Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Surround optical-fiber immunoassay wikipedia , lookup
Marburg virus disease wikipedia , lookup
Henipavirus wikipedia , lookup
Hepatitis B wikipedia , lookup
Herpes simplex virus wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Antiviral drug wikipedia , lookup
Oesophagostomum wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
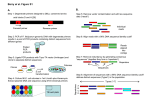
RESEARCH LETTERS paediatricians. When we compared the computerised notes with the cases notified to the coordinating centre, the reporting was complete. We could not assess, however, how many ADRs were not reported. This system, therefore, lacks specificity and reported ADRs should be checked to confirm the relation with drug administration. In paediatric wards, most drugs are prescribed off-label,4 but there are no data on whether this approach is common to primary care. Although in our study no drug was unlicensed or prescribed off-label, our system could address this issue. Concerns have been raised that with our reporting system many trivial ADRs may be reported, which might make detection of important reactions difficult. Continuation of the study will give us information to reassess the reporting criteria for all reactions and drugs. 1 2 3 4 Bonati M, Choonara I, Hoppu K, Pons G, Seyberth H. Closing the gap in drug therapy. Lancet 1999; 353: 1625. Impicciatore P, Pandolfini C, Bosetti C, Bonati M. Reazioni avverse da farmaci in età pediatrica. Ital J Clin Pharmacol 1998; 12: 29–35. Sutcliffe AG. Prescribing medicines for children. BMJ 1999; 319: 70–77. Conroy S, Choonara I, Impicciatore P, et al. Survey of unlicensed and off label drug use in paediatric wards in European countries. BMJ 2000; 320: 79–82. Department of Epidemiology and Biostatistics, Istituto Superiore di Sanità, Viele Regina Elena 299, 00161 Rome, Italy (F Menniti-Ippolito MSc, R Raschetti MSc, R Da Cas MSc); Department of Paediatrics, University of Padova, Padova, Italy (C Giaquinto MD); and Family Paediatrician, “Pedianet project”, Padova, Italy (L Cantarutti MD) Correspondence to: Ms Francesca Menniti-Ippolito (e-mail: [email protected]) Detection of West Nile virus sequences in cerebrospinal fluid Thomas Briese, William G Glass, W Ian Lipkin We have established a sensitive and specific real-time PCR method for detection of West Nile virus. Analysis of specimens obtained during the 1999 New York outbreak indicated the presence of viral sequences in cerebrospinal fluid of all of four individuals with fatal outcomes, and in only one of four who survived. Empirical antiherpesvirus therapy has reduced the morbidity and mortality of encephalitis; however, the advent of potent antiviral drugs with different targets, such as enteroviruses, mandates a new focus on rapid pathogen identification. PCR methods are widely used for detection of herpesviruses and enteroviruses in cerebrospinal fluid (CSF).1 At present, diagnosis of infection with West Nile virus (WNV), an emerging flavivirus recently implicated in outbreaks of fatal encephalitis in Europe, Asia, and North America,2 is based on serology, virus isolation and identification, or molecular analysis of brain materials in a few reference laboratories. Thus, there is no opportunity for early intervention with antiviral therapy. Real-time PCR is a method whereby the presence of a target sequence is detected by continuous measurement of a fluorescent dye label generated during the course of amplification.3,4 Nested PCR is similar in sensitivity to realtime PCR; however, the latter is quantitative over a wide dynamic range, readily adapted to high throughput in a clinical laboratory, and less sensitive to false positive results because assays are done in a closed system. We established a reverse transcription real-time 5⬘ nuclease PCR assay for WNV NY1999 using an ABI Prism 7700 Sequence Detector (PE-Biosystems, Foster City, CA, USA) and two 1614 Sample code Patient number Days after (outcome) onset Serology (IgM-EIA)* A B C D E F G H I J K L M N O P Q R 1 (F) 1 (F) 1 (F) 2 (F) 3 (F) 4 (F) 5 (NF) 6 (NF) 7 (NF) 8 (NF) Control Control Control Control Control Control Control Control 16·68† nd nd 15·36 12·66 12·15 15·42 5·11 16·89 7·06 nd nd nd nd nd nd nd nd 20 nk nk 17 29 24 6 14 2 3 nk nk nk nk nk nk nk nk Molecules/reaction prNS3 prNS5 5⫻103 3⫻104 2⫻104 <100 1·5⫻103 4⫻102 <100 <100 <100 <100 <100 <100 <100 <100 <100 <100 <100 <100 1⫻104 1⫻105 5⫻104 1⫻103 1·5⫻104 7⫻102 6⫻102 <100 <100 <100 <100 <100 <100 <100 <100 <100 <100 <100 F=fatal outcome. NF=non-fatal. nk=not known. nd=not done. *IgM-capture enzyme immunoassay with WNV-Eg101 antigen. †Serological data was obtained for corresponding serum specimen from same date and individual instead of CSF. Reverse transcription 5⬘ nuclease PCR analysis of CSF from New York encephalitis patients primer/fluorescent-probe sets (TIB MOLBIOL, Freehold, NJ, USA). One set was selected in the NS3 gene (set prNS3: fwd, 5⬘-GCA CTG AGA GGA CTG CCC AT; probe, 5⬘-6FAM-TAC CAG ACA TCC GCA GTG CCC AGA-T-TAMRA; rev, 5⬘-TGG GTG AGG GTA GCA TGA CA); the other in the NS5 gene (set prNS5:fwd, 5⬘GCT CCG CTG TCC CTG TGA; probe, 5⬘-6FAMTGG GTC CCT ACC GGA AGA ACC ACG T-TTAMRA; rev, 5-CAC TCT CCT CCT GCA TGG ATG). Sensitivity of the assays for detection of NS3 or NS5 was 50–100 molecules with synthetic RNA transcripts corresponding to nucleotides 4966–5438 and 9915–10082 of the WNV-NY1999 genome (hNY1999; GenBank Acc No AF202541), respectively. Analysis of RNA extracted from serially diluted virus-tissue culture seed showed a linear dynamic range of more than five orders of magnitude with a threshold below ten plaque-forming units. Specificity for WNV-NY1999 was confirmed by NS3 and NS5 sequences of St Louis encephalitis virus, the other flavivirus of the Japanese encephalitis antigenic complex associated with human disease in North America. 18 coded CSF specimens were obtained from the New York State Department of Health for blinded analyses. Ten samples were from individuals with confirmed WNVNY1999 infection;5 eight had neurological disease not due to WNV. One third of the RNA extracted from individual 250 L samples was reverse transcribed and analysed in duplicate by real-time 5⬘ nuclease PCR. Seven of ten samples from individuals with confirmed WNV-NY1999 infection (including three samples obtained at different times from one individual) were positive for NS5 sequences; five of these were also positive for NS3 sequences (table). Three of the serologically confirmed cases were negative by PCR for either gene sequence. Whereas four of five individuals positive for WNV sequences had fatal outcomes; the three negative by PCR survived. The one surviving individual with detectable WNV sequences in CSF (patient 5, table) was a 16-yearold male, the youngest patient with severe disease reported during the outbreak (age of the other cases ranged from 54 to 87 years). No WNV sequences were detected in controls. No correlation was found between PCR results and either the duration of illness at the time of lumbar puncture or the presence of antibody in CSF by IgMcapture enzyme immunoassay (table) or in sera by plaquereduction neutralising antibody assay (data not shown). Serum samples from 24 confirmed cases and ten controls THE LANCET • Vol 355 • May 6, 2000 RESEARCH LETTERS obtained from the New York State Department of Health were extracted and tested for the presence of WNVNY1999 sequences by real-time 5⬘ nuclease PCR. Five of the serologically confirmed cases and none of the controls were positive for WNV-NY1999 sequences (NS3, 3/5 patients; NS5, 5/5 patients; samples obtained 9–16 days after onset of illness). Although it was not possible to analyse matched sets of CSF and sera for all patients, one of the individuals negative by real-time PCR of CSF was positive by PCR for NS5 sequences in serum. The establishment of a real-time PCR method for detection of WNV sequences in human CSF improves diagnosis of viral encephalitides. Although CSF containing WNVs other than WNV-NY1999 were not available for analysis, the primer/probe sets described here are predicted to detect lineage I WNVs, viruses associated with outbreaks of acute illness. Our results suggest that the detection of WNV-NY1999 sequences in CSF correlates with a poor prognosis particularly in older individuals. Further investigation is needed to find whether this correlation can be extended to other flavivirus encephalitides. As antiviral research identifies drugs with activity against WNV, the ability to rapidly implicate this virus is anticipated to achieve clinical importance similar to that associated with herpesviral or enteroviral diseases. We are grateful to Leo Grady, Cinnia Huang, and Susan Wong of the New York State Department of Health for providing CSF and serum samples, Rob Lanciotti and John Roehrig from the Division of VectorBorne Infectious Diseases, CDC, for WNV extracts, and clinical and serological results, and Charles Calisher and Ingo Jordan for helpful discussions. 1 2 3 4 5 Jeffery KJM, Read SJ, Peto TEA, Mayon-White RT, Bangham RM. Diagnosis of viral infections of the central nervous system: clinical interpretation of PCR results. Lancet 1997; 349: 313–17. Asnis D, Conetta R, Waldmon G, et al. Outbreak of West Nile-like viral encephalitis: New York 1999. MMWR Morb Mortal Wkly Rep 1999; 48: 845–49. Higuchi R, Fockler C, Dollinger G, Watson R. Kinetic PCR analysis: real-time monitoring of DNA amplification reactions. Bio/Technology 1993; 11: 1026–30. Lee LG, Connell CR, Bloch W. Allelic discrimination by nicktranslation PCR with fluorogenic probes. Nucleic Acids Res 1993; 21: 3761–66. CDC. Case definitions for infectious conditions under public health surveillance. MMWR Morb Mortal Wkly Rep 1997; 46: 1–55. Emerging Diseases Laboratory, Departments of Neurology, Microbiology and Molecular Genetics, Anatomy, and Neurobiology, University of California, Irvine, CA 92697-4292, USA (T Briese PhD, W G Glass BS, Prof W I Lipkin MD) Correspondence to: Dr T Briese (e-mail: [email protected]) Pharmacogenetic prediction of clozapine response M J Arranz, J Munro, J Birkett, A Bolonna, D Mancama, M Sodhi, K P Lesch, J F W Meyer, P Sham, D A Collier, R M Murray, R W Kerwin We did association studies in multiple candidate genes to find the combination of polymorphisms that give the best predictive value of response to clozapine in schizophrenic patients. A combination of six polymorphisms in neurotransmitter-receptorrelated genes resulted in 76·7% success in the prediction of clozapine response (p=0·0001) and a sensitivity of 95% (±0·04) for satisfactory response. These results will form the basis for a simple test to enhance the usefulness of clozapine in psychiatric treatment. The atypical antipsychotic clozapine was reintroduced into the UK and USA in 1990, following the demonstration of THE LANCET • Vol 355 • May 6, 2000 Gene Polymorphism Detection method (restriction enzymes/ electrophoresis conditions) Adrenergic receptors ␣2A ␣2A ␣1A ⫺1291–C/G ⫺261–G/A Arg492Cys MspI/10% PAGE HhaI/10% PAGE PstI/3% agarose Dopamine receptor D3 Ser9Gly MscI/3% agarose Serotonin receptors 5–HT2A 5–HT2A 5–HT2A 5–HT2A 5–HT2A 5–HT2C 5–HT2C 5–HT3A 5–HT3A 5–HT5A 5–HT5A ⫺1438–G/A 102–T/C 516–C/T His452Tyr Thr25Asp Cys23Ser ⫺330–GT/⫺244–CT repeat 178–C/T 1596–G/A 12–A/T ⫺19–G/C MspI/2% agarose MspI/2% agarose Sau96I/2% agarose BbvI/3% agarose BstNI/2% agarose HinfI/4% agarose 10% PAGE 10% PAGE/5% glycerol NheI/3% agarose BsrI/2% agarose BsaJI/10% PAGE Serotonin transporters Transporter 5–HTT VNTR Transporter promoter 5–HTT 5–HTTLPR 4% agarose 4% agarose Histamine H1 H2 BsmI/10% PAGE HaeIII/10% PAGE Leu449Ser ⫺1018–G/A PAGE=Polyacrylamidegel electrophoresis. Table 1: List of polymorphisms studied and detection methods for the identification of the alleles superior efficacy and tolerability in severely treatment-resistant patients.1 Since then a range of well-tolerated atypical antipsychotics have been introduced.2 Although the evidence base for the use of these drugs is compelling, various reasons seem to prevent use in greater numbers of eligible patients. The treatment costs are greater than with classic antipsychotics and the response to these drugs is heterogeneous, with between 30% and 60% responding to clozapine, the archetypal atypical antipsychotic. We have attempted to explore new targets by studying pharmacogenetic associations in a large number of patients treated with clozapine. We have previously shown that allelic variation in the serotonin neurotransmitter receptor 2A gene (5–HT2A) is a factor in determining clinical response to clozapine.3,4 However, 5–HT2A polymorphisms on their own cannot fully explain the variability seen in treatment response, and it has been postulated that there are contributions from other mutations in neurotransmitter-receptor-related genes. We did association studies in multiple candidate genes to find the combination of polymorphisms that give the best Polymorphism p for genotype p for allele ⫺1291–C/G (ADR2A) ⫺261–G/A (ADR2A) Arg492Cys (ADR1A) Ser9Gly (D3) Leu449Ser (H1) ⫺1010–G/A (H2) His452Tyr (5–HT2A) Thr25ASP (5–HT2A) ⫺1438–G/A (5–HT2A) 102–T/C (5–HT2A) 516–C/T (5–HT2A) ⫺330–GT/⫺244–CT (5–HT2C) Cys23Ser (5–HT2C) 178–C/T (5–HT3A) 1596–G/A (5–HT3A) ⫺12–A/T (5–HT5A) ⫺19–G/C (5–HT5A) 5–HTTLPR VNTR (5–HTT) 0·85 0·54 0·22 0·89 0·30 0·08 0·01* 0·57 <0·001 <0·001 0·65 0·04† 0·08‡ 0·92 0·98 0·20 0·55 0·04 0·89 0·61 0·40 0·10 0·63 0·35 0·43 0·02 0·78 0·001 0·001 0·82 0·31 0·17 0·79 0·85 0·09 0·35 0·36 0·70 *Try recessive: 0·004. †Short allele dominant. ‡Ser23 dominant. Table 2: Comparison of responders vs non-responders for the 19 polymorphisms genotyped 1615