Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
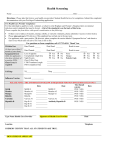
Date: _dd_/_mm__/_yyyy__ MTRH - ANTENATAL CARE INITIAL ENCOUNTER FORM (ANC1) Names: (First, Middle, Surname) MTRH No/AMRS ID: Marital Status: Single Married Divorced Widowed Separated DOB: dd /mm / yyyy OR Age:____yrs District: Location/Sub-location: Village/Estate: Phone No: Partner’s Phone No.: Education Level: None Primary Secondary College University Partner’s name: Occupation: Partner’s occupation Partner’s Age:____yrs 1. Menstrual & Contraceptive history L.N.M.P date___/___/____ EDD: __/___/____ 2. Past Obstetrical history 2. Contraception used (most recent): None Natural IUD Progestin pills Traditional Condoms Implants Depo-Provera Combined hormone pills Gravida:_______ Parity: ________+_________ Gestation at Location D.O.D Outcome: delivery/ (Home or dd/mm/yy (Live/still-births, Miscarriage Health yy ectopic, e.t.c) (mos) Facility) 3. Had Ultrasound this pregnancy? Yes No Sex Length Mode of Birth of of labor delivery (SVD, weight child (hrs) VAC, CS) (kg) (M,F) Complications (maternal, fetal, child) 5. Current pregnancy history (Check each case); REFER TO CONSULTANT IF YES Excessive Nausea and Vomiting Y N Abnormal Vaginal discharge Y N Severe Headache Y N Vaginal bleeding Y N Severe Swelling of hands/face Y N Uterine contractions Y N Fever Y N Foetal movements: Adequate Reduced Absent Dysuria: Y N Cough: Y N Days Weeks N/A (<20 wks) Months Genital ulcers Y N Night sweats: Y N Days Weeks Months 6. Medical history for woman (If Yes, complete ‘Comment’) Thyroid Y N Abnormal PAP smear Y N History of blood transfusion Y N Diabetes Y N Thromboembolic disease / blood clots Y N Congenital anomalies in newborns Y N Hypertension/ High BP Y N Urinary tract infections (UTI) Y N Anemia Y N Yellowness of eyes Y N Seizure disorder Y N Breast disorder Y N Heart disease Y N Problems with anesthesia Y N Drug allergies Y N Asthma Y N Multiple preg. in maternal family Y N Hospitalizations Y N Comment / Others………………………………………………………………………………………………………………………………. ……………………………………………………………………………………………………………………………………………………. History of Infectious Diseases (If Yes to Hx of STD, tick all that apply) Cervicitis, non specific PID GUD Genital warts 7. Hx. Sexually Transmitted Diseases. Yes No Gonorrhea Herpes Syphilis Chlamydia Trichomonas 8. Tuberculosis: Yes No 9. Medications (Please indicate all medications the patient is taking, tick all that apply) None Vitamins Iron/ Fe Folate ARV’s Malaria prophylaxis Cotrimoxazole/ Septrin Other (Specify) MTRH – Antenatal Care Initial Encounter Form. Version 2.2 15th Aug 2011 Psychosocial history 10. Barriers to proper health care Yes No If Yes, tick all that apply Housing/ shelter Communication Transportation Child care Money/ finances Work commitments Unplanned pregnancy Other…………………………………………….. Spouse / family 11. History of postpartum depression or other mental health problems? Yes No 12. Substance use? Alcohol Y N Cigarettes Khat (miraa) Y N Aerosol/ glue 13. Patient education Checklist (Tick when completed) Weight gain / Nutrition Mode of delivery Contraception Sexual activity Use of medications Work Birth plan 14. Do you know when the baby will be born? 16.Indicate preferred infant feeding option Y Y N N Cannabis (bhangi) Intravenous (IV) Signs of labor Fetal movement Y Y N N PROM/ APH Infant feeding 15. Preferred mode of delivery SVD Elective CS Yes No Exclusive breast feeding Expressed breast milk Formula Animal milk 17. Who will be present for social support during delivery? Husband/ Partner Sibling Parents Parents in-law Grandmother Children Other…………………………………………… 18. Will you deliver at a health facility? If No, why? Yes No If Yes, Where? MTRH Other………. ………………….. Lack of transport Culture Family Health worker’s attitude Cost Other……………………… 19. Do you have emergency transport plan? Yes No Yes No 20. Do you have insurance or NHIF? 21. Physical examination Head / Neck Temp:________ HR:___________ BP _______/_______ Normal Abnormal (See comment) Wt:________(Kgs) Ht:_____ ____(cm) CVS (Cardiac) Normal Pallor Normal General Abnormal (See comment) Jaundice Oedema Lymphadenopathy Breast exam RS (Respiratory) Normal Mastitis Normal Abnormal (See comment) Cracked nipples Lump Other Genital exam Normal Ulcer Not done Comment: Vaginal discharge Warts FGM Uterus: Presentation: Cephalic Other Fundal ht: ________cm Fetal HR:_________bpm Specify…………………………………………………………………….. 22. Results of TODAY’S Laboratory Testing; Urine Screen: Protein Nil + ++ +++ Glucose Nil + ++ +++ Leukocytes Nil + ++ +++ Blood group/ABO : A Hemoglobin:_________g/dL B AB O Syphilis/ VDRL: Pos Neg Random blood sugar: _______mmol/L 23. Counselled on HIV: Yes No N/A 24. Tested for HIV: Yes No Antibody screen: Pos Neg PBS for MPS: Pos Neg HIV results: Pos Neg Other:…………………………………………………………………………………………………………………………… 25. Drugs prescribed/given this visit Dose Frequency Duration Picked up 1. Cotrimoxazole 2. Fe Supplement 3. Folic Acid 4. 5. 6. 7. 8. 26. Rh Pos Neg Out of Stock If Neg, Indirect Coomb’s Test (ICT) at 28 weeks If Neg.(ICT), Anti-D Rh IgG given at 28 weeks 27. TT given to date: Non TT1 TT2 TT3 TT4 TT5 TT Given today: Yes No Referrals TT Complete: Yes No Referrals: None Obstetric consultant Pos Neg. N/A <28 wks Yes No 28. IPT1: Yes No IPT2: Yes No 29. Insecticide Treated Net Yes No Social Work Nutritionist AMPATH Other: ___________________________________ Reason for Referral________________________________________ Return to Clinic: Date:_______/________/__________ Provider:_________________________ Signature:______________________ Provider #:_________________ MTRH – Antenatal Care Initial Encounter Form. Version 2.2 15th Aug 2011 MTRH – Antenatal Care Initial Encounter Form. Version 2.2 15th Aug 2011