Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Neuropsychopharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Neuropharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Drug interaction wikipedia , lookup
Psychopharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
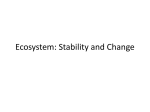
Notice: This manuscript is a version of an article published in Neuroscience and Biobehavioral Reviews v. 24, no. 3 (May 2000) p. 279-294. The published article is available at www.elsevier.com/locate/neubiorev NEUROSCIENCE AND BIOBEHAVIORAL REVIEWS PERGAMON Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 www.elsevier.com/locate/neubiorev Review Contingent tolerance to amphetamine hypophagia: new insights into the role of environmental context in the expression of stereotypy D.L. Wolgin* Department of Psychology, Florida Atlantic University, 777 Glades Road, P.O. Box 3091, Boca Raton, FL 33431 USA Received 25 May 1999; received in revised form 1 October 1999; accepted 18 October 1999 Abstract A growing literature attests to the fact that the environment in which a drug is given can have a profound effect on the development and expression of tolerance and sensitization. The dominant paradigm for studying such context-dependency is based on Pavlovian conditioning, in which a distinctive environment serves as a conditioned stimulus. Context dependency is demonstrated when tolerance or sensitization is expressed only in the environment in which the drug was given chronically. An alternative paradigm for studying context-dependency is to manipulate the contingencies of reinforcement operating in the environment in which the drug is administered. For example, tolerance to amphetamine-induced hypophagia is contingent on having access to food while intoxicated [Carlton PL, Wolgin DL. Contingent tolerance to the anorexigenic effects of amphetamine. Physiol Behav 1971;7:221–223]. Such context-dependency can be explained in terms of an instrumental (or operant) conditioning model, in which food serves as a reinforcer for the learned suppression of stereotyped movements that interfere with ingestion. Research based on this model suggests that the expression of sensitized stereotyped responses is subject to an operant level of control. q 2000 Elsevier Science Ltd. All rights reserved. Keywords: Contingent tolerance; Sensitization; Instrumental learning; Amphetamine; Cocaine; Anorexia; Stereotypy; Context-dependency; Response–consequent relation Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2. Early theoretical framework . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3. The mechanisms of amphetamine hypophagia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4. The mechanism of tolerance to amphetamine hypophagia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5. Learned suppression versus channeling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6. The temporal dynamics of learned suppression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7. Contingent loss of tolerance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8. The effect of sensitization on tolerance development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1. Introduction A cardinal principle of behavioral pharmacology is that drug effects are strongly influenced by the context in which the drug is administered. In the drug tolerance/sensitization literature, context usually refers to the physical environment * Tel.: 1 1-561-297-3366; fax: 1 1-561-297-2160. E-mail address: [email protected] (D.L. Wolgin). 279 280 281 282 284 285 287 289 292 292 292 in which the drug is given. For example, it has been well established that tolerance and sensitization to the behavioral effects of a variety of drugs are context-dependent; i.e. they are expressed in the environment in which the drug is chronically administered but not in an environment not previously associated with the drug (for reviews, see Refs. [1–4]). These context-dependent effects are thought to be mediated by associative learning, with the environmental context serving as the CS and the drug serving as the US. 0149-7634/00/$ - see front matter q 2000 Elsevier Science Ltd. All rights reserved. PII: S0149-763 4(99)00070-6 2 280 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 Repeated administration of the drug in the distinctive environment constitutes conditioning trials and results in the environmental context acquiring control over the expression of the drug response. It should be noted that the precise nature of the associative control exerted by the environment is still being debated (see, e.g. Refs. [1,5]). For example, with respect to conditioned sensitization, it has been argued that the environmental context in which the drug is given acts more as an “occasion setter” than as a conventional CS [1]. Similarly, associative accounts of tolerance differ as to whether environmental stimuli elicit a drug-opposite CR [3,6] or an isodirectional CR [7]. Despite these differences, however, all of these views attribute context dependency to an association between the environment in which the drug is given and the drug’s effect. For purposes of experimental control, environments used in studies of context-dependency are designed to be distinctive, but devoid of biologically relevant stimuli, such as food, water, or another animal, with which the subject can interact. In the “real world”, however, drug use takes place in much more complex and “interactive” environments. Such environments contain a rich array of stimuli that may modify the pharmacological and behavioral effects of drugs. Indeed, an early textbook of behavioral pharmacology emphasized the relevance of operant conditioning principles in understanding how both antecedent and consequent stimuli associated with drug administration can alter a drug’s effects [8]. Viewed from the perspective of the operant paradigm, the concept of context dependency takes on an entirely different meaning. When a subject interacts with stimuli in its environment while intoxicated, the consequences of its behavior can alter the topography, temporal patterning, or persistence of drug-induced responses [9]. In addition, environmental stimuli that consistently precede such responses, along with interoceptive stimuli arising from the drug itself, can acquire discriminative stimulus control over the occurrence of those responses. Clearly, the potential for drug–environment interactions is increased when drugs are administered chronically. Such interactions can shape the subject’s behavior, giving rise to patterns of responding that would not have developed in an environment lacking these antecedent and consequent stimuli. In other words, contingent relationships between behavior and its consequences also constitute an environmental context and, therefore, can be expected to contribute to contextdependent effects when drugs are administered chronically. A classic example of this latter type of context dependency is the phenomenon of contingent tolerance to amphetamine-induced hypophagia. When rats are given repeated injections of amphetamine in an environment containing food, they develop tolerance to the initial suppression of feeding. However, if they are given the same number of drug injections in the absence of food, tolerance does not develop [10]. Similar results have been found with cocaine [11], cathinone [12], and methylphenidate [13]. Thus, the opportunity to ingest food while intoxicated plays a critical role in the development of tolerance to the hypophagic effect of stimulant drugs. Despite the apparent simplicity of this example, there is substantial disagreement regarding which of amphetamine’s behavioral effects are altered by the presence of food. Some theorists have argued that contingent tolerance develops to the anorexic effect of the drug [6,14]. According to this view, food serves two functions: (1) It provides feedback of a functional disturbance in nutritional homeostasis and (2) it stimulates a physiological compensatory response to counteract the anorexia. An alternative view is that access to food influences the expression of stereotyped behavior, which nonspecifically interferes with feeding [15]. Normally, when rats are given repeated injections of moderate to high doses of amphetamine ( . 1 mg/kg), the locomotor and stereotyped movements induced by the drug undergo sensitization. Although access to food does not prevent the induction of sensitization, it does influence the expression of stereotypy. Indeed, as I will explain below, rats can learn to inhibit stereotyped responses through instrumental or operant conditioning. Such learning takes place because in an environment containing food, suppressing stereotypy has an important consequence: it allows the rat to eat. 2. Early theoretical framework To develop the argument that contingent tolerance has more to do with stereotypy than anorexia, I will begin with a review of the original study by Carlton and Wolgin [10]. Groups of rats maintained on a daily ration of 10–15 g of food were given access to sweetened milk for 30 min on alternate days. The Before group received an injection of amphetamine (2 or 3 mg/kg) 20 min before the milk test and an injection of saline afterwards; the After group received the injections in the reverse order, and the Saline control group received injections of saline at both time points. In the Before group, amphetamine initially caused a marked decrease in the mean amount of milk consumed, but by the eighth trial intakes exceeded baseline levels; i.e. tolerance developed to the initial suppression of intake. At this point, the order of injections for the After group was reversed so that it now received amphetamine before the milk tests. The After group showed no tolerance on the first day of the reversal. However, with continued pretest injections of the drug, tolerance developed at about the same rate as it had in the Before Group. Thus, there was no apparent benefit with respect to the rate of tolerance development as a result of the prior history of post-test amphetamine injections. These findings were difficult to reconcile with the traditional view that drug tolerance resulted from biochemical alterations triggered by mere exposure to the drug. 3 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 281 Fig. 1. Effect of various doses of amphetamine (left panel) and cocaine (right panel) on the intakes of rats given milk either in bottles or via intraoral cannulas. The rats were maintained on 15 g of food per day. The data are expressed as a percentage of intakes under the saline dose. Intakes were significantly higher in the cannula condition at all common doses. (Cocaine graph adapted from Fig. 1 in Ref. [25]). However, the results of an experiment by Schuster et al. [16] provided a theoretical perspective that seemed to account for the data quite well. In this study, rats treated chronically with amphetamine (1 mg/kg) were reinforced for pressing a lever on a multiple schedule of reinforcement consisting of two components, each separately cued. In one component, the rats were differentially reinforced for responding at a low rate (DRL), while in the other component they were reinforced for responding after a fixed interval of time had elapsed (FI). In two rats, amphetamine initially caused an increase in the rate of responding in both components of the schedule, which resulted in a loss of reinforcement in the DRL component but not in the FI component. With chronic treatment, tolerance developed only to the rate-increasing effect of the drug in the DRL component. In a third subject, however, amphetamine initially caused a decrease in FI responding and a loss of reinforcement. In this rat, tolerance developed in the FI component. On the basis of these findings, Schuster et al. [16] proposed that tolerance develops when the acute effect of a drug results in a loss of reinforcement, but not when the drug increases, or has no effect on, reinforcement density. Since tolerance could be differentially expressed on one component of a multiple schedule but not on another in the same rat, it was clear that more than pharmacological exposure was responsible for such tolerance. And since tolerance was correlated with reinforcement loss, these results suggested that rats could compensate for such loss by actively altering their behavior. The implications of these findings for understanding contingent tolerance seemed straightforward. Rats given chronic injections of amphetamine prior to a feeding test did not eat; consequently, they lost reinforcement. Rats given the drug after the feeding test did not lose reinforcement. Hence, the Before group would be expected to learn to compensate for the loss in some unspecified way, resulting in the development of tolerance, while the After group would not. Although we did not recognize it at the time, the problem with this interpretation is that it contradicts a basic assumption regarding the effect of amphetamine on food intake. To say that amphetamine is anorexigenic is to say that it causes a loss of appetite for food. But if this is true, then food should no longer have reinforcing properties, and therefore, should not serve as an incentive for a learned behavioral compensation. 3. The mechanisms of amphetamine hypophagia This conceptual paradox forced us to re-evaluate our assumptions regarding the mechanism by which amphetamine suppresses food intake. Our thinking was greatly influenced by the results of an experiment in which various doses of amphetamine (2–6 mg/kg) were given prior to daily milk tests over an 8-month period [17]. Two findings from this study stood out. First, although the rats developed tolerance to the initial suppression of feeding at all of these doses, many of them showed extremely variable intakes from day to day. In some cases, their intakes alternated between 0 and 40 or even 50 cm 3. (Baseline intakes for these rats, reassessed at the end of the experiment, ranged from 29– 38 cm 3.) Such variability seemed inconsistent with the view that the drug simply decreased the activity of a homeostatic system controlling food intake [14] or body weight [18]. Second, all of the rats exhibited stereotyped head movements that varied in intensity across subjects and drug doses. Because such movements are incompatible with drinking milk, these observations suggested that behavioral interference may have contributed to the suppression of feeding, a possibility raised earlier by several investigators [19–21]. 4 282 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 To evaluate this possibility, we compared the effect of amphetamine on the intakes of rats given milk either through an intraoral cannula or in a bottle. We reasoned that if amphetamine acts primarily by reducing the appetite for food via anorexia, then intakes should be suppressed to an equivalent degree with both methods of feeding. However, if the drug disrupts feeding in part by inducing incompatible patterns of behavior, then the suppression of intakes should be greater with the bottle, the condition in which the rats must maintain a stationary position in order to feed. Another way to characterize this distinction is in terms of the effects of the drug on the appetitive and consummatory phases of feeding [22,23]. The appetitive phase involves locating, approaching, and maintaining contact with food. This phase is important in the bottle condition, but not in the cannula condition. The consummatory phase, on the other hand, refers to the actual ingestion of food. This phase occurs in both the bottle and the cannula conditions. Therefore, if amphetamine is equipotent in disrupting intake with both methods of feeding, an effect of the drug on the consummatory phase is implicated. However, if amphetamine is more potent in disrupting bottle feeding than cannula feeding, an effect on appetitive behavior is indicated. The intraoral cannulas were constructed from polyethylene tubing and surgically implanted in the dorsorostral region of the mouth to preclude forced swallowing of milk. The tubing was routed subcutaneously along the cheek to emerge at an incision on top of the head, where it was slipped over an L-shaped piece of stainless steel tubing and cemented in place. Milk was gravity-fed from a 50 cm 3 syringe to the cannula through a fluid swivel at a rate of about 1 cm 3/min. The swivel was held in a counterbalance arm, which allowed relatively unimpeded movement by the rat. Throughout the 30-min session, milk flowed continuously through the tubing and the rat could either move it to the back of its mouth and swallow it or let it spill out. Spillage was recovered from trays placed beneath the cage, measured, and subtracted from the volume missing from the syringe at the end of the session. Saline-treated rats typically ingested milk continuously for 30 min with this method, allowing little milk to spill from their mouths. Although they were free to move about as they drank, they typically remained in one location and licked their paws or the cage floor while ingesting the milk. Their daily intakes closely paralleled those of bottle-fed rats [24]. The acute effects of various doses of amphetamine on the intakes of bottle- and cannula-fed rats is shown in Fig. 1 (left). Amphetamine produced dose-dependent decreases in intake with both methods, but the potency of the drug was clearly greater in the bottle condition. For example, at low doses (e.g. 1 mg/kg), amphetamine produced only a 5% reduction in intake in the cannula condition, but a 40% reduction in the bottle condition. At the 2 mg/kg dose, intake was reduced by 20% with the cannula, but by 70% with the bottle. Similar effects were obtained with cocaine ([25]; Fig. 1, right). These results demonstrate that amphetamine and cocaine affect both the appetitive and consummatory phases of feeding, but that the effect is greater on appetitive behavior. Note, in addition, that at doses of amphetamine typically used in feeding experiments (1– 2 mg/kg), there is little suppression of feeding in the cannula condition, suggesting that at these doses anorexia is quite mild. The results of several other studies support this conclusion. For example, analyses of the microstructure of feeding have found that under both amphetamine [26] and cocaine [27], rats are hyperactive, have longer latencies to initiate feeding, and frequently interrupt their meals with periods of activity. Similarly, a number of studies have reported that amphetamine produces reciprocal changes in feeding and motor activity in both normal and brain-damaged rats [28–33]. For example, following 6-hydroxydopamineinduced damage to the nigrostriatal system, amphetaminetreated rats showed reduced stereotypy and increased feeding compared to controls, despite the fact that hypothalamic sites presumed to mediate the anorexic effect of amphetamine were spared [31]. Conversely, following kainic acidinduced damage to the striatum, amphetamine-treated rats showed increased stereotypy [32] and decreased food intake [33]. Finally, the suppression of feeding induced by amphetamine is blocked by “typical” neuroleptics, which also block stereotyped movements, but not by “atypical” neuroleptics, which do not [34,35]. Taken together these findings reinforce the view that amphetamine interferes with feeding primarily by inducing incompatible patterns of behavior. 4. The mechanism of tolerance to amphetamine hypophagia If amphetamine primarily affects the appetitive phase of feeding, then the search for a mechanism of tolerance should focus on changes in the motor effects of the drug that are incompatible with ingestion. Fig. 2 (left panel) shows the effects of daily administration of amphetamine (2 mg/kg) on the activity and milk intakes of bottle-fed rats [15]. The frequency of various categories of behavior (immobility, stationary activity, locomotion, and three types of stereotyped behavior) was measured by rating the rats’ activity at 5 min intervals before, during, and after access to milk. As shown in Fig. 2 (left panel), the recovery of milk intake in bottle-fed rats was accompanied by a decrease in the frequency of stereotyped movements and an increase in the frequency of stationary activity (primarily drinking) while milk was available. Both before and after the period of milk availability, however, these rats engaged in continuous stereotyped movements (data not shown). In contrast, cannula-fed rats showed no change in the frequency of stereotyped behaviors (Fig. 2, right panel). This latter 5 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 Fig. 2. Left: Frequency of stereotyped head movements and stationary activity (top) and mean intakes ( ^ SE; bottom) of rats given daily injections of amphetamine (2 mg/kg) and access to milk in bottles for 24 trials. Activity was scored at 5-min intervals throughout the 30-min session. The development of tolerance to drug-induced hypophagia was accompanied by a significant decrease in stereotyped behavior and an increase in stationary activity. PRE denotes mean intake on the last baseline trial. (From Fig. 4 in Ref. [15]). Copyright q 1987 by the American Psychological Association. Adapted with permission. Right: Frequency of stereotyped head movements and stationary activity (top) and mean intakes (bottom) of rats given daily injections of amphetamine (2 mg/kg) and access to milk via intraoral cannulas for 24 trials. There were no significant changes in either activity or intake over the course of the experiment. (From Fig. 3 in Ref. [15]). Copyright q 1987 by the American Psychological Association. Adapted with permission. 283 6 284 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 finding is important because it demonstrates that tolerance did not develop to the motor effects of the drug. Taken together, these results can be explained by means of a simple instrumental learning model [36]. Because amphetamine induces little anorexia at this dose, as evidenced by the small decrease in intake in the cannula condition, milk would retain its reinforcing properties and could serve as an incentive to suppress stereotyped movements, which interfere with ingestion. If we assume that the suppression of stereotypy requires practice, the gradual increase in drinking over trials may be viewed as a learning curve, illustrating how well, on average, the rats have mastered the task of holding still. Since stereotypy does not interfere with ingestion in cannula-fed rats, no learning would occur in this group. Similarly, no suppression of stereotypy would be expected in tolerant bottle-fed rats during periods in which milk is not available, since at those times there is no incentive to hold still. The instrumental learning model can also account for the contingent nature of tolerance to amphetamine hypophagia [10]. Rats given amphetamine before feeding experience the drug in an environment that provides reinforcement (i.e. milk) for suppressing stereotyped movements. Each trial provides a new opportunity to master this task. In contrast, rats given amphetamine after feeding experience the drug in an environment in which no reinforcement is provided for holding still, and therefore, do not learn to suppress stereotypy. When these rats are later given the drug before feeding, they must begin the learning process de novo, and therefore show no “savings” from their prior drug experience. This interpretation is supported by the results of an experiment on tolerance to the rate-enhancing effects of amphetamine on operant responding [37]. In this study, rats were differentially reinforced for pressing a lever at a low rate, i.e. on a DRL schedule of reinforcement. Amphetamine injections given prior to the task resulted initially in an increased rate of responding, which resulted in a loss of reinforcement. With repeated trials, the rats learned to inhibit their responses so that their inter-response times more closely conformed to the requirements of the schedule. Rats given injections of the drug after the task did not demonstrate such tolerance when they were subsequently tested with pretest injections of the drug. These results confirm that rats can learn to suppress maladaptive patterns of behavior when appropriate reinforcement is available in the environment. There is ample evidence that amphetamine-treated rats are sensitive to the density of reinforcement (e.g. [38]). However, as a study by Smith [39] makes clear, the context in which reinforcement loss occurs must also be considered. In this study, rats were reinforced for pressing a lever on a multiple random ratio (RR), DRL schedule. Amphetamine initially disrupted responding, and caused a loss of reinforcement, in both components of the schedule. During chronic administration of the drug, tolerance developed to the rate-decreasing effect of the drug on RR responding, but not to the rate-increasing effect on DRL responding. However, when the rats were tested on the DRL component alone, tolerance rapidly developed. When the RR component was reinstated, tolerance on the DRL component disappeared once again. As Smith [39] noted, these results suggest that the development of tolerance is influenced by the global density of reinforcement. That is, when the initial effect of the drug results in a loss of reinforcement, the relative cost of that loss influences the development and/or expression of tolerance. In the context of the multiple schedule, the proportion of reinforcers lost in the DRL component was relatively small compared to that in the RR component. Under these conditions, tolerance was not expressed in the DRL component. However, in the absence of the RR component, all of the reinforcers came from the DRL component, and under these conditions tolerance developed rapidly. Thus, context determined whether tolerance was expressed or not. 5. Learned suppression versus channeling Although the instrumental learning model provides a theoretical basis for understanding why tolerance to the hypophagic effect of stimulants is contingent on having access to food, the evidence presented so far is admittedly circumstantial. First, the correlation between decreased stereotypy and increased feeding does not prove that the two events are causally related. Since rats cannot both move their heads and lick a drinking tube simultaneously, an increase in drinking would necessarily be associated with a decrease in stereotyped movements whatever the mechanism of tolerance. Second, the behavior that eventually replaces head movements, licking, is itself a highly stereotyped response. Several studies have shown that the topography of drug-induced stereotypy can be modified by both environmental and experiential factors [40–44]. Consequently, it is possible that in the studies described above, one form of stereotyped behavior (e.g. head scanning) was simply “channeled” into another (licking). Although both the channeling and suppression interpretations are consistent with the instrumental learning model, the ability of rats to actually inhibit stereotyped movements implies a greater degree of “voluntary” control. To address these issues, we designed an experiment to dissociate the suppression of stereotypy from the act of licking a drinking tube [45]. Groups of rats were implanted with intraoral cannulas as previously described. In this case, however, milk was not delivered noncontingently. Instead, the rats were reinforced with intraoral infusions of milk for holding their heads stationary within a narrow area of space defined by intersecting photobeams. Access to this area was provided through a circular opening in one wall of the cage. The duration of each infusion was controlled by the rat; it 8 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 285 Fig. 3. Left: Mean intakes of amphetamine-treated rats given intraoral infusions of milk while holding their heads stationary within intersecting photobeams (Cannula) or given access to milk in bottles in the same location (Bottle). Amphetamine injections were given daily 20 min prior to each 30-min session. Right: Dose–response functions determined before (DR 1) and after (DR 2) chronic administration of amphetamine (2 mg/kg). The data are expressed as a percentage of intakes under the saline dose. (From Fig. 1 in Ref. [45]). lasted as long as the rat’s head remained stationary within the photobeams. The infusion rate was constant at 1 cm 3/ min. After the rats were reliably infusing milk, daily tests with amphetamine (2 mg/kg) were begun. For one group, an empty drinking tube was provided just beyond the photobeams, which could be licked during the infusion; for a second group, no drinking tube was provided. We reasoned that if tolerance involves channeling head movements into licking, only the group having access to the drinking tube should develop tolerance. On the other hand, if tolerance involves learning to suppress stereotyped movements, both groups should become tolerant. For purposes of comparison, a third group was given injections of amphetamine and access to milk in bottles. Four of six rats given chronic injections of amphetamine learned to self-administer infusions of milk by holding their heads stationary within the photobeams. As shown in Fig. 3, the amount of milk ingested as a result of the infusions increased over trials at a rate that was comparable to that of amphetamine-treated rats given milk in bottles. Tolerance was confirmed in both groups by a rightward shift in the dose–response function. The opportunity to lick an empty drinking tube did not affect the development of tolerance. Of the four tolerant rats, two had access to the empty drinking tube while two others did not. Moreover, the two rats that had access to the tube never licked it as they received infusions of milk. These results clearly demonstrate that tolerance does not involve channeling and, more importantly, that amphetamine-treated rats can learn to suppress stereotyped movements in the absence of any physical contact with a drinking tube. The two rats that did not learn to self-administer infusions of milk never approached the circular opening during the entire chronic phase of the experiment. Instead, they engaged in continuous stereotyped sniffing and head scanning throughout each session. However, when subsequently tested with saline injections on the dose–response determination, both rats self-administered about 40 cm 3 of milk. Thus, their failure to learn to suppress stereotyped movements cannot be attributed to inadequate training or to forgetting the appropriate response. Instead, it may have been due to the absence of discriminative cues. Unlike a standard feeding test, in which milk is provided in bottles attached to the front of the home cage in full view of the rat, here there were no cues (sight, smell) associated with the availability of milk. If this analysis is correct, then providing such environmental cues should facilitate learning to suppress stereotypy. 6. The temporal dynamics of learned suppression In order to analyze the development of learned suppression of stereotypy in more detail, we examined the temporal distribution of photobeam interruptions over the course of the experiment. For this purpose, we calculated the total 9 286 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 Fig. 4. Daily milk intake and temporal distribution of photobeam interruptions on selected trials for rat CS1, which was injected with saline during the chronic phase of the experiment. Bars represent the duration of photobeam interruptions in successive 60-s intervals (bins). Numbers adjacent to data points on the intake graph correspond to the selected trials. Note that milk infusions were sustained over many consecutive bins and always began within the first minute. (From data reported in Ref. [45]). duration of interruptions in consecutive 60 s intervals (“bins”) for each trial. These daily profiles of photobeam interruptions provide a detailed picture of the rat’s ability to control the disruptive effects of stereotypy on goal-directed behavior both within and between trials. Fig. 4 is typical of the results for rats tested with saline. Daily milk intake is shown in the upper left panel; the remaining panels show the temporal pattern of photobeam interruptions on selected trials. These trials are indicated by numbers adjacent to the corresponding milk intakes. These rats almost always began to self-administer infusions of milk during the first 60 s of the trial, and their intakes were sustained over many consecutive 60-s intervals. This initial period of drinking was punctuated by brief intermittent pauses, as indicated by bin durations of less than 60 s. Such sustained periods of drinking, which were separated from other periods of drinking by at least 60 s, were defined as a “bout.” Within a trial, subsequent bouts of drinking, if any, were of shorter duration than the initial bout, and were generally separated from the initial bout by several “empty” bins (e.g. trials 10 and 14). Only rarely was a fragmented pattern of photobeam interruptions observed. In contrast, amphetamine-treated rats had longer latencies to initiate milk infusions and showed a more fragmented pattern of photobeam interruptions. This pattern is illustrated in Fig. 5. Note that when milk infusions began for the first time (trial 10), the photobeam interruptions occurred late in the session. On subsequent trials, relatively normal bouts of drinking were found only rarely (e.g. trial 26). On most trials, infusions were either very fragmented or they occurred late in the session. The profiles for the other tolerant rats were qualitatively similar. Quantitatively, amphetamine-treated rats differed from saline controls in two respects. First, the mean number of bouts within a trial was greater in the amphetamine group (3.97 vs. 1.69; tÖ7Ü à 4:56; P , 0:003). Second, the mean number of consecutive 60-s bins in the first bout of drinking (whenever it occurred) was greater in the saline group than in the amphetamine group (15.99 vs. 4.91; tÖ7Ü à 5:41; P , 0:001). These differences reflect the greater degree of behavioral fragmentation in amphetamine-tolerant rats, which resulted from the intrusion of stereotyped movements into the “behavioral stream.” Thus, even though amphetamine-treated rats showed substantial recovery of milk intake, it is clear that the drug 10 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 287 Fig. 5. Daily milk intake and temporal distribution of photobeam interruptions on selected trials for rat CA3, which was injected with amphetamine (2 mg/kg) during the chronic phase of the experiment. Bars represent the duration of photobeam interruptions in successive 60-s intervals (bins). Numbers adjacent to data points on the intake graph correspond to the selected trials. In general, the pattern of photobeam interruptions is fragmented and the latency to initiate milk infusions is delayed on some of the trials. (From data reported in Ref. [45]). continued to exert profound effects on the temporal patterning of their behavior. These results provide important insights into the behavioral nature of tolerance to amphetamine-induced hypophagia. Clearly, tolerant rats do not become refractory to amphetamine’s motor effects; nor are they able to completely suppress the expression of stereotyped movements. Rather, there is an interplay between the contingencies of reinforcement, which encourage a stationary head posture, and the unconditioned motor effects of the drug. As we shall see below, the motor effects undergo sensitization during the course of chronic amphetamine treatment, which may contribute to the disintegration of sustained drinking behavior described above. 7. Contingent loss of tolerance So far, the discussion has focused on the role of instrumental learning on the acquisition of contingent tolerance. But as Poulos et al. [14] first demonstrated, the loss of tolerance to amphetamine hypophagia is also contingent on having access to food in the test environment. That is, if drug injections are suspended, rats lose tolerance if they are given milk tests during the drug-free interval, but they do not lose tolerance if milk tests are also suspended during this period [14]. How does the instrumental learning model account for this example of context dependency? Before addressing this question, some clarification is needed regarding the conditions necessary for the loss of tolerance to amphetamine hypophagia. One might assume that the loss of tolerance results from both the suspension of drug treatment and the continuation of milk tests. But studies involving other drugs suggest that this may not necessarily be the case. For example, contingent tolerance to the anticonvulsant effects of ethanol [46], carbamazepine [47], and diazepam [48] is lost even if rats are given drug injections after convulsant stimulation. These results demonstrate that cessation of drug treatment per se is not necessary for the loss of tolerance. Instead, experiencing the criterion response (in this case, seizure activity) while in the undrugged state appears to be critical. If this principle applies to the loss of tolerance to amphetamine hypophagia as well, then rats should lose tolerance if they are given the opportunity to drink milk in the undrugged state, even if they continue to receive drug injections at some other time. A study by Wolgin and Hughes [49] showed that this is indeed the case. As shown in Fig. 6 (top), tolerant rats given injections of amphetamine after daily milk tests (After group), showed a loss of tolerance, as evidenced by a shift in their dose–response function. Note that the loss was limited to the dose previously given 288 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 Fig. 6. Top: Development and loss of tolerance to amphetamine-induced hypophagia. Dose–response functions were determined before (DR 1) and after (DR 2) daily treatment with amphetamine (2 mg/kg) for 55 trials. The development of tolerance is indicated by the rightward shift in DR 2. Rats in the After group were then given injections of saline before, and injections of amphetamine (2 mg/kg) after, daily milk tests for 4 weeks. Rats in the Saline group were given injections of saline both before and after the milk tests for the same period. On a subsequent dose–response determination (DR 3), both groups showed a loss of tolerance, as evidenced by a leftward shift in DR 3. The loss was more general in the Saline group, however. (Adapted from Fig. 2 in Ref. [49]). Bottom: Motor activity (frequency of locomotion 1 stereotyped movements expressed as a percentage of the frequencies of all categories of behavior) accompanying the development and loss of tolerance to amphetamine-induced hypophagia. Prior to the development of tolerance (DR 1), rats in both groups engaged in motor activity on at least 80% of the rating periods when tested with doses of 1–4 mg/kg. Following chronic administration of amphetamine (2 mg/kg), activity dropped significantly at the 1 and 2 mg/kg doses in both groups (DR 2). With the loss of tolerance (DR 3), activity returned to pretolerance levels. (Adapted from Fig. 4 in Ref. [49]). chronically during tolerance acquisition (2 mg/kg). Tolerant rats given saline injections during this period (Saline group) showed a somewhat more general loss of tolerance, at both the 1 and 2 mg/kg doses. Despite these quantitative differences, these results clearly show that the critical factor in the loss of tolerance to amphetamine hypophagia is drinking milk in the undrugged state, not the cessation of drug treatment per se. We can now return to the question of how the instrumental learning model accounts for the contingent loss of tolerance. When tolerant rats drink milk in the undrugged state, they are, in effect, receiving noncontingent reinforcement; i.e. they no longer need to suppress stereotypy in order to get milk. With continued experience drinking milk under these conditions, they gradually learn that behavioral strategies for suppressing stereotypy are no longer required to ingest milk. Consequently, when the rats are later given access to milk in the drugged state, they no longer suppress stereotyped movements (see Fig. 6, bottom) and are therefore unable to drink. However, when these rats were again given daily injections of amphetamine prior to milk tests, they reacquired tolerance at a faster rate than nontolerant controls. Thus, having once learned how to inhibit stereotypy, they were able to reacquire this skill more quickly. The key point is that, like the acquisition of tolerance, the loss of tolerance is a function of the instrumental relationship between the rat’s behavior and its consequences. When feeding is contingent on suppressing stereotyped movements, rats learn to do so. When the context changes, so that this contingency is no longer operative, these behavioral strategies are no longer exhibited. A recent study by Hughes and Wolgin [50] provides strong support for this interpretation. Rats were given daily injections of amphetamine (2 mg/kg) and access to milk in bottles for 30 min. After they developed tolerance 11 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 289 Fig. 7. Frequency of various components of motor activity during the development of sensitization. The rats were given injections of amphetamine (2.5 mg/kg) at 3-day intervals for 36 trials. The data for each category of behavior are expressed as percentages of the frequencies of all categories. Non-stereotyped responses are displayed as bars, stereotyped responses as line graphs. The maximum raw score for each category on each trial was 96 (16 rats £ 6 rating periods). Sensitization consists of a change in the pattern of movement from primarily locomotion and stereotyped sniffing to one dominated by focused head scanning movements. (From Fig. 1 in Ref. [52]). to the hypophagic effect of the drug, as indicated by a shift in the dose–response function, they were given additional drug trials, but with milk delivered intraorally via an implanted cannula. Thus, ingestion was no longer contingent on suppressing stereotyped movements. Not surprisingly, four of five rats showed a resurgence of stereotyped behavior while drinking from the cannula. When tolerance was subsequently reassessed by again presenting milk in bottles, these rats exhibited a loss of tolerance. In contrast, one rat continued to suppress stereotyped head movements while ingesting milk from the cannula. Consequently, this rat never learned that the contingencies of reinforcement had changed. When tolerance was later reassessed in the bottle condition, this rat did not show a loss of tolerance. These results provide two new insights regarding the loss of tolerance. First, because rats that lost tolerance were injected with amphetamine prior to cannula feeding, it is clear that drug exposure per se (or lack thereof) has nothing to do with whether or not tolerance is retained. Tolerance can be lost when drug treatment is suspended entirely [49], when it is given after milk tests [49] and, as in the present case, when it is given prior to testing. What is critical is the context in which milk is presented, i.e. whether feeding is still contingent on suppressing stereotypy. If it is, then tolerance will be retained. If it is not; then tolerance may be lost. Second, ultimately it is the rat’s behavior that determines whether tolerance is lost or not. Even if the environmental context has changed, tolerance will not be affected unless the rat’s behavior produces appropriate feedback. Thus, a rat that remains stationary while drinking from a cannula will not learn that feeding is no longer contingent on suppressing stereotypy, and, therefore, will retain tolerance when later given milk in a bottle. 8. The effect of sensitization on tolerance development If contingent tolerance involves learning to suppress stereotyped movements in order to feed, then prior sensitization of stereotypy might be expected to retard the subsequent development of tolerance to the hypophagic effect of the drug. Implicit in this prediction is the assumption that sensitized stereotyped movements are less subject to voluntary control. Therefore, as sensitization develops, there should be a progressive disintegration of adaptive, goal directed behaviors like feeding due to an inability to suppress the more intense stereotyped responses (cf. Refs. [21,51]). To test this prediction, rats were given injections of amphetamine (2.5 mg/kg) to induce sensitization of stereotypy [52]. At this dose of amphetamine, sensitization consists of a change in the pattern of movement from primarily locomotion and sniffing to one dominated by focused head scanning. As shown in Fig. 7, on the first few trials, rats given amphetamine displayed stereotyped 12 290 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 Fig. 8. Top: Effect of saline and various doses of amphetamine on milk intakes in sensitized and nonsensitized rats before (DR 1) and after (DR 2) a 48-day period in which the rats received daily injections of amphetamine (2 mg/kg) and access to milk for 30 min. Both the sensitized and nonsensitized rats showed tolerance at the 0.5, 1 and 2 mg/kg doses. (From Fig. 4 in Ref. [52]). Bottom: Motor activity (frequency of locomotion 1 stereotyped movements expressed as a percentage of all categories of behavior) before and after the development of tolerance to amphetamine-induced hypophagia in sensitized and nonsensitized rats. Prior to the development of tolerance (DR 1), the rats in both groups engaged in motor activity on more than 70% of the rating periods when tested at doses of 1–4 mg/kg. (Note, however, that the type of activity differed between the groups.) On DR 2, conducted following the development of tolerance, the frequency of activity decreased significantly at the 1 and 2 mg/kg doses in both groups. (From Fig. 4 in Ref. [52]). sniffing on 60–80% of the rating periods, and either stationary activity (primarily grooming) or locomotion during the remaining periods. On subsequent trials, the frequency of stereotyped sniffing gradually declined to , 20%, while the frequency of focused stereotyped head scanning increased to about 80%. In addition, there was a shift in the onset of head scanning (not shown), so that it appeared progressively earlier in the session. In contrast, controls given saline injections exhibited immobility, stationary activity, or locomotion, but no stereotypy. Following the sensitization phase, both groups were given daily injections of amphetamine (2 mg/kg) and access to milk. Despite clear differences between the groups in the psychomotor effects of the drug at the end of the Fig. 9. Effect of various doses of amphetamine on milk intakes of sensitized and nonsensitized rats before (DR 1) and after (DR 2, DR 3) a 38-day period in which the rats received daily injections of amphetamine (2 mg/kg) and access to milk for 30 min. (DR 3 was a replication of DR 2 to confirm the reliability of the results.) The data are expressed as a percentage of intakes under the saline doses for each DR determination. Although both the sensitized and nonsensitized rats showed tolerance, direct comparisons between the groups revealed that the nonsensitized group drank significantly more at the 4 mg/kg dose than the sensitized group. pDiffers from DR 1; [ p] Main effect of DR (From Fig. 1 in Ref. [54]). 13 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 291 Fig. 10. Effect of saline and various doses of amphetamine on motor activity (locomotion 1 3 categories of stereotyped movements) in sensitized and nonsensitized rats. Each bar indicates the relative amounts of each movement category, expressed as a percentage of the total number of responses from all of the behavioral categories. At each dose, the left bar represents data collected before the tolerance phase (DR 1) and the middle and right bars, data collected after the tolerance phase (DR 2, 3). The maximum score was 40 for the sensitized group and 35 for the nonsensitized group (8 or 7 rats £ 5 rating periods). Sensitized rats showed more oral stereotypy at the 4 mg/kg dose than nonsensitized rats. pDiffers from DR 1. (From Fig. 2 in Ref. [54]). sensitization phase, both groups developed tolerance to amphetamine-induced hypophagia. Dose–response tests conducted before and after the tolerance phase revealed a somewhat greater rightward shift in the nonsensitized control group, but substantial tolerance (Fig. 8, top) and suppression of stereotypy (Fig. 8, bottom) were still found in the sensitized group. Thus, contrary to our expectations, prior sensitization of stereotypy did not retard the development of tolerance to drug-induced hypophagia (see also Ref. [53]). Even more surprising was the finding that during the tolerance phase, sensitization of stereotypy developed in the previously nonsensitized group. This was apparent from an analysis of ratings taken during the 5-min intervals before and after milk was available each day. In the absence of milk, head scanning increased from 25% of all observations prior to the tolerance phase to 63% at the end of that phase. In contrast, when milk was available, head scanning occurred only 20% of the time in the post-tolerance period. Thus, these rats developed sensitization of stereotypy at the same time that they were learning to suppress stereotyped movements in order to feed. Similar results have been found with cocaine [25]. Clearly, having access to milk does not prevent the induction of sensitization of stereotypy. Equally important, however, is that sensitization does not seem to interfere with the rat’s ability to suppress stereotypy when milk is available. Before we accept this conclusion, however, a potential criticism should be addressed. In the studies reported so far, the dose of amphetamine used to induce sensitization of stereotypy (2.5 mg/kg) was very similar to the dose used in the tolerance phase (2 mg/kg). Even after sensitization developed, the type of movements induced by this dose were similar to, albeit more intense than, the movements normally experienced by rats during the tolerance phase of the experiment. It is possible that if a higher sensitizing dose were used, one which produced both quantitative and qualitative changes in the pattern of stereotyped movements, sensitization would interfere with the development of tolerance to amphetamine hypophagia. To address this issue, Hughes et al. [54] gave rats injections of 5 mg/kg amphetamine at three-day intervals for 30 trials to induce sensitization of stereotypy, and then tested the development of tolerance to drug-induced hypophagia, using the standard dose (2 mg/kg) of the drug. At the end of the sensitization phase, amphetamine-treated rats exhibited stereotyped head scanning (74%) and oral stereotypy (24%). When these rats were later given the standard dose of amphetamine during the tolerance phase, they still learned to suppress stereotyped movements in order to drink milk. As shown in Fig. 9 (left panel), tolerance to amphetamine hypophagia was confirmed by a rightward shift of the posttolerance dose–response function, and was associated with a corresponding decrease in stereotyped activity (see Fig. 10, left panel). Thus, once again, prior sensitization of stereotypy did not prevent the development of tolerance to the hypophagic effect of the drug. But is this conclusion valid? Fig. 9 (right panel) shows that the nonsensitized group also showed a shift in its posttolerance dose–response functions, but in this case tolerance generalized to a higher dose (4 mg/kg) as well. Thus, tolerance was more general in the nonsensitized control group than in the sensitized group, suggesting that sensitization of stereotypy may, in fact, have limited the development of tolerance to drug-induced hypophagia. Hughes proposed an interesting explanation for this finding, based on the instrumental learning model. She noted that in the nonsensitized group, the pattern of stereotyped responses elicited by the 4 mg/kg dose (sniffing, head scanning) was qualitatively similar to that elicited by the lower, chronic dose (see Fig. 10, right panel). Consequently, behavioral strategies for suppressing stereotypy that were acquired at the 2 mg/kg dose could generalize to the 4 mg/kg dose. In the sensitized group, however, the pattern of stereotypy elicited by the 4 mg/kg dose contained a relatively high percentage of 14 292 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 oral stereotypy (Fig. 10, left panel). Because little oral stereotypy was experienced by this group at the lower, chronic dose, it did not learn to suppress those responses during the tolerance phase. As a result, tolerance could not generalize to the higher dose during the dose–response tests. In summary, rats exposed to a relatively high sensitizing dose of amphetamine were still capable of learning to suppress stereotyped movements provided that they experienced those movements in an environment in which they could drink milk. Thus, there is no evidence that prior sensitization of stereotypy per se interferes with the subsequent development of tolerance to amphetamine-induced hypophagia. It is still possible, however, that sensitization exerts a more subtle effect on the ability to suppress stereotyped movements. As noted earlier, the temporal pattern of drinking, as measured by photobeam interruptions, is more fragmented in tolerant rats than in saline controls [45]. Thus, while sensitization of stereotypy may not interfere with the development of tolerance as measured by the recovery of milk intake, it may exert an effect on the temporal patterning of drinking behavior. Current research on the role of environmental context in the development of tolerance and sensitization has focused almost exclusively on associative mechanisms. Although this work has provided important insights into the mechanisms controlling these phenomena, we should not lose sight of the fact that context can mean more than just the physical environment in which the drug is given. As research on contingent tolerance demonstrates, instrumental contingencies operating in a particular environment also constitute a context, and can exert a profound effect on the development and/or expression of tolerance and sensitization. When a rat is given chronic injections of amphetamine in an environment in which it can ingest milk, the expression of stereotypy is very different than when the rat is given the drug in an environment without milk. To fully understand the role of environmental context in tolerance and sensitization, therefore, we must broaden the scope of our analyses and consider both associative and operant mechanisms. Note that the experimental paradigms for investigating these mechanisms are very different. For the former, exposure to a distinctive physical environment while intoxicated is sufficient. For the latter, a more interactive environment is required, one in which the rat’s behavior has consequences. 9. Conclusions The ability to suppress stereotyped movements, even after sensitization of stereotypy has developed, challenges several commonly held assumptions regarding stimulantinduced stereotypy in general and sensitization in particular. In contrast to the flexibility, adaptiveness, and goal directedness of normal “voluntary” behavior, stereotyped movements are, by definition, repetitive, aimless and involuntary. Because such movements are typically studied in environments such as open fields or activity boxes, which are devoid of biologically meaningful stimuli, it is easy to think of these movements as being irrepressible. But if rats can learn to suppress even sensitized stereotyped movements, then our assumptions about the uncontrollability of these movements are not justified. In humans, stereotypy of movement or thought is considered a sign of pathology, e.g. in schizophrenia, autism, obsessive-compulsive disorder, addiction, and Tourette’s syndrome [55], precisely because it disrupts adaptive, goal-directed behavior. However, like rats given amphetamine, human patients with tardive dyskinesia, Tourette’s syndrome, l-DOPA-induced chorea and autism can suppress their seemingly involuntary tics, dyskinesias and stereotypies when reinforced for doing so [56–61]. Understanding the neurological mechanisms by which “involuntary” movements can be suppressed through instrumental learning would provide potentially important insights for the clinical management of these disorders. Although little is known about these mechanisms at the present time, there is some evidence that proprioceptive feedback plays a role in the inhibition of dyskinetic movements [58]. Acknowledgements Supported by USPHS grant DA04592 from the National Institute on Drug Abuse. I thank Katherine Hughes for many stimulating discussions and for helpful comments on an earlier draft of the manuscript. I also thank my students and staff for their able assistance in conducting the studies cited in this review and two anonymous reviewers for incisive criticism that substantially improved the manuscript. References [1] Anagnostaras SG, Robinson TE. Sensitization to the psychomotor stimulant effects of amphetamine: modulation by associative learning. Behav Neurosci 1996;110:1397–414. [2] Robinson TE, Browman KE, Crombag HS, Badiani A. Modulation of the induction or expression of psychostimulant sensitization by the circumstances surrounding drug administration. Neurosci Biobehav Rev 1998;22:347–54. [3] Siegel S. Pharmacological conditioning and drug effects. In: Goudie AJ, Emmett-Oglesby M, editors. Psychoactive drugs: tolerance and sensitization. Clifton, NJ: Humana Press, 1989. p. 115–80. [4] Stewart J, Badiani A. Tolerance and sensitization to the behavioral effects of drugs. Behav Pharmacol 1993;4:289–312. [5] Stewart J, Vezina P. Conditioning and behavioral sensitization. In: Kalivas PW, Barnes CD, editors. Sensitization in the nervous system. Caldwell, NJ: Telford Press, 1988. p. 207–24. [6] Poulos CX, Cappell H. Homeostatic theory of drug tolerance: a general model of physiological adaptation. Psychol Rev 1991;98:390–408. [7] Baker TB, Tiffany ST. Morphine tolerance as habituation. Psychol Rev 1985;92:78–108. 15 D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 [8] Thompson T, Schuster CR. Behavioral pharmacology, Englewood Cliffs, NJ: Prentice Hall, 1968. [9] Young AM, Goudie AJ. Adaptive processes regulating tolerance to behavioral effects of drugs. In: Bloom FE, Kupfer DJ, editors. Psychopharmacology: the fourth generation of progress. New York: Raven Press, 1995. p. 733–42. [10] Carlton PL, Wolgin DL. Contingent tolerance to the anorexigenic effects of amphetamine. Physiol Behav 1971;7:221–3. [11] Woolverton WL, Kandel D, Schuster CR. Tolerance and cross-tolerance to cocaine and d-amphetamine. J Pharmacol Exp Therap 1978;205:525–35. [12] Foltin RW, Schuster CR. Behavioral tolerance and cross-tolerance to dl-cathinone and d-amphetamine in rats. J Pharmacol Exp Therap 1982;222:126–31. [13] Emmett-Oglesby MW, Taylor KE. Role of dose interval in the acquisition of tolerance to methylphenidate. Neuropharmacology 1981;20:995–1002. [14] Poulos CX, Wilkinson DA, Cappell H. Homeostatic regulation and Pavlovian conditioning in tolerance to amphetamine-induced anorexia. J Comp Physiol Psychol 1981;95:735–46. [15] Wolgin DL, Thompson GB, Oslan IA. Tolerance to amphetamine: contingent suppression of stereotypy mediates recovery of feeding. Behav Neurosci 1987;101:264–71. [16] Schuster CR, Dockens WS, Woods JH. Behavioral variables affecting the development of amphetamine tolerance. Psychopharmacologia 1966;9:170–82. [17] Wolgin DL, Salisbury JJ. Amphetamine tolerance and body weight set point: a dose–response analysis. Behav Neurosci 1985;99:175– 85. [18] Stunkard AJ. Anorectic agents: a theory of action and lack of tolerance in a clinical trial. In: Garattini S, Samanin R, editors. Anorectic agents: mechanisms of action and tolerance. New York: Raven Press, 1981. p. 191–210. [19] Carlton PL. Cholinergic mechanisms in the control of behavior by the brain. Psychol Rev 1963;70:19–39. [20] Cole SO. Brain mechanisms of amphetamine-induced anorexia, locomotion, and stereotypy: a review. Neurosci Biobehav Rev 1978;2:89– 100. [21] Lyon M, Robbins T. The action of central nervous system stimulant drugs: A general theory concerning amphetamine effects. In: Essman WV, Valzelli L, editors. Current developments in psychopharmacology. New York: Spectrum, 1975. p. 78–163. [22] Craig W. Appetites and aversions as constituents of instincts. Biol Bull 1918;34:91–107. [23] Tinbergen N. The study of instinct. New York: Oxford University Press, 1951. [24] Salisbury JJ, Wolgin DL. Role of anorexia and behavioral activation in amphetamine-induced suppression of feeding: implications for understanding tolerance. Behav Neurosci 1985;99:1153–61. [25] Wolgin DL, Hertz JM. Effects of acute and chronic cocaine on milk intake, body weight, and activity in bottle- and cannula-fed rats. Behav Pharmacol 1995;6:746–53. [26] Blundell JE, Latham CJ. Characterisation of adjustments to the structure of feeding behaviour following pharmacological treatment: effects of amphetamine and fenfluramine and the antagonism produced by pimozide and methergoline. Pharmacol Biochem Behav 1980;12:717–22. [27] Cooper SJ, van der Hoek GA. Cocaine: a microstructural analysis of its effects on feeding and associated behaviour in the rat. Brain Res 1993;608:45–51. [28] Cole SO. Interaction of arena size with different measures of amphetamine effects. Pharmacol Biochem Behav 1977;7:181–4. [29] Cole SO. Interaction of food deprivation with different measures of amphetamine effects. Pharmacol Biochem Behav 1979;10:235–8. [30] Heffner TG, Zigmond MJ, Stricker EM. Effects of dopaminergic agonists and antagonists on feeding in intact and 6-hydroxydopamine-treated rats. J Pharmacol Exp Therap 1977;201:386–99. 293 [31] Joyce EM, Iversen SD. Dissociable effects of 6-OHDA-induced lesions of neostriatum on anorexia, locomotor activity and stereotypy: the role of behavioral competition. Psychopharmacology 1984;83:363–6. [32] Mason ST, Sanberg PR, Fibiger HC. Amphetamine-induced locomotor activity and stereotypy after kainic acid lesions of the striatum. Life Sci 1978;22:451–60. [33] Sanberg PR, Fibiger HC. Body weight, feeding, and drinking behaviors in rats with kainic acid-induced lesions of striatal neurons— with a note on body weight symptomatology in Huntington’s disease. Exp Neur 1979;66:444–66. [34] Burridge SL, Blundell JE. Amphetamine anorexia: antagonism by typical but not atypical neuroleptics. Neuropharmacology 1979;18:453–7. [35] Robertson A, MacDonald C. Atypical neuroleptics clozapine and thioridazine enhance amphetamine-induced stereotypy. Pharmacol Biochem Behav 1984;21:97–101. [36] Wolgin DL. The role of instrumental learning in behavioral tolerance to drugs. In: Goudie AJ, Emmett-Oglesby M, editors. Psychoactive drugs: tolerance and sensitization. Clifton, NJ: Humana Press, 1989. p. 17–114. [37] Campbell JC, Seiden LS. Performance influence on the development of tolerance to amphetamine. Pharmacol Biochem Behav 1973;1:703–8. [38] Galbicka G, Kautz MA, Ritch ZJ. Reinforcement loss and behavioral tolerance to d-amphetamine: using percentile schedules to control reinforcement density. Behav Pharmacol 1992;3:535–44. [39] Smith JB. Effects of chronically administered d-amphetamine on spaced responding maintained under multiple and single-component schedules. Psychopharmacology 1986;88:296–300. [40] Borberg S. Conditioning of amphetamine-induced behaviour in the albino rat. Psychopharmacologia 1974;34:191–8. [41] Collins JP, Lesse H, Dagan LA. Behavioral antecedents of cocaineinduced stereotypy. Pharmacol Biochem Behav 1979;11:683–7. [42] Ellinwood EH, Kilbey MM. Amphetamine stereotypy: the influence of environmental factors and prepotent behavioral patterns on its topography and development. Biol Psychiat 1975;10:3–16. [43] Robbins TW. Relationship between reward-enhancing and stereotypical effects of psychomotor stimulant drugs. Nature 1976;264:57– 59. [44] Sahakian BJ, Robbins TW. The effects of test environment and rearing condition on amphetamine-induced stereotypy in the guinea pig. Psychopharmacologia 1975;45:115–7. [45] Wolgin DL, Wade JV. Learned suppression of stereotypy in amphetamine-treated rats: implications for understanding tolerance to amphetamine ‘anorexia’. Behav Pharmacol 1995;6:254–62. [46] Mana MJ, Pinel JPJ. Response contingency and the dissipation of ethanol tolerance. Alcohol 1987;4(Suppl. 1):413–6. [47] Weiss SRB, Post RM. Development and reversal of contingent inefficacy and tolerance to the anticonvulsant effects of carbamazepine. Epilepsia 1991;332:140–5. [48] Kalynchuk LE, Kippin TE, Pinel JPJ, McIntyre CP. Dissipation of contingent tolerance to the anticonvulsant effect of diazepam: effect of the criterion response. Pharmacol Biochem Behav 1994;49:1113– 7. [49] Wolgin DL, Hughes KM. Role of behavioral and pharmacological variables in the loss of tolerance to amphetamine hypophagia. Psychopharmacology 1997;132:342–9. [50] Hughes KM, Wolgin DL. Changes in behavioral contingencies without disrupted drug exposure can produce a loss of tolerance to amphetamine hypophagia in rats. Soc Neurosci Abstr 1999;25:2082. [51] Teitelbaum P, Pellis SM, DeVietti TL. Disintegration into stereotypy induced by drugs or brain damage: a microdescriptive behavioural analysis. In: Cooper SJ, Dourish CT, editors. Neurobiology of stereotyped behaviour. Oxford: Clarendon Press, 1990. p. 169–99. [52] Wolgin DL, Hughes KM. Effect of sensitization of stereotypy on the 16 294 [53] [54] [55] [56] [57] D.L. Wolgin / Neuroscience and Biobehavioral Reviews 24 (2000) 279–294 acquisition and retention of tolerance to amphetamine hypophagia. Psychopharmacology 1996;126:219–25. Wolgin DL, Kinney GG. Effect of prior sensitization of stereotypy on the development of tolerance to amphetamine-induced hypophagia. J Pharmacol Exp Therap 1992;262:1232–41. Hughes KM, Popi L, Wolgin DL. Experiential constraints on the development of tolerance to amphetamine hypophagia following sensitization of stereotypy: instrumental contingencies regulate the expression of sensitization. Psychopharmacology 1998;140:445–9. Ridley RM. The psychology of perseverative and stereotyped behaviour. Progr Neurobiol 1994;44:221–31. Azrin NH, Peterson AL. Treatment of Tourette syndrome by habit reversal: a waiting-list control group comparison. Behav Ther 1990;21:305–18. Azrin NH, Kaplan SJ, Foxx RM. Autism reversal: eliminating [58] [59] [60] [61] stereotyped self-stimulation of retarded individuals. Am J Ment Def 1973;78:241–8. Caligiuri MP, Lohr JB. A potential mechanism underlying the voluntary suppression of tardive dyskinesia. J Psychiat Res 1989;23:257– 66. Evers RAF, Van De Wetering BJM. A treatment model for motor tics based on a specific tension-reduction technique. J Behav Ther Exp Psychiat 1994;25:255–60. Messiha FS, Carlson JC. Behavioral and clinical profiles of Tourette’s Disease: a comprehensive overview. Brain Res Bull 1983;11:195– 204. Walters AS, McHale D, Sage JI, Hening WA, Bergen M. A blinded study of the suppressibility of involuntary movements in Huntington’s chorea, tardive dyskinesia, and l-DOPA-induced chorea. Clin Neuropharmacol 1990;13:236–40.