Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Meningococcal disease wikipedia , lookup
2015–16 Zika virus epidemic wikipedia , lookup
Leptospirosis wikipedia , lookup
Hepatitis C wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Ebola virus disease wikipedia , lookup
Influenza A virus wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
West Nile fever wikipedia , lookup
Orthohantavirus wikipedia , lookup
Antiviral drug wikipedia , lookup
Henipavirus wikipedia , lookup
Marburg virus disease wikipedia , lookup
Hepatitis B wikipedia , lookup
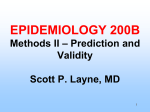
Infectious Laryngotracheitis Virus Olivia Henry | a1210305 Word Count: 1,821 Infectious laryngotracheitis virus (ILTV) is an alphaherpesvirus that causes acute respiratory disease in broilers, pullets and adult chickens worldwide. First described by May and Tittsler in 1925 (Rodriguez-Avila, et al., 2007), this highly contagious virus is economically important as the disease results in serious production losses due to reduced egg production, mortality and delayed growth (Fuchs, et al., 2007; Hidalgo, 2003). Although they were the first poultry vaccines available, modified live ILTV vaccines are used only in cases of severe outbreaks due to the ability of the vaccine strains to establish latent infections and spread to unvaccinated flocks (Bagust, et al., 2000; Hidalgo, 2003; Lee, et al., 2012; Mutalib, 1992; Ou, et al., 2011; Rodriguez-Avila, et al., 2007). Clinical Progression and Pathology Clinical symptoms of ILTV generally appear six to twelve days following natural exposure. General clinical signs that are characteristic for ILTV include nasal discharge and moist rales followed by coughing, gasping, sneezing, conjunctivitis and depression (Bagust, et al., 2000; Hidalgo, 2003). In early ILTV, gross lesions may be observed in the conjunctiva, larynx and trachea and the changes in Figure 1. A trachea of an infected chicken, partially tissue range from mild to severe. The two clogged by blood and mucus (Carver, 2012) recognised forms of ILTV are severe epizootic form and mild enzootic form. (Bagust, et al., 2000) Symptoms associated with severe epizootic forms include mucoid inflammation, difficulty breathing, necrosis in respiratory tissue and expulsion of blood-stained mucus. Haemorrhages and mucus plugs are also visible upon gross examination of the trachea (See Figure 1). Additionally, while morbidity of severe epizootic form is high (90%100%), mortality may be highly variable, ranging between 5% and 70% (Bagust, et al., 2000; Rodriguez-Avila, et al., 2007). Mild enzootic symptoms Figure 2. Immunohistochemical staining displaying the presence of CD4+ and CD8+ T lymphocytes scattered throughout the mucosa, as indicated by arrows (A) and B lymphocytes forming clusters in the mucosa (B) of birds 4 days following inoculation. Bar=100µm (Devlina, et al., 2010) range from excess mucus production to weakness, decreased egg production, eye secretion, conjunctivitis, swelling of infraorbital sinuses, continual nasal discharge and haemorrhagic conjunctivitis (Bagust, et al., 2000; Hidalgo, 2003). Additionally, morbidity and mortality are generally low in mild enzootic form, 5% and 0.1%-2%, respectively. (Bagust, et al., 2000; Hidalgo, 2003) The various stages of ILTV may also be seen in microscopic changes of the respiratory tract. In its early stages, intranuclear inclusion bodies are present in epithelial cells of the trachea, larynx and conjunctiva. The tracheal mucosa will display a loss of goblet cells and an infiltration of inflammatory cells. Cells will lose cilia and become oedematous as the infection progresses. Syncytia form and lymphocytes, histiocytes and plasma cells may be found in the mucosa and submucosa (Figure 2). In late stages, the mucosa is covered by a thin layer of basal cells and possibly lack epithelial cover due to cell destruction and desquamation, which results in the disappearance of the inclusion bodies. Blood vessels also become exposed and rupture (Bagust, et al., 2000; Devlina, et al., 2010; Hidalgo, 2003). Primary disease in infected chickens tends to last between seven and fourteen days, however some extreme cases have been reported to persevere for up to four weeks (Bagust, et al., 2000; Hidalgo, 2003). Virology ILTV exhibits the typical structure of a herpesvirion. An irregular outer envelope bears viral glycoprotein spikes. The Figure 3. Electron microscopy of ILTV replication. Images show assembly of the virion within an LMH cell line (A), the formation of primary envelope at the nuclear membrane (B & C), assembly of tegument and formation of secondary envelope (D & E) and virion release via exocytosis (F & G). Bars = 1µm (A), 150nm (B & C), 500nm (D) and 300nm (E, F & G). envelope contains a tegument layer, a symmetrical icosahedral nucleocapsid and a double- stranded DNA core. The DNA genome consist of a linear 155 kilobase molecule containing unique long and short segments flanked by inverted repeats. The major immunogens of the virus have been reported to be the five glycoproteins of ILTV. These stimulate both the humoral and cell-mediated immune responses (Bagust, et al., 2000; Fenner, et al., 1974; Fuchs, et al., 2007; Hidalgo, 2003). Natural transmission occurs through the upper respiratory and ocular routes after coming into contact with infectious aerosols or discharge. ILTV is not, however, transmissible via the egg (vertically) or to humans through cooked meat from infected chickens (Bagust, et al., 2000; Carver, 2012; Fuchs, et al., 2007; Hidalgo, 2003; Ou, et al., 2011). There are three known sources of ILTV. These are (1) clinically infected fowls, (2) fowls which are latent carriers of ILTV, and (3) fomites contaminated with ILTV, especially that of farm employees (Bagust, et al., 2000; Hidalgo, 2003; Ou, et al., 2011). The upper respiratory tract is the target of ILTV infection and disease. While the tracheal and laryngeal epithelia are always affected, other mucous membranes such as the conjunctiva, respiratory sinuses, air sacs and lung tissue are also at risk. The trachea is the most active site of replication, regardless of exposure and route of transmission. (Bagust, et al., 2000) Upon infection, ILTV attaches to the host cell receptors and its envelope fuses with the host cell plasma membrane. The nucleocapsid is then released into the host cytoplasm, where it is transported to the nuclear membrane. The double-stranded viral DNA is then released from the nucleocapsid and enters the nucleus via nuclear pores. Like other alphaherpesviruses, transcription within the nucleus is tightly regulated and sequential. DNA-binding proteins and enzymes are among some 70 viral encoded proteins produced during this process; however a majority are structural proteins. These structural proteins form the capsid, which forms a package for the viral DNA. Replication of the viral DNA occurs by a rolling circle mechanism. Concatamers are formed and cleaved into monomeric units before being packaged into the capsid. The nucleocapsids are then enveloped and de-enveloped by transportation through the inner and outer leaflets of the nuclear membrane, respectively (Figure 3B & 3C). Within the cytoplasm, nucleocapsids are associated with electron dense tegument and participate in a second budding event, where it is re-enveloped once again in the trans-Golgi region (Figure 3D & 3E). The enveloped virions may be released by cell lysis or vacuolar membrane fusion and exocytosis (Figure 3F & 3G) (Hidalgo, 2003; Fuchs, et al., 2007). As with other herpesviruses, the establishment of latency occurs due to the invasion of nervous tissue (Bagust, et al., 2000; Fenner, 1968). The trigeminal ganglion (TRG) appears to be the main site of latency of the ILTV. The TRG innervates tissue in the upper respiratory tract, the mouth, and the eyes, providing strong evidence of neural migration. During the acute phase of ILTV infection, invasion of the TRG often occurs in both wild and vaccine strains (Bagust, et al., 2000; Hidalgo, 2003). The establishment of latency and the shedding of the infectious virus at low levels provide numerous problems in the poultry industry due to the ability of vaccinated birds to infect unvaccinated birds (Bagust, et al., 2000; Hidalgo, 2003; Lee, et al., 2012; Mutalib, 1992; Ou, et al., 2011; Rodriguez-Avila, et al., 2007). Management As previously mentioned, there are three main sources of ILTV: clinically infected fowls, latent carriers of ILTV, and fomites contaminated with ILTV (Bagust, et al., 2000; Hidalgo, 2003; Ou, et al., 2011). Biosecurity measures and management practises must be strictly enforced in order to prevent or minimise exposure of susceptible chickens to ILTV (Giambrone, et al., 2008). Simple routine and hygiene practises are encouraged and enforced to minimise transmission via fomites, such as clothes and equipment. These practises include covering footwear or wearing specific footwear for various premises to minimise transmission between farms and flocks, and meticulously disinfecting equipment and footwear after use (Carver, 2012). Additionally, it has been found that heating ILTV to 38°C for 48 hours will inactivate the virus, however heating alone is not sufficient in reducing levels of ILTV in practice due to deeply built-up litter (Giambrone, et al., 2008). Giambrone and collegues (2008) recommended a combination of heating litter to 38°C for 24 hours, using commercial poultry litter treatments and in-house composting for five days. This practise was found to be efficient in controlling ILTV outbreaks, reducing incidence and severity of not only ILTV, but also other important viral pathogens (Giambrone, et al., 2008). In the event of an outbreak, vaccinations may limit spread and severity, while also shortening disease duration (Hidalgo, 2003). Due to the fact that ILTV infections predominantly occur in the upper respiratory tract, viraemia is uncommon and the humoral immune response, including maternal IgG and secretory antibodies do not confer resistance to ILTV infection. Additionally, passive transfer of anti-ILTV serum and neutralizing antibodies proved unsuccessful (Hayles, et al., 1975; Hidalgo, 2003; Poulsen, et al., 1998). Therefore it was proposed that viral clearance is primarily mediated by the cell mediated immunity (CMI) and modified live vaccines are likely to provide the best protection against ILTV (Bagust, et al., 2000; Hidalgo, 2003; Poulsen, et al., 1998). There are currently two live-attenuated ILTV vaccines commercially available: those attenuated by sequential passages in tissue culture (tissue culture origin, or TCO vaccines) and those attenuated by multiple passages in embryonating eggs (chicken embryo origin, or CEO vaccines) (Hidalgo, 2003; Lee, et al., 2012; Oldoni, et al., 2009; Mutalib, 1992; RodriguezAvila, et al., 2007; Vagnozzi, et al., 2010). Vaccines may be mass administered using drinking water, spray or sometimes individually as eye drops. While the eye drop procedure is more effective than administration through drinking water, it is highly inefficient for the poultry industry. Therefore the most common method is to vaccinate through drinking water, though the protection of chickens vaccinated in this way may not be ideal as individual dosage cannot be controlled (Hayles, et al., 1976; Hilbink, et al., 1981; Villegas, 1998). CEO vaccines have been found to be more effective than TCO vaccines, due to the fact that TCO vaccines are more attenuated and therefore less immunogenic (Hidalgo, 2003). Other ILTV vaccines include recombinant subunit vaccines and live attenuated recombinant ILT vaccines. Recombinant subunit vaccines are produced by inserting a gene encoding an immunogenic glycoprotein into an avian viral vector. The live attenuated recombinant vaccines are constructed by selecting for homologous recombinant events in vivo. The live-attenuated recombinant vaccine, however, has not been commercially successful for ILTV thus far (Hidalgo, 2003). ILTV vaccines are used sparingly, due to the complications that arise from their use. Vaccination of birds for ILTV results in the occurrence of carrier birds. Bird-to-bird transmission following vaccination may result in a gain of virulence. In the case of CEO, shedding of the virus by carrier birds may cause severe respiratory disease and mortality, while TCO may cause a mild respiratory response (Bagust, et al., 2000; Hidalgo, 2003; Rodriguez-Avila, et al., 2007). This is a serious problem not only within individual poultry farms, but also internationally, as ILTV vaccines raise serious concerns in regard to imports and exports. Within individual poultry farms, producers that mix vaccinated and unvaccinated flocks, or even new flocks vaccinated using different administrations (for example, mass application instead of eye drop administration) may witness an outbreak due to the different levels of protection (Hidalgo, 2003). Internationally, there is concern that importation of live, vaccinated and unvaccinated chickens may result in an outbreak of ILTV, especially when importing from countries with intensive poultry production. Additionally, caution must be exercised when importing eggs and egg crates due to the possibility of the presence of fomites (Hidalgo, 2003). Additionally, the presence of the vaccine in drinking water may remain in the water systems and infect susceptible flocks. Ou and collegues (2011) suggested a series of water treatments should be used in conjunction with other management techniques outlined by Giambrone, et al. in 2008. Ou suggested heating the house to 38°C for 24 hours, treating litter with commercial products, composting litter and ensuring to treat water with multiple sanitizers such as citric acid or sodium hypochlorite. Live-CEO derived vaccines were found to be able to attach to biofilms in drinking water systems and infect susceptible chickens (Ou, et al., 2011). Summary While ILTV is not directly harmful to human health, it is an economically important disease due to its effect on bird mortality, egg production, growth and overall animal well-being. Clinical symptoms are obvious and therefore may be observed and responded to rapidly, halting viral spread in the event of an outbreak. Eradication of ILTV may be possible due to the extremely narrow host range. However, this will be difficult due to latent infections produced by not only the virus, but also the most effective vaccines. Due to its highly contagious nature, transmission of ILTV is a serious issue. However it can be controlled using simple management techniques and biosecurity measures. These measures include separating unvaccinated birds from vaccinated birds, disinfecting equipment, minimizing spread of fomites and adequate litter and water treatments. On a global scale, imports and exports must be monitored to ensure that live birds do not shed ILTV and fomites are not transported to susceptible countries. Further research in this area is required in order to produce vaccines that elicit cell mediated immunity without latency or shedding of the ILTV. References 1. Bagust, T., Jone, R. & Guy, J., 2000. Avian infectious laryngotracheitis. Revue scientifique et technique (International Office of Epizootics), pp. 483-492. 2. Carver, D. K., 2012. Poultry Diseases: Infectious Laryngotracheitis Virus (ILT). [Online] Available at: http://www.ces.ncsu.edu/depts/poulsci/tech_manuals/laryngotracheitis.pdf [Accessed August 2012]. 3. Devlina, J. et al., 2010. Evaluation of immunological responses to a glycoprotein G deficient candidate vaccine strain of infectious laryngotracheitis virus. Vaccine, 5(28), p. 1325– 1332. 4. Fenner, F., 1968. The Biology of Animal Viruses Volume II: The Pathogenesis and Ecology of Viral Infections. 1st ed. New York: Academic Press Inc.. 5. Fenner, F. et al., 1974. The Biology of Animal Viruses. 2nd ed. New York: Academic Press, Inc.. 6. Fuchs, W. et al., 2007. Molecular biology of avian infectious laryngotracheitis virus. Veterinary research (Paris), pp. 261-279. 7. Giambrone, J., Fagbohun, O. & Macklin, K., 2008. Management practices to reduce infectious laryngotracheitis virus in poultry litter. Journal of Applied Poultry Research, pp. 64-68. 8. Hayles, L., Hamilton, D. & Newby, W., 1975. Transfer of parental immunity to infectious laryngotracheitis in chicks. Canadian Journal of Comparative Medicine, pp. 218-219. 9. Hayles, L., Newby, W., Gasperdone, H. & Gilchrist, E., 1976. Immunization of broiler chickens with a commercial infectious laryngotracheitis vaccine in the drinking water. Canadian Journal of Comparative Medicine, pp. 129-134. 10. Hidalgo, H., 2003. Infectious laryngotracheitis: A review. Brazilian Journal of Poultry Science, pp. 157-168. 11. Hilbink, F., Smit, T. & Yadin, H., 1981. Drinking watter vaccination against infectious laryngotracheitis. Canadian Journal of Comparative Medicine, pp. 120-123. 12. Lee, J., Bottje, W. & Kong, B., 2012. Genome-wide host response against infectious laryngotracheitis virus vaccine infection in chicken embryo lung cells. BMC Genomics, p. 143. 13. Lee, S. et al., 2011. First complete genome sequence of infectious laryngotracheitis virus. BMC Genomics, p. 197. 14. Mutalib, A., 1992. Studies on transmissibility of a tissue-culture-modified laryngotracheitis virus. Journal of Veterinary Diagnostic Investigation, pp. 412-415. 15. Oldoni, I. et al., 2009. Pathogenicity and growth characteristics of selected infectious laryngotracheitis virus strains from the United States. Avian Pathology, pp. 47-53. 16. Ou, S., Giambrone, J. & Macklin, K., 2011. Infectious laryngotracheitis vaccine virus detection in water lines and effectiveness of sanitizers for inactivating the virus. Journal of Applied Poultry Research, pp. 223-230. 17. Portz, C. et al., 2008. Natural infection of turkeys by infectious laryngotracheitis virus. Elsevier, pp. 57-64. 18. Poulsen, D., Thureen, D. & Keeler Jr, C., 1998. Comparison of disease susceptibility and resistance in three lines of chickens experimentally infected with infectious laryngotracheitis virus. Poultry Science, pp. 17-21. 19. Rachamadugu, R., Lee, J., Wooming, A. & Kong, B., 2009. Identification and expression analysis of infectious laryngotracheitis virus encoding microRNAs. Virus Genes, pp. 301308. 20. Rodriguez-Avila, A., Oldoni, I., Riblet, S. & Garcia, M., 2007. Replication and transmission of live attenuated infectious laryngotracheitis virus (ILTV) vaccines. Avian Diseases, pp. 905911. 21. Vagnozzi, A., Garcia, M., Riblet, S. M. & Zavala, G., 2010. Protection induced by Infectious Laryngotracheitis Virus vaccines alone and combined with Newcastle Disease Virus and/or Infectious Bronchitis Virus vaccines. Avian Diseases, pp. 1210-1219. 22. Villegas, P., 1998. Viral diseases of the respiratory system. Poultry Science, pp. 1143-1145.