Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
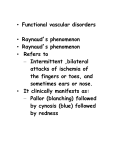
CLINICAL APPROACHES TO SECONDARY HYPERTENSION DEFINITION • Essential, primary, or idiopathic hypertension is defined as high BP in which secondary causes or mendelian (monogenic) forms are not present • High BP – repeatedly measured BP exceeding 140/90 mmHg, i.e. a systolic BP above 140 and/or diastolic BP above 90 Aetiology of Hypertension • Primary – 90-95% of cases – also termed “essential” of “idiopathic” • Secondary – about 5% of cases – Renal or renovascular disease – Endocrine disease • • • • Phaeochomocytoma Cushings syndrome Conn’s syndrome Acromegaly and hypothyroidism – Coarctation of the aorta – Iatrogenic • Hormonal / oral contraceptive • NSAIDs Aetiology of Hypertension • Primary – 90-95% of cases – also termed “essential” of “idiopathic” • Secondary – about 5% of cases – Renal parenchymal (2-5%) or renovascular disease – Endocrine disease • • • • Phaeochomocytoma Cushing syndrome Conn syndrome Acromegaly and hypothyroidism – Coarctation of the aorta – Iatrogenic • Hormonal / oral contraceptive • NSAIDs Renal parenchymal disease • • • • • • • • Acute and chronic glomerulonephritis Polycystic kidney disease Diabetic nephropathy Pyelonephritis Obstructive uropathy Neoplasms Renal trauma Radiation nephritis Hypertension in parenchymal renal disease: CONCLUSIONS • Hypertension may result from renal disease that reduces functioning nephrons; • Evidence shows a clear relationship between high blood pressure and end-stage renal disease; • BP should be controlled to 130/85 mmHg (125/75 mmHg in patients with proteinuria in excess of 1g/24 h) Aetiology of Hypertension • Primary – 90-95% of cases – also termed “essential” of “idiopathic” • Secondary – about 5% of cases – Renal parenchymal or renovascular disease (0.3-3%) – Endocrine disease • • • • Phaeochomocytoma Cushings syndrome Conn’s syndrome Acromegaly and hypothyroidism – Coarctation of the aorta – Iatrogenic • Hormonal / oral contraceptive • NSAIDs RENAL ARTERY STENOSIS (RAS) • Atherosclerotic RAS (>90% of cases): involves the ostium and the proximal portion of the main renal artery with plaque extending into the perirenal aorta • Fibromuscular dysplasia (10% of cases): typically seen in young and middle-aged females. As opposed to atherosclerotic RAS, fibromuscular dysplasia typically affects the distal two thirds of the main renal artery RENAL ARTERY STENOSIS: screening and diagnostic studies Renal duplex sonography Magnetic resonance angiography Renal artery arteriography Captopril renography RENAL ARTERY STENOSIS: treatment • BP control • Antiplatelet, lipid-lowering therapy, and beta-blockers, if appropriate • No ACE-inhibitors in severe RAS ! RENAL ARTERY STENOSIS: treatment Percutaneous or surgical revascularization, if: ● Resistant or poorly controlled hypertension and unilateral or bilateral renal artery stenosis ● Renal artery stenosis and recurrent flash pulmonary edema for which there is no readily explainable cause ● Chronic renal failure and bilateral renal artery stenosis or renal artery stenosis to a solitary functioning kidney ● Sonographic renal longitudinal length >7cm Aetiology of Hypertension • Primary – 90-95% of cases – also termed “essential” of “idiopathic” • Secondary – about 5% of cases – Renal or renovascular disease – Endocrine disease • Phaeochomocytoma (0.1-0.6 %) • Cushings syndrome • Conn’s syndrome • Acromegaly and hypothyroidism – Coarctation of the aorta – Iatrogenic • Hormonal / oral contraceptive • NSAIDs The left ventricle is markedly thickened in this patient with severe hypertension that was untreated for many years. The myocardial fibers have undergone hypertrophy. This left ventricle is very thickened (slightly over 2 cm in thickness), but the rest of the heart is not greatly enlarged. This is typical for hypertensive heart disease. The hypertension creates a greater pressure load on the heart to induce the hypertrophy. PHEOCHROMOCYTOMA diagnostic techniques • • • • • • Biochemical tests High pressure liquid chromatography: Plasma catecholamines: noradrenaline, adrenaline; Free plasma fractionated metanephrines: normetanephrine, metanephrine; Urinary catecholamines (24h) Urinary fractionated metanephrines (24h) Spectrophotometry: Total metanephrines (24h urine); Vanillylmandelic acid (24h urine) PHEOCHROMOCYTOMA imaging techniques • Duplex sonography; • Magnetic resonance imaging (MRI); • Computed romography (CT); • 123I – meta-iodo-benzyl-guanidine scanning (123I-MIBG) PHEOCHROMOCYTOMA: laparoscopic removal Preoperative Management (10-14 days) Purpose: to prevent catecholamine induced, serious, and potentially life-threatening complications during surgery, including hypertensive crises, cardiac arrhythmias, pulmonary oedema, and cardiac ischemia; BP should be reduced to below 160/90 mm Hg for at least 24h; orthostatic hypotension should be present, but blood pressure in the upright position should not fall below 80/45 mm Hg; there should be no more than one ventricular extrasystole every 5 min; and the electrocardiogram should show no S-T segment changes and T-wave inversions for 1 week; PHEOCHROMOCYTOMA: Management • Phenoxybenzamine, a long acting alpha-adrenergic blocker, is the mainstay of medical treatment to control BP. A total dose of 1 mg/kg is sufficient in most patients. • An alpha-blocker Doxazosin in increasing doses from 1 to 16 mg once a day. •A beta-adrenoceptor blocker (eg,propranolol 40 mg three times daily or atenolol 25–50 mg once daily) could be included after several days of alpha-adrenergic blockade. • Adequate salt and fluid intake lowers the risk of orthostatic hypotension. PHEOCHROMOCYTOMA: Management •Should substantial rises in blood pressure still take place during surgery, these can be controlled by bolus or by continuous infusion of phentolamine, sodium nitroprusside, or a shortacting calcium antagonist (eg, nicardipine); • Tachyarrhythmias can be treated by infusion of a shortacting -adrenoceptor blocker (eg, esmolol). Aetiology of Hypertension • Primary – 90-95% of cases – also termed “essential” of “idiopathic” • Secondary – about 5% of cases – Renal or renovascular disease – Endocrine disease • Phaeochomocytoma • Cushings syndrome • Conn’s syndrome (0.3-1%) • Acromegaly and hypothyroidism – Coarctation of the aorta – Iatrogenic • Hormonal / oral contraceptive • NSAIDs Primary Hyperaldosteronism • Screening for hyperaldosteronism should include plasma aldosterone and plasma renin activity measured in morning samples • Plasma aldosterone:renin ratio: normally <20; diagnostic cut-off value >30; • Aldosterone excretion rate during salt loading, captopril, or spironolactone test (the captopril test may be less useful in blacks because of the high prevalence of low plasma renin activity) • Adrenal CT, MRI Primary Hyperaldosteronism Should be differentiated from • Secondary hyperaldosteronism in patients with renal failure, CHF, essential hypertension • Monogenic forms of hypertension (pseudohyperaldosteronism): Liddle’s syndrome (autosomal-dominant disorder, characterized by low-renin, low-aldosterone, lowpotassium volume-expanded hypertension) Gordon’s syndrome (autosomal-dominant disorder, characterized by low-renin, low-aldosterone, high-potassium volume-expanded hypertension) Primary Hyperaldosteronism TREATMENT 1. Medical • Spironolactone, a competitive aldosterone antagonist • Amiloride, a potassium-sparing diuretic • Glucocorticoids (in glucocorticoid-remediable form) 2. Surgical, if appropriate Aetiology of Hypertension • Primary – 90-95% of cases – also termed “essential” of “idiopathic” • Secondary – about 5% of cases – Renal or renovascular disease – Endocrine disease • Phaeochomocytoma • Cushing’s syndrome (0.1-0.6%) Conn’s syndrome • Acromegaly and hypothyroidism – Coarctation of the aorta – Iatrogenic • Hormonal / oral contraceptive • NSAIDs Hypothyroidism • Both hypertension (particularly diastolic) and hypotension are common; Hyperthyroidism • Accompanied by systolic hypertension, especially in the elderly; Acromegaly • 25-50% exhibit elevated blood pressure • Coarctation of the Aorta with Dissection • Coarctation of the Aorta Case 1 • A 28-year old female is seen in the emergency department with symptoms of severe periodic headaches, sweating, and nausea with vomiting. She also complains of feeling lightheaded while standing. Her BP on presentation is 240/136, with a HR of 92. On standing, the patient has a BP of 204/98, with a HR of 136. On ophthalmologic examination the patients has mild blurring of the optic discs without hemorrhage. What is the best medication for the management of this patient’s hypertension? Case 1 • What is the best medication for the management of this patient’s hypertension? A. B. C. D. E. Phentolamine Fenoldopam Esmolol Nicardipine Diazoxide Case 1 • What is the best medication for the management of this patient’s hypertension? A. B. C. D. E. Phentolamine – correct answer Fenoldopam Esmolol Nicardipine Diazoxide Case 1 • What test would best determine the patient’s diagnosis? A. Plasma catecholamines B. 24-h urine collection for 5-hydroxyindolacetic acid C. Abdominal CT-scan D. 24-h urine collection for metanephrines and vanillylmandelic acid E. Adrenal vein sampling for renin levels Case 1 • What test would best determine the patient’s diagnosis? A. Plasma catecholamines B. 24-h urine collection for 5-hydroxyindolacetic acid C. Abdominal CT-scan D. 24-h urine collection for metanephrines and vanillylmandelic acid – correct answer E. Adrenal vein sampling for renin levels Case 2 • A 28-year old female has hypertension that is difficult to control. She was diagnosed at age 26. Since that time she has been on increasing amounts of medication. Her current regimen consists of atenolol 50 mg bid, lisinopril 40 mg qd, clonidine 0.1 mg bid, and amlodipine 5mg qd. Physical examination is unremarkable. Laboratory studies reveal a potassium of 2.8 mmol/l. Fasting blood glucose is 5.27 mmol/l. What is the likely diagnosis? Case 2 • What is the likely diagnosis? A. B. C. D. E. Congenital adrenal hyperplasia Fibromuscular dysplasia Cushing’s syndrome Conn’s syndrome Pheochromocytoma Case 2 • What is the likely diagnosis? A. B. C. D. E. Congenital adrenal hyperplasia Fibromuscular dysplasia Cushing’s syndrome Conn’s syndrome – correct answer Pheochromocytoma Case 2 • What is the best way to diagnose the disease? A. B. C. D. E. Renal vein renin levels 24-h urine collection for metanephrines MRI of the renal arteries 24-h urine collection for cortisol Plasma aldosterone/renin ratio Case 2 • What is the best way to diagnose the disease? A. B. C. D. E. Renal vein renin levels 24-h urine collection for metanephrines MRI of the renal arteries 24-h urine collection for cortisol Plasma aldosterone/renin ratio – correct answer Thank you for attention!