin test (eg, health care workers) should undergo 2-step testing on initial evaluation. Hospital Physician Board Review Manual EVALUATION AND TREATMENT The case patient’s induration response to PPD showed an increase of 11 mm. Given her occupational risk of TB infection, the patient is started on treatment for LTBI. Based on a number of clinical trials, many of which were double-blind and placebo-controlled, there is compelling epidemiologic evidence that treatment of LTBI is efficacious in preventing disease provided patients adhere to treatment.20 The rationale for treating LTBI is not only to prevent active TB in the individual but also as a public health measure since most active TB cases are derived from the pool of LTBI. This beneficial public health effect of isoniazid preventive therapy is schematically shown in an initial 1963 Ferebee model21 updated by Iseman13 (Figure 5). As shown in this theoretical model, isoniazid decreases the number of cases of reactivation TB leading to a decrease in secondary TB infection and disease. • What is the standard recommended treatment for LTBI? www.turner-white.com D i a g n o s i s a n d Tr e a t m e n t o f L a t e n t Tu b e r c u l o s i s I n f e c t i o n ESAT-6 or CFP-10 Wash Add enzymeconjugated anti-IFNγ Add substrate antibody for detection Lymphocytes IFNγ A Anti-IFNγ ab Anti-IFNγ ab B Each spot = the “footprint” of 1 IFNγ-producing cell Figure 4. Basic technique of the T-SPOT.TB assay. After peripheral blood mononuclear cells (PBMCs) are isolated from blood, they are washed and counted and 250,000 cells are added to a well of a 96-well tissue culture plate that is precoated with anti-interferon-γ (IFNγ) antibody. Either ESAT-6 or CFP-10 Mycobacterium tuberculosis antigen is added to the well. A negative control well is one in which no M. tuberculosis antigen is added. After washing, an enzyme-conjugated anti-IFNγ antibody is added. In cells that produce IFNγ in response to stimulation with an M. tuberculosis antigen, dark-colored spots are generated by the catalytic action of the conjugated enzyme on the colo rimetric substrate; they are essentially footprints of the antigen-specific effector T cells in the sample. For example, in illustration A, the result would be 2 spots. Shown in B is an actual well in a T-SPOT.TB assay that demonstrates numerous IFNγ-producing lymphocytes. TREATMENT The preferred treatment of LTBI is 9 months of isoniazid.7,22 Two isoniazid regimens may be used: 5 mg/kg (maximum dose, 300 mg) daily for 9 months (preferable for self-administration) or 15 mg/kg (maximum dose, 900 mg) twice weekly for 9 months (preferable for directly observed preventive therapy). For those who are not infected with HIV, do not have fibrotic lesions on chest radiograph, and are older than 18 years, a shorter regimen consisting of 6 months of isoniazid 5 mg/kg (maximum dose, 300 mg) once daily or 15 mg/kg (maximum dose, 900 mg) twice weekly are acceptable but inferior alternatives to the 9-month regimen. For individuals with exposure to isoniazidresistant TB or who are intolerant to isoniazid, rifampin 600 mg once daily for 4 months is recommended. FOLLOW-UP The patient is nonadherent with daily isoniazid therapy. Based on the 2000 ATS guidelines,7 an infectious disease consultant recommends rifampin 600 mg once daily and pyrazinamide (PZA) 2 g once daily for 2 months. • Would you follow the consultant’s recommendations? MATCHING TREATMENT REGIMEN TO THE PATIENT This consultant’s recommendations should not be followed. Initially, based on 3 randomized trials in HIVinfected individuals comparing isoniazid preventive www.turner-white.com therapy (6–12 months) with 2 months of rifampinPZA, the latter regimen was found to be as efficacious as isoniazid without any apparent increase risk of adverse effects.23–25 Thus, to help improve compliance by shortening the length of therapy, 2 months of rifampin-PZA once daily or rifampin-PZA twice weekly for 2 to 3 months was recommended as a viable alternative.7 However, soon after the publication of the 2000 ATS guidelines, this 2-drug regimen was found to have a significantly greater risk of grade 3 hepatitis (liver enzymes > 5 times normal) or grade 4 hepatitis (liver enzymes > 10 times normal or > 5 times normal with compatible symptoms) with an initial report of 5 deaths from severe liver injury.26,27 As a result, the 2-month regimen of rifampin and PZA can no longer be recommended. Indeed, revised guidelines issued warning that the 2-month rifampin-PZA combination should be used with extreme caution and not be used in patients with alcoholism, chronic liver disease, or those with a history of isoniazid-induced liver toxicity.26 The most recent recommendation from the Centers for Disease Control and Prevention also emphasize that rifampin-PZA should not be offered for treatment of LTBI.28 In contrast to HIV-negative subjects, where the risk of hepatotoxicity of rifampin-PZA is greater than with isoniazid alone, the rifampin-PZA regimen appears to be as safe as isoniazid monotherapy in HIV-positive individuals.29 For individuals who are nevertheless put on rifampin-PZA dual therapy, stricter monitoring also was recommended: (1) no more than a 2-week supply of rifampin-PZA should be given; Infectious Diseases Volume 10, Part 2 D i a g n o s i s a n d Tr e a t m e n t o f L a t e n t Tu b e r c u l o s i s I n f e c t i o n 10 million infected 10 million infected 1 in 600 reactivate 1 in 1000 reactivate 16,000 reactivation 48,000 newly infected 20,000 cases annually 4000 new TB cases 10,000 reactivation 1 in 12 with TB 30,000 newly infected 250 million uninfected A 12,500 cases annually 2500 new TB cases 1 in 12 with TB 250 million uninfected B Figure 5. Illustration depicting (A) the theoretical cycle of development of tuberculosis (TB) infection and disease without isoniazid (INH) prophylaxis, and (B) reduction of reactivation disease, secondary infection, and secondary disease due to the effect of INH prophylaxis of an entire infected U.S. population (1998). (2) patients should be evaluated closely for symptoms and signs of hepatitis such as anorexia, nausea, emesis, abdominal pain, and jaundice; and (3) liver function tests should be obtained before starting therapy and at 2, 4, and 6 weeks after initiation of treatment, even in asymptomatic individuals.26,30 Thus, in the case patient, other measures to improve adherence (eg, isoniazid twice weekly under directly observed preventive therapy) should be tried before resorting to the riskier rifampin-PZA regimen. While it is not clear why the incidence of hepatitis with the rifampin-PZA combination appears to be greater than that with rifampin-PZA plus isoniazid, used for active TB, impaired host immunity during active disease may account for the decreased risk of liver injury even in those who received the 3-drug regimen.31 A decreased host immune response also is used to explain why treatment was not associated with a relatively alarming risk of hepatitis in the initial studies examining the use of rifampin-PZA in HIV-positive patients.31 While not mutually exclusive, an alternative explanation for the increased risk of hepatitis with rifampinPZA is that perhaps PZA in the absence of isoniazid may be metabolized to more hepatotoxic metabolites (M. Iseman, personal communication, December 2003). This interesting hypothesis is indirectly supported by the observation that the use of a fluoroquinolone plus PZA for LTBI due to a multidrug-resistant strain of M. tuberculosis in New York City and California also was associated with an unacceptable risk of hepatitis.32,33 Despite these concerns about rifampin-PZA hepatotoxicity, Stout and colleagues30 recently suggested that the Hospital Physician Board Review Manual rifampin-PZA regimen may be useful for high-risk, traditionally nonadherent groups (61% of their 114 patients were homeless and 17% drank alcohol excessively), albeit cautioning the need for close monitoring. However, the rate of confirmed and suspected cases of hepatitis in their cohort was 5.3%.30 In an accompanying editorial, Jasmer and Daley31 evaluated 5 separate rifampin-PZA regimen studies comprising over 1300 patients and found the overall frequency of grade 3 or 4 hepatitis to be 5.8%. This relatively high incidence of significant hepatitis is unacceptable as it is 19- to 53-fold greater than that seen with isoniazid preventive therapy, where the incidence of at least grade 3 hepatitis is estimated to be approximately 0.1% to 0.3%.34 Jasmer and Daley also questioned the claim of improved compliance with the shorter regimen by identifying a multicenter study that showed that there was no difference in the proportion of patients who completed therapy with 2 months of rifampin-PZA versus the 6 months of isoniazid (61% versus 57%, respectively; P > 0.2).27 • What is the recommended treatment of LTBI due to multidrug-resistant M. tuberculosis in someone with a PPD skin test conversion? MULTIDRUG-RESISTANT TB Prospective studies evaluating the treatment of LTBI caused by a presumed multidrug-resistant TB strain are lacking and thus such treatment is controversial. As previously noted, in high school students and teachers from Orange County, California33 and health care workers at Lincoln Hospital in Bronx, New York32 www.turner-white.com D i a g n o s i s a n d Tr e a t m e n t o f L a t e n t Tu b e r c u l o s i s I n f e c t i o n who were exposed to multidrug-resistant TB and were treated with ofloxacin and PZA, there was an unacceptably high risk of hepatitis (approximately 25%–32%). HIV-negative persons can be treated with drugs to which the tubercle bacilli is susceptible or observed for the development of active TB. HIV-positive persons should be treated with at least 2 drugs to which the strain is susceptible because the risk of progression to active TB is so high in this population. Alternatively, fluoroquinolone monotherapy without PZA may be considered with the caveat that long-term efficacy data on these treatments are lacking.7 Other recommended options include PZA-ethambutol or fluoroquinoloneethambutol regimens.35 suboptimal, as may be seen in homeless persons, alcoholics, or intravenous drug abusers, pyridoxine may decrease the incidence of isoniazid-induced peripheral neuropathy. Pyridoxine is also recommenced in pregnant women, persons with seizure disorders and in other conditions in which neuropathy is common (eg, diabetes, uremia, HIV infection). The dose of pyridoxine should be less than or equal to 10 mg per day, because larger doses may antagonize isoniazid itself.39 Indeed, very large doses of pyridoxine are recommended as an antidote for isoniazid overdose.40 • What are the adverse effects of isoniazid and who is at high risk of developing them? MONITORING FOR DRUG TOXICITIES Review of symptoms and physical examinations are the cornerstone of monitoring for drug toxicities with subsequent clinically indicated laboratory testing for confirmation (eg, liver function tests such as AST, alanine aminotransferase, alkaline phosphatase, and bilirubin). However, certain individuals should have liver function testing obtained at baseline and periodically during treatment, including HIV-infected subjects, pregnant women and those at least 3 months postpartum, alcoholics, patients with liver disease, or individuals taking other potentially hepatotoxic medications.7 The major adverse effects of isoniazid are hepatitis, peripheral neuropathy, anaphylaxis, and psychosis, while minor side effects include headache, rash, nausea, and nonspecific abdominal pain not necessarily associated with hepatitis.36–38 Risk of isoniazid-associated hepatitis (defined as symptoms consistent with hepatitis, aspartate aminotransferases [AST] levels ≥ 5 times normal levels, and resolution of signs and symptoms of hepatotoxicity after withdrawal of isoniazid) is 0.1% in persons younger than age 35 years and approximately 0.2% to 0.3% in persons aged 35 or older.34 Risk increases with age, current alcohol use, ingestion of other hepatotoxic drugs, and chronic hepatitis B or C infection. For the standard isoniazid regimen for LTBI, baseline and follow-up liver function tests are not routinely indicated except for those individuals with HIV infection, pregnancy, or history of chronic liver disease or in those who regularly drink alcohol.7 Subjects should be evaluated monthly for adherence to the regimen and to uncover any symptoms suggestive of hepatitis. Patients should abstain from alcohol and other potential hepatotoxins. Clinical signs of hepatitis such as fever, fatigue, nausea, vomiting, and jaundice should be monitored. Mild elevations of hepatic transaminases are common and in the absence of symptoms do not necessarily require interruption of medication. If AST and alanine aminotransferase levels are 5 times the upper limit of normal, or if 3 times normal with compatible symptoms, then isoniazid should be discontinued. • Should vitamin B6 be given with isoniazid preventive therapy and, if so, what is the recommended dose? Vitamin B6 (pyridoxine) is not routinely recommended with isoniazid preventive therapy in individuals with adequate nutrition. However, when the diet is www.turner-white.com • What is the recommendation for monitoring for drug toxicity in the treatment of LTBI? SUMMARY One third of the world’s population is latently infected with M. tuberculosis. From this pool, approximately 9 million active TB cases emerge annually, resulting in 2 to 3 million deaths and making TB the second most common cause of death by a single infectious agent in the world. In otherwise healthy individuals with LTBI, the lifetime risk for active TB is approximately 5% within the first year of infection and 5% for the remainder of the lifetime of the individual. Perhaps the single most important host risk factor for reactivation TB is coinfection with HIV, where the estimated rate of reactivation is approximately 5% to 10% per year. Other particularly high-risk individuals include those with upper lobe fibronodular scarring, recent immigrants from regions endemic for TB, nursing home residents, and persons with silicosis, chronic kidney disease, gastrectomy, malnutrition, diabetes mellitus, organ transplantation, or immunosuppressive use. Testing for latent infection involves administering 0.1 mL of 5 tuberculin units of PPD (or 0.1 mL of 2 tuberculin units of RT-23, available in many places outside the United States) intradermally and Infectious Diseases Volume 10, Part 2 D i a g n o s i s a n d Tr e a t m e n t o f L a t e n t Tu b e r c u l o s i s I n f e c t i o n measuring the diameter of induration at 48 to 72 hours. There is compelling epidemiologic evidence that treatment for LTBI decreases the development of active TB. The preferred treatment regimen of LTBI is 9 months of isoniazid for those with normal chest radiographs. Correctly diagnosing and treating individuals with LTBI are important cornerstones to curbing the scourge of TB. Acknowledgment The authors thank Drs. Marian Goble, Carol Welsh, Brian Fouty, and Michael Iseman for critical review of the manuscript. 13. Mandell GL, Bennett JE, Dolin R, editors. Principles and practice of infectious diseases. 6th ed. London: Churchill Livingstone; 2004:2860. 14. Menzies R, Vissandjee B. Effect of bacille Calmette-Guerin vaccination on tuberculin reactivity. Am Rev Respir Dis 1992;145:621–5. 15. Mori T, Sakatani M, Yamagishi F, et al. Specific detection of tuberculosis infection: an interferon-a-based assay using new antigens. Am J Respir Crit Care Med 2004;170:59–64. 16. Brock I, Weldingh K, Lillebaek T, et al. Comparison of tuberculin skin test and new specific blood test in tuberculosis contacts. Am J Respir Crit Care Med 2004;170:65–9. 17. Barnes PF. Diagnosing latent tuberculosis infection: turning glitter to gold. Am J Respir Crit Care Med 2004;170:5,6. REFERENCES 18. Richeldi L. An update on the diagnosis of tuberculosis infection. Am J Respir Crit Care Med 2006;174:736–42. 1. Raviglione MC, Snider DEJ, Kochi A. Global epidemiology of tuberculosis. Morbidity and mortality of a worldwide epidemic. JAMA 1995;273:220–6. 19. Menzies D, Pai M, Comstock G. Meta-analysis: new tests for the diagnosis of latent tuberculosis infection: areas of uncertainty and recommendations for research. Ann Intern Med 2007;146:340–54. 2. Lienhardt C, Rodrigues LC. Estimation of the impact of human immunodeficiency virus infection on tuberculosis: tuberculosis risks re-visited? Int J Tuberc Lung Dis 1997;1:196–204. 20. Iseman MD. A clinician’s guide to tuberculosis. Philadelphia: Lippincott, Williams & Wilkins; 2000:355–97. 3. WHO report: global tuberculosis control: surveillance, planning, financing. Geneva: World Health Organization; 2002. 21. Ferebee SH. An epidemiological model of tuberculosis in the United States. TB control: with present methods? with BCG vaccination? or with isoniazid prophylaxis? NTA Bull 1967;53:4–7. 4. Cantwell MF, Snider DE Jr, Cauthen GM, Onorato IM. Epidemiology of tuberculosis in the United States, 1985 through 1992. JAMA 1992;272:535–9. 22. Comstock GW. How much isoniazid is needed for prevention of tuberculosis among immunocompetent adults. Int J Tuberc Lung Dis 1999;3:847–50. 5. Blumberg HM, Burman WJ, Chaisson RE, et al. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med 2003;167:603–62. 23. Gordin F, Chaisson RE, Matts JP, et al. Rifampin and pyrazinamide vs isoniazid for prevention of tuberculosis in HIV-infected persons: an international randomized trial. Terry Beirn Community Programs for Clinical Research on AIDS, the Adults AIDS Clinical Trials Group, the Pan American Health Organization, and the Centers for Disease Control and Prevention Study Group. JAMA 2000;283:1445–50. 6. Chan ED, Iseman MD. Current medical treatment for tuberculosis. BMJ 2002;325:1282–6. 7. Targeted tuberculin testing and treatment of latent tuberculosis infection. Am J Respir Crit Care Med 2000;161(4 Pt 2):S221–47. 8. Stead WW, Lofgren JP, Warren E, Thomas C. Tuberculosis as an endemic and nosocomial infection among the elderly in nursing homes. N Engl J Med 1985;312:1483–7. 9. Small PM, Fujiwara PI. Management of tuberculosis in the United States. N Engl J Med 2001;345:189–200. 10. Ellerin T, Rubin RH, Weinblatt ME. Infections and antitumor necrosis factor a therapy. Arth Rheum 2003;48:3013– 22. 11. Howard TP, Solomon DA. Reading the tuberculin skin test: Who, when, and how? Arch Intern Med 1988;148:2457–9. 12. Starke JR. Mycobacterium tuberculosis. In: Rudolph CD, Rudolph AM, Hostetter MK, et al, editors. Rudolph’s ped iatrics. 21st ed. Philadelphia: McGraw-Hill, Medical Pub Division; 2003:949–59. 10 Hospital Physician Board Review Manual 24. Halsey NA, Coberly JS, Desormeaux J, et al. Randomised trial of isoniazid versus rifampicin and pyrazinamide for prevention of tuberculosis in HIV-1 infection. Lancet 1998;351:786–92. 25. Mwinga A, Hosp M, Godfrey-Faussett P, et al. Twice weekly tuberculosis preventive therapy in HIV infection in Zambia. AIDS 1998;12:2447–57. 26. Centers for Disease Control and Prevention. Update: fatal and severe liver injuries associated with rifampin and pyrazinamide for latent tuberculosis infection, and revisions in the American Thoracic Society/CDC recommendations—United States, 2001. MMWR Morb Mortal Wkly Rep 2001;50:733–5. 27. Jasmer RM, Saukkonen JJ, Blumberg HM, et al. Shortcourse rifampin and pyrazinamide compared with isoniazid for latent tuberculosis infection: a multicenter clinical www.turner-white.com D i a g n o s i s a n d Tr e a t m e n t o f L a t e n t Tu b e r c u l o s i s I n f e c t i o n trial. Ann Intern Med 2002;137:640–7. 28. Centers for Disease Control and Prevention (CDC); American Thoracic Society. Update: adverse event data and revised American Thoracic Society/CDC recommendations against the use of rifampin and pyrazinamide for treatment of latent tuberculosis infection—United States, 2003. MMWR Morb Mortal Wkly Rep 2003;52:735–9. 29. Gordin FM, Cohn DL, Matts JP, et al. Hepatotoxicity of rifampin and pyrazinamide in the treatment of latent tuberculosis infection in HIV-infected persons: is it different than in HIV-uninfected persons? Clin Infect Dis 2004;39:561–5. 30. Stout JE, Engemann JJ, Cheng AC, et al. Safety of 2 months of rifampin and pyrazinamide for treatment of latent tuberculosis. Am J Respir Crit Care Med 2003;167:824–7. 31. Jasmer RM, Daley CL. Rifampin and pyrazinamide for treatment of latent tuberculosis infection: is it safe? Am J Respir Crit Care Med 2003;167:809–12. 32. Horn DL, Hewlett D Jr, Alfalla C, et al. Limited tolerance of ofloxacin and pyrazinamide prophylaxis against tuberculosis. N Engl J Med 1994;330:1241. 33. Ridzon R, Meador J, Maxwell R, et al. Asymptomatic hepatitis in persons who received alternative preventive therapy with pyrazinamide and ofloxacin. Clin Infect Dis 1997;24:1264–5. 34. Nolan CM, Goldberg SV, Buskin SE. Hepatotoxicity associated with isoniazid preventive therapy: a 7-year survey from a Public Health Tuberculosis Clinic. JAMA 1999;281:1014– 8. 35. Management of persons exposed to multidrug-resistant tuberculosis. MMWR Recomm Rep 1992;41(RR-11):61–71. 36. Alao AO, Yolles JC. Isoniazid-induced psychosis. Ann Pharmacother 1998;32:889–91. 37. Crook M. Isoniazid-induced anaphylaxis. J Clin Pharmacol 2003;43:545–6. 38. LoBue PA, Moser KS. Use of isoniazid for latent tuberculosis infection in a public health clinic. Am J Respir Crit Care Med 2003;168:443–7. 39. Snider DE Jr. Pyridoxine supplementation during isoniazid therapy. Tubercle 1980;4:191–6. 40. Chan ED, Terada LS, Kortbeek J, Winston BW. Bedside critical care manual. 2nd ed. Philadelphia: Hanley & Belfus; 2002:102–3. Copyright 2007 by Turner White Communications Inc., Wayne, PA. All rights reserved. www.turner-white.com Infectious Diseases Volume 10, Part 2 11