Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
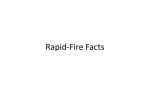
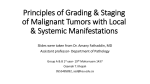
http://www.medicine-on-line.com Hemoptysis, shoulder pain, weight loss: 1/5 Case 035: Hemoptysis, shoulder pain, and weight loss. Authors: Gregory E Antonio MD, FRANZCR David C Chung MD, FRCPC Thomas YK Chan MD, PhD, FRCP Affiliation: The Chinese University of Hong Kong A 65-year-old male patient presented to the outpatient clinic with complaints of hemoptysis, pain around his right shoulder, and weight loss. He has been a onepack-a-day smoker for more than 40 years and had a “smoker’s cough” for as long as he could remember. The cough was usually worst in the morning; the sputum it produced was usually grayish-white; but it was mixed with flecks of blood on several days in the last month. The onset of shoulder pain was insidious and he described it as a gnawing sensation accentuated by movement. He lost 9 kg over the past 6 months and attributed it to lack of appetite. He was diagnosed to have pulmonary tuberculosis (TB) in 1962 and received a course of drug therapy for 2 years. Otherwise there was no history of hypertension, ischemic heart disease, and diabetes. He was not on any medications and he had no allergy. On examination the patient looked thin and gaunt but not in distress. His vital signs were: Oral temperature 36.6 oC, BP 134/80 mmHg, pulse rate 80/min, respiratory rate 20/min. There was no cyanosis or clubbing. Auscultation of the chest revealed diffused inspiratory and expiratory wheezes together with bronchovesicular breath sound in the right apex. The right shoulder was normal to examination; there was no cervical lymphadenopathy. There was obvious ptosis of the right upper eyelid; the right pupil was smaller than the left; the right side of his face was warm and dry in comparison to his left. Otherwise, his heart sounds were normal; abdomen was soft with no organomegaly; power of the extremities was normal; mental status was clear. 1. What are the differential diagnoses? When a patient presents with hemoptysis, efforts should be directed at differentiating where the blood comes from: from the lungs, the upper airway, or http://www.medicine-on-line.com Hemoptysis, shoulder pain, weight loss: 2/5 the upper gastrointestinal (GI) tract. It is quite possible for blood from the upper airway or regurgitated blood from the upper GI tract to drip down the trachea to be coughed up again to mimic hemoptysis. With our patient the blood is mixed with the sputum, making it more likely to have come from the lungs. Together with weight loss and history of TB and smoking, reactivation of old TB or lung cancer are the most likely diagnoses. Besides symptoms and signs referable to the respiratory system, this patient also has signs of a right Horner’s syndrome, suggesting involvement of the stellate ganglion of the right sympathetic chain by the disease process. Whatever this disease process is, the patient needs further investigation, including a chest x-ray which is shown below: 2. What are the abnormalities seen on this chest x-ray? http://www.medicine-on-line.com Hemoptysis, shoulder pain, weight loss: 3/5 This frontal chest radiograph shows background lung changes of Chronic Obstructive Pulmonary Disease, i.e. hyperinflated and lucent lungs (emphysematous changes). There is a mass (large arrow) in the right apical region which is non-specific but in this clinical setting is suggestive of a neoplastic lesion. There are numerous small nodules (small arrows) in the mid and upper zones of both lungs, which may represent granulomata (from previous tuberculous infection) but metastatic deposits cannot be excluded. Progress of the Case: Biopsy at bronchoscopy and mediastinoscopy proved that the tumor was malignant. A malignant tumor at this location is called a Pancoast tumor. http://www.medicine-on-line.com Hemoptysis, shoulder pain, weight loss: 4/5 3. What is a Pancoast tumor? A Pancoast tumor (superior sulcus tumor) is nothing more than a bronchial carcinoma situated at the superior sulcus of the upper lobe of the right lung. It was first reported by Dr. HK Pancoast in 1924 and thus acquired his name. By virtual of its location, the tumor can invade adjacent structures and bring on the Pancoast syndrome with its associated manifestations: Structures involved Manifestations 2nd and 3rd ribs Upper chest pain and shoulder pain Stellate ganglion Horner’s syndrome C8 & T1 roots of brachial plexus Hand weakness & atrophy / parasthesia Subclavian vein / superior vena cava Venous obstruction Phrenic nerve Palsy of right diaphragm Recurrent laryngeal nerve Hoarseness Besides bronchial carcinoma, rarer causes of the Pancoast syndrome include: Metastatic tumors. Hematological malignancies. Infections. Cervical rib. Pulmonary amyloid nodules. 4. What is the treatment of superior sulcus bronchial carcinoma? When a patient presents with the Pancoast syndrome from superior sulcus bronchial carcinoma, invasion of adjacent structures has occurred and prognosis is guarded. However progress in surgery, chemotherapy, and radiation therapy— either alone or in combination—has brought a ray of hope in recent years. The patient should be referred to a specialist center for further evaluation and treatment. http://www.medicine-on-line.com Hemoptysis, shoulder pain, weight loss: 5/5 Further reading Archie VC et al. Superior sulcus tumors: A mini-review. The Oncologist 2004;9:550.