Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Mitral insufficiency wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
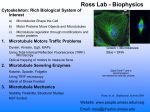
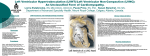
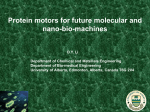
Microtubule Involvement in the Adaptation to Altered Mechanical Load in Developing Chick Myocardium Elizabeth A. Schroder, Kimimasa Tobita, Joseph P. Tinney, Jane K. Foldes, Bradley B. Keller Downloaded from http://circres.ahajournals.org/ by guest on August 12, 2017 Abstract—Mechanical load regulates ventricular growth, function, and structure from the earliest stages of cardiac morphogenesis through senescence. Dramatic changes in cardiac form and function have been defined for developing cardiovascular systems, and changes in mechanical loading conditions can produce structural malformations such as left heart hypoplasia. To date, relatively little is known regarding the interactions between changes in mechanical load, morphogenesis, and the material properties of the embryonic heart. We tested the hypothesis that passive material properties in the embryonic heart change in response to altered mechanical load and that microtubules play an important role in this adaptive response. We measured biaxial passive stress-strain relations in left ventricular (LV) myocardial strips in chick embryos at Hamburger-Hamilton stage 27 following left atrial ligation (LAL) at stage 21 to reduce LV volume load and create left heart hypoplasia. Following LAL, myocardial stresses at given strains and circumferential stiffness increased versus control strips. Western blot analysis of LAL embryos showed an increase in both total and polymerized -tubulin and confocal microscopy confirmed an increase in microtubule density in the LV compact layer versus control. Following colchicine treatment, LV stresses and stiffness normalized in LAL specimens and microtubule density following colchicine was similar in LAL to control. In contrast, Taxol treatment increased myocardial stresses and stiffness in control strips to levels beyond LAL specimens. Thus, the material properties of the developing myocardium are regulated by mechanical load and microtubules play a role in this adaptive response during cardiac morphogenesis. (Circ Res. 2002;91:353-359.) Key Words: embryonic ventricle 䡲 cardiac morphogenesis 䡲 viscoelastic properties 䡲 -tubulin 䡲 microtubules T syndrome (HLHS) in the chick embryo,10,11,14 whereas increased ventricular load produced by conotruncal (arterial) banding accelerates myocardial growth via hyperplasia.9,10 Similar changes in mechanical load alter cardiac growth and function in the fetal heart and young infant.15,16 Although the relationship between changes in ventricular load, function, and structure is well documented, we know very little regarding the intracellular and extracellular mechanisms responsible for this adaptation in the developing myocardium. Changes in microtubule content and distribution in response to altered mechanical load have been shown to directly affect cardiomyocyte structure and function in feline, canine, and human myocardium.17–20 Cardiomyocyte hypertrophy is also associated with increased density of the intracellular microtubular network resulting in increased viscous damping.21 Drugs such as colchicine that depolymerize microtubules have been shown to restore passive stiffness to control values in some but not all models of myocardial hypertrophy.22–25 Although microtubules may not be a major determinant in the passive properties of normal adult heart,21,23 microtubules have been shown to contribute to the contractile dysfunction noted in hypertrophic and dilated cardiomyopathy.20,21,26,27 Hatcher et al28 investigated the he adaptation of ventricular function and structure to altered mechanical load is a fundamental property of the myocardium present from the earliest stages of cardiac morphogenesis through senescence. Embryonic heart rate, blood pressure, and cardiac output increase geometrically during formation of the heart and blood vessels1–3 and the developing heart undergoes a dramatic transformation in 3-dimensional structure coincident with rapid cardiomyocyte clonal expansion and differentiation.1,2,4,5 Although there are numerous examples of single-gene defects associated with congenital cardiac malformations, most single-gene models of congenital heart disease display a wide variation in phenotype, suggesting an important role for modifying genes as well as epigenetic or environmental factors.6 – 8 Experimental interventions that increase or decrease mechanical load during cardiac development result in both changes in cardiac function and structure.9 –11 With a peak systolic pressure of less than 10 mm Hg and an end-diastolic pressure of less than 2 mm Hg during early cardiac morphogenesis, the developing myocardium responds rapidly to changes in mechanical load to maintain cardiac output.12,13 Inflow occlusion of the developing left ventricle produced by left-atrial ligation (LAL) produces hypoplastic left heart Original received February 22, 2002; revision received June 21, 2002; accepted July 9, 2002. From Cardiovascular Development Research Program, Department of Pediatrics, University of Kentucky, Lexington, Ky. Correspondence to Bradley B. Keller, Dept of Pediatrics, University of Pittsburgh, 3705 Fifth Ave, Pittsburgh, PA 15213-2583. E-mail [email protected] © 2002 American Heart Association, Inc. Circulation Research is available at http://www.circresaha.org DOI: 10.1161/01.RES.0000030179.78135.FA 353 354 Circulation Research August 23, 2002 Downloaded from http://circres.ahajournals.org/ by guest on August 12, 2017 relationship between microtubules and the decrease in ventricular function noted in chick embryos after neural crest ablation; however, no change in microtubule content was found. In the present study, we tested the hypothesis that microtubules are involved in the adaptive response of the developing myocardium to altered mechanical load. We measured biaxial passive left ventricle (LV) stress-strain relations in chick embryos after LAL known to reduce LV volume load and produce HLHS.11 After LAL, myocardial stresses at given strains and circumferential stiffness increased versus control strips. Western blot analysis of LAL embryos showed an increase in both total and polymerized -tubulin and confocal microscopy confirmed an increase in microtubule density in LV compact myocardium versus control. After colchicine treatment, LV stresses and stiffness normalized in LAL specimens and microtubule density after colchicine was similar in LAL to controls. Taxol treatment, which hyperpolymerizes microtubules, increased myocardial stresses and stiffness in control strips to levels beyond LAL specimens. Thus, the material properties of the developing myocardium are regulated by mechanical load and microtubules play a role in this adaptive response during cardiac morphogenesis. Materials and Methods Embryo Selection Fertile White Leghorn chicken eggs (CBT Farms, Chestertown, Md) were incubated in a forced-draft, constant-humidity incubator and studied at Hamburger-Hamilton stage 27 (5 days) of a 46-stage (21 day) incubation period as previously described.29 At the selected stage the embryonic ventricle has externally distinct RV and LV chambers with common atrioventricular (AV) canal, large interventricular communication, and common outflow tract.30 Embryos that were dysmorphic or exhibited overt bleeding were excluded. Our research protocols conform to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85-23, revised 1985). Left Atrial Ligation (LAL) to Reduce Left Ventricular Preload Embryos were initially incubated to stage 21. A 1-cm2 hole was made in the shell and the inner shell and extraembryonic membranes were removed to expose the developing embryo. The embryo was then gently positioned left side up and microforceps were used to make a slit-like opening in the thoracic wall above the primitive left atrium. A loop of 10 to 0 nylon suture tied with an overhand knot was then placed across the primitive left atrium and tightened, decreasing the effective volume of the left atrium and thus redistributing blood from the left to the right ventricle.10,11,14 Each embryo was then repositioned to its original right side up orientation, the eggshell opening was sealed with parafilm, and reincubated until stage 27. Preparation of Myocardial Strips for Mechanical Testing Hamburger and Hamilton (1951) stage 27 embryos (normal and LAL) were excised and placed in a Petri dish containing hypothermic (25°C), hyperkalemic chick ringer solution (in mmol/L: 82 NaCl, 60 KCl, 2 CaCl2, 10 Trizma- HCl, and 10 Trizma-base) adjusted to pH 7.4 to arrest the heart during diastole.31 The ventricle was removed from the embryo by cutting along the AV groove and across the conotruncal cushions. Myocardial strips were dissected from the LV free wall in both a longitudinal (LNG) and a circumferential (CIR) orientation. We defined the LNG direction of the cardiac coordinate system by an axis from the midpoint of the primitive AV valve to the LV apex. Average cross-sectional area was not significantly different between experimental groups cut in LNG (0.1790⫾0.0140 versus 0.1860⫾0.0162 mm2; normal versus LAL, respectively) or CIR (0.1476⫾0.0107 versus 0.1362⫾0.0162 mm2; normal versus LAL, respectively) orientations. After excision, strip length was measured and then the specimens were mounted on our force workstation as previously described.31 Microspheres (10 m) were placed on the epicardial surface of the ventricular strip in a triangular pattern such that the centroid of the triangle aligned with the central axis of the wires and was midway between their ends. Microsphere spacing averaged 100 m. A custom linear motor stretched the ventricular segment in a triangular ramp pattern at a velocity of 0.2 mm/s at 30% above the excised length. Myocardial strips were preconditioned for 1 minute at 30% stretch and then data were recorded for the range of 0 to 0.25 longitudinal strain. Myocardial strip dimensions and strain patterns during stretch were monitored using a video microscopy system and by internal length sensors in the displacement motor. While the ventricle was being stretched, we recorded passive force-strain measurements in isolated LV strips using a custom analog-digital signal and image acquisition system.11 The data acquisition system simultaneously acquired force and strain data at 100 Hz (LabVIEW, National Instruments) and 10 Hz (NIH image 1.62), respectively. Two-dimensional epicardial wall strain was determined by tracking triangular arrays of microspheres from acquired images.31 Embryonic LV geometry at the study stage is complex11,30 and the ventricular wall is composed of an inner trabeculae layer with varying intertrabecular spaces and a thin outer compact myocardium. Because it is not technically feasible to acquire realistic 3-dimensional data of the trabeculated embryonic wall during stretching, basic geometric assumptions are required in order to estimate myocardial stresses. Therefore, for this study, we considered the embryonic LV myocardium to be a freely deforming solid body composed of isotropic and incompressible elastic material. Wall stresses at the midportion of the myocardial strip during stretch were calculated as force divided by cross-sectional area, assuming a cylindrical geometry. Passive stress-strain relations were fit by the following equation32: ⫽a Exp(bE), where , a, b, and E, are, respectively, midwall stress, midwall stress at zero strain, myocardial stiffness constant, and Lagrange strain. We chose “excision length” as the reference state. We recognize that this passive reference state is not a completely unloaded state due to residual stress in the embryonic myocardium.33 To determine b from the stress-strain relations in each embryo, we used a quasi-Newton algorithm to minimize least square loss function. Convergence criterion was set to 0.0001. All calculations were performed using Sigma Plot (SPSS Inc). Normalized hysteresis loop area, a measure of viscous damping, was calculated as the loop area between the stress-strain relationship during an increase (loading) and decrease (unloading) in stress divided by the total area under the loading portion of the curve.21,34,35 When stress is increased, the area under the stress strain relation is equal to the potential energy gained by the muscle strip during stretch. When stress is decreased, the energy returned to the system is equal to the integral of the stress-strain relation. If damping occurs, there will be a difference between the energy gained during stretch and the energy returned during release. This loop area represents the energy lost to heat and reflects the resistance to stretch associated with viscosity. Assessment of Microtubule Contribution to Passive Properties To examine the contribution of microtubule density on the passive properties of the embryonic myocardium, excised specimens (CIR or LNG strips) were placed in 50 mol/L colchicine (Sigma)/chick ringer solution on ice for 1 hour28 or in 25 mol/L Taxol (Cytoskeleton Inc)/chick ringer solution at 37°C for 4 hours. Colchicine binds tightly to the -tubulin subunit, prevents polymerization, and results in a rapid destabilization of microtubules. Taxol lowers the critical concentration of ␣-tubulin heterodimers required to form microtu- Schroder et al Microtubules in Embryonic Heart 355 Figure 1. Average stress-strain relationships for stage 27 LV specimens. Black circles indicate control specimens; white circles, control specimens after colchicine treatment; gray circles, control specimens after Taxol treatment; black triangles, LAL specimens; white triangles, LAL specimens after colchicine treatment. *P⬍0.05 vs stage 27 normal. bules, thus increasing microtubule density via the hyperpolymerization of existing microtubules and the formation of aberrant, nonfunctional microtubules. Strips were then attached to the transducer and motor and stretched following the aforementioned protocol. Downloaded from http://circres.ahajournals.org/ by guest on August 12, 2017 SDS-PAGE and Western Blot Analysis of -Tubulin Whole cell lysates were prepared from LV specimens (control and LAL groups, with and without colchicine treatment). Polymerized -tubulin content was assessed following the protocol outlined by Hatcher.28 SDS-PAGE (7% separating gel) and immunoblotting were carried out following routine protocols. Mouse monoclonal anti–-tubulin antibody (Sigma) was visualized with a horseradish peroxidase-conjugated secondary antibody (Jackson Immunolaboratories) and chemiluminescence (Amersham). Each lane contained protein prepared from 10 LV specimens (30 to 40 g total protein). Ventricular dimensions are comparable in control and LAL embryos at this developmental stage.11 All Western blot experiments were repeated at least 3 times to ensure that experimental observations were reproducible. Known amounts of purified tubulin (Cytoskeleton Inc) were run on each gel to allow for the quantification of both total and polymerized -tubulin. Immunoblots were scanned on an HP ScanJet 4c and quantified using densitometry (Scion Image, Scion Corporation). Confocal Microscopy and Immunofluorescence Protocols The embryonic heart was arrested by injection of 20 L of 25°C hyperkalemic chick Ringer solution containing (in mmol/L) 82 NaCl, 60 KCl, 2 CaCl2, 10 Trizma- HCl, and 10 Trizma-base, pH 7.4 via the sinus venosus. Each embryo was fixed in cold methanol with 1 mmol/L EGTA. After fixation, the heart was removed from the embryo and then carefully placed in a LNG orientation within a 13% polyacrylamide gel that was immediately polymerized with 2% ammonium persulfate.36 Polyacrylamide-embedded hearts were sectioned at 100 m with a standard vibrotome (VT1000S, Leica, Germany). Sections representing LV myocardium were permeabilized with 0.1% Triton X-100 for 30 minutes and were stained for f-actin with FITC-conjugated phalloidin (Molecular Probes) and for -tubulin with mouse monoclonal anti–-tubulin primary antibody (Sigma) and Alexa 568 (IgG1 specific, Molecular Probes) secondary antibody. LV myocardium at the midventricular level was examined using a Leica confocal microscopy system (Model TCS Laser Scanning Confocal Microscope System, Leica, Germany). Laser power, aperture, opening percentage, and gain of the confocal system were selected to minimize background fluorescence and to optimize the fluorescence intensity of the trabecular myocardium. Once this protocol was established, similar settings were used for all specimens. Z-Serial optical sectioning was performed for a z-depth of 100 m at an interval of 1 m using a 63⫻ water-immersion objective. Stacks of 50 z-serial section images were captured and saved digitally. The middle 20 consecutive sections from each stacked image were projected using maximum intensity point projection for subsequent image analysis. Statistical Analysis Data are presented as mean⫾SE. Two-factor repeated analysis of variance (ANOVA) was performed to compare the mean values of stress-strain relations between experimental groups. Two-factor ANOVA was performed to compare mean values of wall stress, strain components, and b between experimental groups. Individual comparisons were performed using a Tukey test. Statistical significance was defined by a value of P⬍0.05. All calculations were performed using SigmaStat (SPSS Inc). Results Passive Material Properties of Embryonic LV Strips LV myocardial strips from control and LAL embryos yielded reproducible passive stress-strain curves in more than 90% of experiments. Myocardial stresses at given strains and CIR myocardial stiffness were significantly increased after LAL (P⬍0.05 versus normal stage 27; Figure 1 and Table 1). This suggests an increase in the stiffness of the passive elastic component. After colchicine treatment, LV stress and stiffness were unchanged for control embryos; however, colchicine treatment reduced LAL values to control values (P⬍0.05). Taxol treatment resulted in an increase in stresses at given strains and myocardial stiffness in both the LNG and CIR directions. Mean hysteresis loop energy, a measure of viscous damping, was increased in LAL LV and Taxoltreated control specimens (both CIR and LNG) compared with controls (Table 2). Western Blot Analysis for -Tubulin Total and polymerized -tubulin increased at stage 27 after LAL compared with control (Figure 2). After colchicine treatment, there was no significant difference in the amount of polymerized -tubulin between LAL and control groups. Immunohistochemistry Indirect immunofluorescence images of LV specimens showed that microtubules form a reticular or randomly arranged network pattern in the compact myocardium. In normal developing LV, microtubular density in the compact myocardium was lower than in the trabecular myocardium, whereas the compact myocardial microtubular density increased after LAL (Figure 3). Colchicine treatment of LAL 356 Circulation Research TABLE 1. August 23, 2002 Ventricular Curve Statistics Left Ventricle S 27 N S 27 NColchicine S 27 NTaxol S 27 LAL S 27 LALColchicine Circumferential n 8 9 4 6 7 a, mg/mm2 8.47⫾1.83 9.84⫾2.43 1.14⫾0.68* 10.56⫾1.28 8.32⫾2.97 Stiffness constant b 7.53⫾0.87 8.64⫾1.04 26.91⫾4.38* 11.37⫾1.04* 9.54⫾1.06 r 0.99⫾0.001 0.99⫾0.002 0.98⫾0.001 0.99⫾0.001 0.98⫾0.005 9 10 7 10 8 Longitudinal n 2 a, mg/mm 5.14⫾0.93† 4.93⫾1.78† 4.47⫾2.8 12.93⫾1.57* 7.29⫾4.48 Stiffness constant b 7.79⫾0.50 9.01⫾1.01 19.72⫾1.68* 7.71⫾0.39† 10.09⫾1.09 r 0.99⫾0.007 0.98⫾0.004 0.97⫾0.017 0.99⫾0.001 0.99⫾0.002 S indicates Hamburger-Hamilton stage; N, normal; and LAL, left atrial ligation. Mean⫾SE. *P⬍0.05 vs stage 27 normal; †P⬍0.05 vs circumferential. Downloaded from http://circres.ahajournals.org/ by guest on August 12, 2017 specimens reduced the microtubular density in both compact and trabecular myocardium to the levels observed in control embryos. Discussion Formation of the heart and blood vessels occurs within an active biomechanical environment. During the period of primary cardiac morphogenesis, the embryonic cardiovascular (CV) system operates at a peak systolic pressure of less than 10 mm Hg and each of the parameters that influence cardiac output have stage-specific optimized values.12 Despite relative structural immaturity, the embryonic heart dynamically varies heart rate, preload, afterload, and viscoelastic properties influencing the final structure and function of the heart. Experimental models of congenital heart disease in the chick embryo include left heart hypoplasia produced by LAL,11,37 double outlet right ventricle produced by altered venous return,38 and conotruncal defects produced by neural crest ablation,39 and each has clinical correlates to human anomalies. Previous studies have focused on the changes in systolic properties that occur in these malformations,11,40 but our present study investigated changes in passive material properties after LAL and identified an increase in microtubules that may explain, in part, the increased passive stiffness observed in the LAL LV.31 For the low-pressure embryonic cardiovascular system, changes in diastolic function may be a critical regulatory pathway during morphogenesis of the heart.41 TABLE 2. We assessed myocardial stiffness in the embryonic myocardium using uniaxial loading of specimens with biaxial surface strain measurements and found that myocardial stresses at given strains, circumferential myocardial stiffness, and hysteresis loop area increased in response to reduced mechanical load. This increase in passive stiffness of embryonic myocardium in response to reduced mechanical load is in contrast to the response of the adult myocardium to unloading.42,43 Rothen-Rutishauser et al44 observed distinct differences in neonatal rat cardiomyocytes and adult rat cardiomyocytes in their requirement for intact microtubules in culture. They showed that adult cardiomyocytes lose a certain degree of flexibility due to their longer adaptation to specific situations in the heart, whereas neonatal cardiomyocytes can maintain and reassemble myofibrils even after microtubules are destroyed. This adaptability to the environment may allow immature cardiomyocytes to remodel in response to reduced mechanical load differently from the loss of structural and functional integrity observed in unloaded adult heart.42 Although LAL initially reduced LV loading, the subsequent increase in passive stiffness after LAL more closely resembled the changes in passive stiffness that occur in adult myocardium in response to increased mechanical load. We therefore investigated the role of microtubules in our LAL model because increased microtubule content has been associated with increased viscous damping in hypertrophied adult myocardium.21 Much work has been done defining the role of microtubules in pressure-overload hypertrophy models of the adult Hysteresis Area Percent Left Ventricle S 27 N S 27 NColchicine S 27 NTaxol S 27 LAL S 27 LALColchicine Circumferential n Hysteresis area percent 8 9 4 6 7 18.10⫾3.79 19.11⫾5.24 55.90⫾13.01* 37.30⫾9.20* 23.90⫾5.97† Longitudinal n Hysteresis area percent 9 10 7 10 8 24.24⫾6.01 25.42⫾9.93 64.93⫾8.46* 42.83⫾4.96* 27.35⫾4.04† S indicates Hamburger-Hamilton stage; N, normal; and LAL, left atrial ligation. Mean⫾SE. *P⬍0.05 vs stage 27 normal; †P⬍0.05 vs untreated buffer. Schroder et al Downloaded from http://circres.ahajournals.org/ by guest on August 12, 2017 Figure 2. Representative Western blot of total and polymerized -tubulin before and after colchicine treatment for normal and LAL left ventricular specimens. A 0.5-g standard of purified tubulin is shown in the first Western lane. Corresponding summary data for total and polymerized -tubulin before and after colchicine treatment for normal (filled) and LAL (open) left ventricular specimens are directly beneath the matching Western lane. *P⬍0.05 vs control. heart.19,21,23–25,27,45 Increased microtubule content has been suggested as one maladaptive mechanism that occurs in pressure-overload hypertrophy,46 and data in the feline heart support the view that microtubular stabilization is an important factor contributing to increased cytoskeletal stiffness and contractile dysfunction.27 To date, however, very little has been done to evaluate the role of microtubules in cardiac morphogenesis and function. Microtubules have been shown to be important regulators of cellular organization and myofibrillogenesis,47,48 and they mediate the transport of materi- Figure 3. Representative photomicrographs of -tubulin immunofluorescence in normal and LAL left ventricular specimens before and after colchicine treatment. Note the increased density of microtubules in the compact myocardium after LAL. After colchicine treatment, microtubule density appears similar to control in both normal and LAL specimens. White double arrow designates the compact myocardium. Scale bar⫽30 m. Microtubules in Embryonic Heart 357 als necessary for the production of new cellular structures. Thus, it seemed reasonable to consider that microtubules may play a role in mediating the adaptive response of the developing myocardium to altered mechanical load. Western blot analysis and confocal images showed an increase in total -tubulin content as well as an increase in polymerized -tubulin present in the LV myocardium of LAL embryos versus stage-matched controls. Colchicine treatment returned protein levels to those observed in normal hearts. However, the mechanisms that regulate tubulin synthesis and microtubule stabilization in response to altered mechanical stress have not yet been defined. We also noted a change in the viscous properties of the embryonic myocardium after LAL, as assessed by hysteresis loop area during stretch and release.21,34,35,49,50 This was apparent as a decrease in force during release after stretch, which resulted in an increase in loop area. This increase in hysteresis loop area following LAL normalized after colchicine treatment and microtubule depolymerization. Taxol treatment increased hysteresis loop area when compared with control. Unlike changes that occur in vivo in response to altered mechanical load (LAL), Taxol treatment in vitro results in an unregulated hyperpolymerization of microtubules. These results are consistent with the association between increased microtubule content and increased viscous damping in adult myocytes from hypertrophied canine, feline, and human heart failure specimens,20,21,27 although not all laboratories concur with these results.23–25 The mechanism by which increased microtubule density effects viscous properties is not well understood. In adult myocytes, microtubules are concentrated in the perinuclear regions.47 When microtubular density increases, it occurs throughout all regions of the cell, extending along the entire length of the sarcomere, thus contributing to increased diastolic stiffness and viscous resistance. Our Western and confocal images show that microtubules form a reticular or randomly arranged network pattern in the compact myocardium with an increase in both intensity and density of microtubules in the LAL specimens. This increase may contribute to both diastolic stiffness and viscous resistance. Changes in the viscous properties of the developing myocardium could also impact diastolic function and contribute to changes in ventricular filling patterns similar to pathological states of diastolic dysfunction in the adult heart.21,51–53 It is important to note that in the adult heart passive elasticity is influenced by a wide range of intracellular, cell-cell, and cell-matrix constituents including titin, desmin, ␣-actinin, collagen, microtubules as well as by myofilaments.21,23,54 Myofilament stiffness in the adult myocardium is therefore determined by a large set of cytoskeletal components with a high degree of organization, which may minimize the effect of a change in one component, eg, microtubule content, on the measured stiffness of cellular preparations from hypertrophied myocardium.21,35,51 However, the embryonic myocardium contains a significantly lower content of organized collagen and a lower order of cytoskeletal organization,1,55 perhaps explaining the increase in passive stiffness associated with increased microtubule content in LAL myocardium.56 358 Circulation Research August 23, 2002 Downloaded from http://circres.ahajournals.org/ by guest on August 12, 2017 Cardiac morphogenesis occurs coincident with rapid cardiomyocyte clonal expansion.5,57 The compact myocardium is a major source for dividing cardiomyocytes. Cell division appears to cease as immature myocytes are recruited to form mature trabeculae containing mature myocytes and Purkinje cells.58 Confocal images showed that microtubules colocalized with f-actin in the compact layer of LAL embryos and that the degree of myofilament organization appeared to be accelerated in both the compact and trabecular layers in LAL embryos versus controls. In addition to their critical role regulating actin filament distribution during cell division, microtubules have been shown to function as a temporary scaffold to organize cellular components at early developmental stages.47 A lattice of actin filaments and microtubules has been shown to permit the aggregation of myosin filaments in vitro.59 Sedmera et al57 recently showed that cell proliferation was reduced in the LV after LAL. Further experiments are needed to determine if the reduction in LV mechanical load produced by LAL induces a reduction in cell proliferation followed by increased microtubule synthesis and accelerated cell differentiation, or vise versa. Thus, this study is unique in that we have observed an increase in microtubule density and -tubulin protein after reduced mechanical load in the embryonic heart produced by a long-term reduction in mechanical load (LAL) associated with decreased LV filling. Increased microtubule density was associated with changes in both the viscous and elastic components of LV passive properties in LAL chick embryonic myocardium and an acceleration of myofiber maturation. Taken together, these data suggest a role for microtubules in the response of the embryonic myocardium to altered mechanical load. Further research is needed to define the role that microtubules play in translating regional changes in ventricular mechanical load into changes in cardiac structure and function. Acknowledgments This work was supported by an NIH individual NRSA No. F32 HL10200 (E. Schroder, PI) and NIH RO1 HL64626 (B. Keller, PI). The authors would like to thank Jason B. Garrison for his technical assistance. References 1. Clark EB, Hu N, Dummett JL, Vandekieft GK, Olson C, Tomanek R. Ventricular function and morphology in chick embryo from stages 18 to 29. Am J Physiol. 1986;250:H407–H413. 2. Keller BB. Function and biomechanics of developing cardiovascular systems. In: Tomanek RJ, Runyan RB, eds. Formation of the Heart and Its Regulation. Boston, Mass: Birkhauser; 2001:251–272. 3. Nakazawa M, Miyagawa S, Ohno T, Miura S, Takao A. Developmental hemodynamic changes in rat embryos at 11 to 15 days of gestation: normal data of blood pressure and the effect of caffeine compared to data from chick embryo. Pediatr Res. 1988;23:200 –205. 4. Keller BB. Embryonic cardiovascular function, coupling and maturation: a species view. In: Burggren WW, Keller BB, eds. Development of Cardiovascular Systems. Cambridge, Mass: University Press; 1998: 65– 87. 5. Mikawa T, Borisov A, Brown AM, Fischman DA. Clonal analysis of cardiac morphogenesis in the chicken embryo using a replicationdefective retrovirus, I: formation of the ventricular myocardium. Dev Dyn. 1995;193:11–23. 6. Benson DW. Advances in cardiovascular genetics and embryology: role of transcription factors in congenital heart disease. Curr Opin Pediatr. 2000;12:497–500. 7. Eldadah ZA, Hamosh A, Biery NJ, Montgomery RA, Duke M, Elkins R, Dietz HC. Familial Tetralogy of Fallot caused by mutation in the jagged1 gene. Hum Mol Genet. 2001;10:163–169. 8. Gelb BD. Genetic basis of syndromes associated with congenital heart disease. Curr Opin Cardiol. 2001;16:188 –194. 9. Clark EB, Hu N, Frommelt P, Vandekieft GK, Dummett JL, Tomanek RJ. Effect of increased pressure on ventricular growth in stage 21 chick embryos. Am J Physiol. 1989;257:H55–H61. 10. Sedmera D, Pexieder T, Rychterova V, Hu N, Clark EB. Remodeling of chick embryonic ventricular myoarchitecture under experimentally changed loading conditions. Anat Rec. 1999;254:238 –252. 11. Tobita K, Keller BB. Right and left ventricular wall deformation patterns in normal and left heart hypoplasia chick embryos. Am J Physiol. 2000; 279:H959 –H969. 12. Keller BB, Tinney JP, Hu N. Embryonic ventricular diastolic and systolic pressure-volume relations. Cardiol Young. 1994;4:19 –27. 13. Keller BB, Yoshigi M, Tinney JP. Ventricular-vascular uncoupling by acute conotruncal occlusion in the stage 21 chick embryo. Am J Physiol. 1997;273:H2861–H2866. 14. Harh JY, Milton PH, Gallen W, Friedberg DZ, Kaplan S. Experimental production of hypoplastic left heart syndrome in the chick embryo. Am J Cardiol. 1973;31:51–56. 15. McCaffrey FM, Sherman FS. Prenatal diagnosis of severe aortic stenosis. Pediatr Cardiol. 1997;18:276 –281. 16. Samson F, Bonnet N, Heimburger M, Rucker-Martin C, Levitsky DO, Mazmanian GM, Mercadier JJ, Serraf A. Left ventricular alterations in a model of fetal left ventricular overload. Pediatr Res. 2000;48:43– 49. 17. Tsutsui H, Tagawa H, Kent RL, McCollam PL, Ishihara K, Nagatsu M, Cooper G. Role of microtubules in contractile dysfunction of hypertrophied cardiocytes. Circulation. 1994;90:533–555. 18. Tagawa H, Koide M, Sato H, Zile MR, Carabello BA, Cooper Gt. Cytoskeletal role in the transition from compensated to decompensated hypertrophy during adult canine left ventricular pressure overloading. Circ Res. 1998;82:751–761. 19. Cooper G, Kent RL, Mann DL. Load induction of cardiac hypertrophy. J Mol Cell Cardiol. 1989;21:11–30. 20. Heling A, Zimmermann R, Kostin S, Maeno Y, Hein S, Devaux B, Bauer E, Klovekorn WP, Schlepper M, Schaper W, Schaper J. Increased expression of cytoskeletal, linkage, and extracellular proteins in failing human myocardium. Circ Res. 2000;86:846 – 853. 21. Zile MR, Richardson K, Cowles MK, Buckley JM, Koide M, Cowles BA, Gharpuray V, Cooper G IV. Constitutive properties of adult mammalian cardiac muscle cells. Circulation. 1998;98:567–579. 22. Walsh RA. Microtubules and pressure-overload hypertrophy. Circ Res. 1997;80:295–296. 23. Collins JF, Pawloski-Dahm C, Davis MG, Ball N, Dorn GWN, Walsh RA. The role of the cytoskeleton in left ventricular pressure overload hypertrophy and failure. J Mol Cell Cardiol. 1996;28:1435–1443. 24. Bailey BA, Dipla K, Li S, Houser SR. Cellular basis of contractile derangements of hypertrophied feline ventricular myocytes. J Mol Cell Cardiol. 1997;29:1823–1835. 25. de Tombe PP. Altered contractile function in heart failure. Cardiovasc Res. 1998;37:367–380. 26. Zile MR, Koide M, Sato H, Ishiguro Y, Conrad CH, Buckley JM, Morgan JP, Cooper G IV. Role of microtubules in the contractile dysfunction of hypertrophied myocardium. J Am Col Cardiol. 1999;33:250 –260. 27. Tagawa H, Wang N, Narishige T, Ingber DE, Zile MR, Cooper G IV. Cytoskeletal mechanics in pressure-overload cardiac hypertrophy. Circ Res. 1997;80:281–289. 28. Hatcher CJ, Godt RE, Nosek TM. Excessive microtubules are not responsible for depressed force per cross-bridge in cardiac neuralcrest–ablated embryonic chick hearts. Pflügers Arch. 1999;438:307–313. 29. Hamburger V, Hamilton HL. A series of normal stages in the development of the chick embryo. J Morphol. 1951;88:49 –92. 30. Sedmera D, Pexieder T, Hu N, Clark EB. Developmental changes in the myocardial architecture of the chick. Anat Rec. 1997;248:421– 432. 31. Tobita K, Schroder EA, Tinney JP, Garrison JB, Keller BB. Regional passive ventricular stress-strain relations during development of altered loads in the chick embryo. Am J Physiol. 2002;282:H2386 –H2396. 32. Kitabatake A, Suga H. Diastolic stress-strain relation of nonexcised blood-perfused canine papillary muscle. Am J Physiol. 1978;234: H416 –H420. 33. Taber LA, Sun H, Clark EB, Keller BB. Epicardial strains in embryonic chick ventricle at stages 16 through 24. Circ Res. 1994;75:896 –903. Schroder et al Downloaded from http://circres.ahajournals.org/ by guest on August 12, 2017 34. Miller CE, Vanni MA, Keller BB. Characterization of passive embryonic myocardium by quasi-linear viscoelasticity theory. J Biomech. 1997;30: 985–988. 35. Yamamoto S, Tsutsui H, Takahashi M, Ishibashi Y, Tagawa H, ImanakaYoshida K, Saeki Y, Takeshita A. Role of microtubules in the viscoelastic properties of isolated cardiac muscle. J Mol Cell Cardiol. 1998;30: 1841–1853. 36. Nakagawa M, Price RL, Chintanawonges C, Simpson DG, Horacek MJ, Borg TK, Terracio L. Analysis of heart development in cultured rat embryos. J Mol Cell Cardiol. 1997;29:369 –379. 37. Sedmera D, Pexieder T, Hu N, Clark EB. A quantitative study of the ventricular myoarchitecture in the stage 21–29 chick embryo following decreased loading. Eur J Morphol. 1998;36:105–119. 38. Hogers B, DeRuiter MAC, Gittenberger-de Groot AC, Poelmann RE. Unilateral vitelline vein ligation alters intracardiac blood flow patterns and morphogenesis in the chick embryo. Circ Res. 1997;80:473– 481. 39. Kirby ML, Turnage KL III, Hays BM. Characterization of conotruncal malformations following ablation of “cardiac” neural crest. Anat Rec. 1985;213:87–93. 40. Tomita H, Connuck DM, Leatherbury L, Kirby ML. Relation of early hemodynamic changes to final cardiac phenotype and survival after neural crest ablation in chick embryos. Circulation. 1991;84:1289 –1295. 41. Hu N, Connuck DM, Keller BB, Clark EB. Diastolic filling characteristics in the stage 12 to 27 chick embryo ventricle. Pediatr Res. 1991; 29:334 –337. 42. Kent RL, Uboh CE, Thompson EW, Gordon SS, Marino TA, Hoober JK, Cooper G IV. Biochemical and structural correlates in unloaded and reloaded cat myocardium. J Mol Cell Cardiol. 1985;17:153–165. 43. Dipla K, Mattiello JA, Jeevanandam V, Houser SR, Margulies KB. Myocyte recovery after mechanical circulatory support in humans with end-stage heart failure. Circulation. 1998;97:2316 –2322. 44. Rothen-Rutishauser BM, Ehler E, Perriard E, Messerli JM, Perriard J-C. Different behaviour of the non-sarcomeric cytoskeleton in neonatal and adult rat cardiomyocytes. J Mol Cell Cardiol. 1998;30:19 –31. 45. Rappaport L, Samuel JL, Bertier B, Bugaisky L, Marotte F, Mercadier A, Schwartz K. Isomyosins, microtubules and desmin during the onset of cardiac hypertrophy in the rat. Eur Heart J. 1984;5:243–250. Microtubules in Embryonic Heart 359 46. Sato H, Nagai T, Kuppuswamy D, Narishige T, Koide M, Menick DR, Cooper G IV. Microtubule stabilization in pressure overload cardiac hypertrophy. J Cell Biol. 1997;139:963–973. 47. Rappaport L, Samuel JL. Microtubules in cardiac myocytes. Int Rev Cytol. 1988;113:101–143. 48. Watkins SC, Samuel JL, Marotte F, Bertier-Savalle B, Rappaport L. Microtubules and desmin filaments during onset of heart hypertrophy in rat: a double immunoelectron microscope study. Circ Res. 1987;60: 327–336. 49. Pinto JG, Fung YC. Mechanical properties of the heart muscle in the passive state. J Biomech. 1973;6:617– 630. 50. Weisfeldt ML, Loweven WA, Shock NW. Resting and active mechanical properties of trabeculae carneae from aged male rats. Am J Physiol. 1971;220:1921–1927. 51. Kato S, Koide M, Cooper Gt, Zile MR. Effects of pressure- or volumeoverload hypertrophy on passive stiffness in isolated adult cardiac muscle cells. Am J Physiol. 1996;271:H2575–H2583. 52. Brady AJ. Mechanical properties of isolated cardiac myocytes. Physiol Rev. 1991;71:413– 428. 53. Covell J. Factors influencing diastolic function: possible role of the extracellular matrix. Circulation. 1990;81:I155–I158. 54. Granzier HL, Irving TC. Passive tension in cardiac muscle: contribution of collagen, titin, microtubules, and intermediate filaments. Biophys J. 1995;68:1027–1044. 55. Terracio L, Rubin K, Gullberg D, Balog E, Carver W, Jyring R, Borg TK. Expression of collagen binding integrins during cardiac development and hypertrophy. Circ Res. 1991;68:734 –744. 56. Borg TK, Ranson WF, Moslehy FA, Caulfield JB. Structural basis of ventricular stiffness. Lab Inv. 1981;44:49 –54. 57. Sedmera D, Hu N, Weiss K, Keller B, Denslow S, Thompson R. Cellular changes in experimental left heart hypoplasia. Anat Rec. 2002;267: 137–145. 58. Sedmera D, Pexieder T, Vuillemin M, Thompson RP, Anderson RH. Developmental patterning of the myocardium. Anat Rec. 2000;258: 319 –337. 59. Pollard TD, Selden SC, Maupin P. Interaction of actin filaments with microtubules. J Cell Biol. 1984;99:33s–37s. Downloaded from http://circres.ahajournals.org/ by guest on August 12, 2017 Microtubule Involvement in the Adaptation to Altered Mechanical Load in Developing Chick Myocardium Elizabeth A. Schroder, Kimimasa Tobita, Joseph P. Tinney, Jane K. Foldes and Bradley B. Keller Circ Res. 2002;91:353-359; originally published online July 18, 2002; doi: 10.1161/01.RES.0000030179.78135.FA Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2002 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/91/4/353 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/