Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
REVIEW ARTICLE
Molecular Genetics of von Willebrand Disease
By David Ginsburg and E.J. Walter Bowie
V
ON WILLEBRAND disease (vWD) was first described
by Erik von Willebrand in 1926l in several members of
a family from the h a n d archipelago in Finland. The
proband, a 7-year-old girl, and 9 of her 11 siblings all had
significant bleeding symptoms, four dying of hemorrhage
between the ages of 2 and 4 and the proband herself dying
of hemorrhage at the age of 13 at the time of her fourth
menstrual period. von Willebrand coined the term “hereditary pseudohaemophilia” for the disease that subsequently
bore his name. In retrospect, the first case of vWD may
actually have been described by Minot and Lee in 1920,2
and a similar clinical disorder was reported independently
by four American groups in 1928.3,4In 1953, an association
between decreased factor VI11 (FVIII) procoagulant activity and vWD was first described, leading to some confusion
concerning the protein defects responsible for hemophilia
A and v W D . ~An
, ~ explosion in the understanding of von
Willebrand factor (vWF) and FVIlI began with the immunologic characterization of the proteins in the early 1970s,
culminating in the cDNA cloning of FVIII in 19845,6and
vWF in 1985.7-10Molecular defects responsible for hemophilia and vWD were first detected by Southern blot
analysis in 198S1 and 1987,12,13
respectively. The subsequent identification of point mutations in DNAs from large
numbers of hemophilic and vWD patients was made possible by the discovery of the polymerase chain reaction in
1985 and the application of Tuq polymerase in 1987.14J5
This review will focus on the molecular genetics of vWD.
The biosynthesis, structure, and function of the vWF
protein will only be briefly introduced. For a more detailed
discussion of these latter topics, the interested reader is
referred to several excellent recent reviews.16-20
vWF BIOSYNTHESIS
The vWF monomeric subunit of approximately 250 Kd in
molecular weight is assembled into multimers containing
up to 100 subunits with molecular weights in excess of 20 x
loh daltons. vWF is synthesized exclusively in endothelial
cells and megakaryocytes and has become a standard
marker of endothelial cell origin for histochemical studies.
vWF is first synthesized as a large prescursor form that
initially dimerizes and subsequently multimerizes with coincident processing to the mature vWF subunit. Within the
endothelial cell, vWF is secreted via both constitutive and
regulated pathways. Dimerization of vWF and early carbohydrate processing begin in the endoplasmic reticulum with
final carbohydrate processing and multimerization restricted to golgi and post-golgi compartments. A specific
storage compartment for vWF has been identified within
the endothelial cell termed the Weibel-Palade body. This
structure contains densely packed vWF with a characteristic appearance under the electron microscope. The only
other protein known to be contained within the WeibelPalade body is the recently described selectin, GMP140
Blood, Vol79, No 10 (May 15). 1992: pp 2507-2519
(P-selectin).21,22Platelet vWF is stored within the a-granuole.’6
STRUCTURE AND FUNCTION OF vWF
In plasma, vWF serves two major function. Via specific
binding to the platelet surface as well as to one or more
discrete ligands within the subendothelium, vWF provides a
major adhesive link between the platelet and the vessel wall
at sites of vascular injury. In addition, vWF serves as the
carrier for FVIII in plasma, conferring increased stability
and localizing FVIII to sites of platelet plug and subsequent
fibrin clot formation.
The various binding functions of vWF appear to be
localized to discrete domains within the molecule as shown
by studies of proteolytic vWF fragments (summarized in Fig
1and reviewed in Ruggeri and Zimmerman,17Girma et a1,’8
Ruggeri,19 and SadlerZo). The FVIII binding domain of
vWF has been localized to a 272 amino acid tryptic
In addition, two
fragment at the N-terminus of
monoclonal antibodies mapping to an epitope spanning
amino acids 78 through 9625,26were shown to block FVIII
binding to vWF, suggesting a further localization for this
function. Recent evidence suggests that the mature vWF
N-terminus is required for FVIII binding,27 although the
role of the vWF propeptide is c o n t r ~ v e r s i a l .Regions
~~~~~
involved in binding to platelet glycoprotein Ib (GPIb),
heparin, and collagen have been localized to a 48/52-Kd
tryptic fragment spanning Val449 through L y ~ 7 2 8 . ~An
~-~’
additional potential collagen binding domain has been
mapped to residues 911-1114.32,33Finally, an RGDS sequence thought to function as a ligand for the GPIIb/IIIa
platelet surface integrin is located at amino acids 17441747.
THE vWF GENE AND cDNA
vWF cDNAs were independently isolated by four groups
in 1985.7-1°The complete primary amino acid sequence of
the mature vWF subunit was also independently determined by Titani et aP4 using direct amino acid sequence
analysis. In addition to the expected agreement with the
From the Howard Hughes Medical Institute, Departments of
Human Genetics and Internal Medicine and Program of Cellular and
Molecular Biology, University of Michigan Medical School, Ann
Arbor, MI; and the Mayo Clinic, Section of Metabolic and Hemutologic Biochemistry, Department of Laboratory Medicine & Patholoa,
Rochester, MN.
Submitted November 12,1991; accepted February 28, 1992.
Supported in part by National Institutes of Health Grant No.
I-ROlHL39693. D.G. is a Howard Hughes Medical Institute Investigator.
Address reprint requests to David Ginsbuig, MD, Howard Hughes
Medical Institute, 1150 W Medical Center Dr, 4520 MSRBL Ann
Arbor, MI 48109-0650.
0 1992 by The American Society of Hematology.
0006-4971I921 7910-0039$3.0OlO
2507
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
GINSBURG AND BOWIE
2508
segments of thrombospondin and procollagen has also been
I
_.._1
I
272
I
I
’
U9
12.9
911
I
1114
17UI
mor
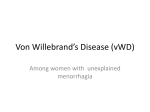
Fig 1. Schematic of tho human vWF gene, mRNA, and protein. l h a
vWF gem end pseudogene are depicted nt the top with boxes
repmaontingexons and the solid black line, introns. The vWF mRNA
encoding the full prepro-vWFsubunit is depicted in the middle as the
stippled bar and lettered boxes. The location of signal peptide (sp)
and propeptide (pro-)cleavage sites are indicatedby anowheads, and
the lettered boxes denote regions of internally repeated sequence.
The approximate localizations for known vWF functional domains
within the mature vWF sequence ere indicated at the bottom.
Numbers undemeath the domains refer to amino acid residues within
the mature vWF subunit. The clusters of mutations responsible for
type IIA vWD, type IIB vWD, and the FVtll binding defects are
indicated. (aa. amino acids; chr, chromosome.)
cDNA
the direct protein analysis also identified
the location of N- and 0-linked glycosylation sites within
the mature vWF subunit.J4 Surprisingly, the vWF cDNA
predicted a 309-Kd (2,813 amino acid) primary translation
product with the sequence corresponding to the N-terminus of mature vWF beginning at codon 764. The N-terminal
segment was shown to encode a typical hydrophobic signal
peptide followed by sequence identical to von Willebrand
antigen I1 (vWA~II)?.~~-’~.~”
vWAglI is a plasma protein of
previously unknown function, associated with, but distinct
from VWF.~”,~’
The vWF propeptide (vWAgll) was subsequently shown to play an important role in the process of
vWF m u l t i m e r i z a t i ~ nand
~ ~ ~targeting to the WeibelPalade b0dy.4~The vWF propeptide is removed by a single
proteolytic cleavage between codon 763 and 764, following
two basic amino acid residues (Lys-Arg). This cleavage has
recently been shown to be mediated by a specific paired
basic amino acid cleaving enzyme with sequence similarity
to the subtilisin-like protease family, including the yeast
protease K e ~ 2 . 4 ~
Analysis of the vWF cDNA sequence also shows a
pattern of repeated homologoussequence domains, suggesting that the gene may have arisen via a complex process of
gene segment d u p l i c a t i ~ n . ~ ~The
- ’ ~ *positions
~~
of these
domains with respect to the various localized vWF functions are shown schematically in Fig 1. Comparison of vWF
to other known sequences within the available protein and
DNA databases shows limited, but potentially important,
sequence similarities. This is most evident for the A
domains, which share significant sequence similarity with
the “L“domains of the MAC-1 integrin receptor a subunit,
chicken cartilage matrix protein, and type VI c0llagen.4~A
possible distant relationship between the C repeats and
The human vWF gene has been localized to chromosome
12~1+
2 pter.7*“’Localization studies using a cDNA probe
from the midportion of vWF identified not only the authentic gene on chromosome 12 but a second sequence on
chromosome 22.12 The latter has recently been localized to
22q11.22-ql 1.23.49The complete exon/intron structure of
the vWF gene has been established by Mancuso et al.”)The
52 exons span 178 kb, approximately 0.1% of human
chromosome 12. Exons range from 40 bp to 1.4 kb for the
largest exon (exon 28). The latter encodes the entire AI
and A2 repeats, a critical region of the molecule spanning
several important functional domains (Fig 1) and also
containing most of the mutations responsible for type IIA
and type IIB vWD (see below). The vWF intron/exon
structure shows little correlation with the homologous
repeat structure described above. Although there is some
limited correspondenceof introns in the D domains, the A1
and A2 domains are contained in a single exon, whereas the
A3 domain extends across 5 exons.” Nearly the entire vWF
pseudogene on chromosome 22 has now been sequenceds1
and shows 97% homology to the authentic chromosome 12
gene, indicating a very recent evolutionary origin. The
pseudogene represents a nonprocessed duplication spanning exons 23-34.5l The presence of multiple stop codons in
the coding sequence provides conclusive evidence that this
is not a functional gene in humans. Southern blot studies
confirm the absence of this pseudogene in a number of
other mammalian species.’U3 The location and high degree
of sequence identity between the pesudogene and authentic
gene present particularly difficult problems for the identification of mutations in vWD (see below).
Information on potential regulatory elements within the
vWF gene includes the analysis of 2.2 kb of upstream
sequence. Although there is a typical “TATA” box at -30,
no “CCAAT” or “ G C box elements are
Transfection studies using vWF promoter sequences have
been difficult and little information is currently available to
explain the extremely high level of expression of vWF in
endothelial cells and megakaryocytes and its remarkable
tissue specificity.
vWD
vWD is an extremely heterogeneous disorder, with over
20 distinct clinical subtypes described (Table 1).1755-s9 The
numerous vWD variants generally all fit into one of two
classes, characterized by either quantitative (types I and
111) or qualitative (type 11 and other variants) defects in
vWF. For the former class, vWF of relatively normal
appearing structure and function may be present, but in
significantly decreased amounts. In type I, vWF levels are
generally between 20% and 50% of normal, and in type 111,
levels are extremely low or undetectable. The type I variant
of vWD is by far the most common, accounting for at least
70% of clinical cases. Type 111 vWD is much less common
with frequency estimated at approximately 1 per million.”“ Overall prevalence figures for all cases of vWD
have ranged as high as 1% to 3% of the population$1*62
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
VON WILLEBRAND DISEASE
2509
Table 1. Summary of vWD Phenotypes
Clinical
Subtype
Frequency
Features
Diagnosis
1-3O:l.OOO; most common
vWD variant ( > 70% of
vWD)
Mild t o moderate bleeding;
autosomal dominant; incomplete penetrance (approximately 60%).
Severe bleeding disorder;?
autosomal recessive inheritance.
vWF:Ag, vWF:RCo, and
FVlllC all proportionately
decreased (20-50%). Normal multimer distribution.
Markedly decreased or undetectable vWF:Ag, vWF:
RCo, and FVIIIC.
1-5: lo6
Type IIA
Approximately 10-15% of
clinical vWD cases
Mild to moderate bleeding
disorder; autosomal dominant, more complete penetrance than type I; generally poor response t o
DDAVP.
Variable decreased vWF:Ag,
vWF:RCo, and FVIIIC; absent high and intermediate
size vWF multimers with
prominent satellite bands;
Type llB
Uncommon variant
( < 5 % of clinical vWD)
Types IIC-H. others
Rare (case reports)
Mild to moderate bleeding
disorder; autosomal dominant, more complete penetrance than type I;? DDAVP
contraindicated.
Variable bleeding disorder;
generally autosomal dominant though some autosomal recessive (type IIC).
FVlll binding defects
(vWF Normandy)
Rare (case reports)
Variable bleeding disorder;
homozygotes (or compound heterozygotes) may
present as autosomal hemophilia A.
Platelet-type vWD
("pseudo-vWD)
Rare (case reports)
Similar to type llB vWD.
Variably decreased vWF antigen vWF:RCo and FVIIIC;
loss of large multimers;
enhanced RIPA; thrombocytopenia.
Variably decreased vWF:Ag,
vWF:RCo, and FVIIIC. Diag.
nosis generally based on
unique abnormalities in
multimer pattern.
Variable vWF:Ag and vWF:
RCo. Disproportionately
low FVIIIC. Generally normal multimers. Decreased
or absent vWF binding to
FVIII.
Can be distinguished from
type llB by mixing studies
with normal platelets and
plasma.
although others suggest a considerably lower range of
approximately 1:10,000.56,59
The sensitivity and specificity of
the current standard diagnostic tests (vWF:Ag, vWF ristocetin cofactor activity [vWF:RCo], FVIII procoagulant activity [FVIIIC], and bleeding time) may be as low as 60%.63
Additional variability is contributed by a number of other
factors, including blood group and estrogen leve1.56,M,65
Mean vWF:Ag levels can vary from 75% for blood type 0
individuals to 123% for type AB, when compared with a
standard normal donor plasma pool. As a result, the
diagnosis of vWD may be more readily established in
patients who are blood type 0. Clinical symptoms are more
common in women, most likely due to the hemostatic
stresses of pregnancy and menstruation. The bewildering
complexity of vWD classification and the low accuracy of
the current diagnostic tests present major problems for the
practicing clinical hematologist. These issues lend additional importance to the identification of vWF mutations, to
eventually facilitate the precise diagnosis and classification
of vWD at the molecular level.
The treatment of choice for mild type I vWD is DDAVP.
Intravenous or intranasal administration of this vasopressin
Molecular
Basis
Unknown.
vWF gene deletions; nonsense mutation; other cisdefects in mRNA expression.
Missense mutations clustered within vWF A2 domain. Two subgroups:
group 1-Defect in intracellular transport; group 2-?
proteolysis in plasma after
secretion.
Missense mutation clustered
in vWF A1 domain result in
increased or spontaneous
binding t o platelet GPlb.
Unknown, some may represent compound heterozygotes for other variants.
Missense mutations within
the N-terminus of mature
vWF which interfere with
FVlll binding.
Missense mutation within
GPlb a-chain probably resulting in increased or
spontaneous binding to
vWF.
analogue generally results in marked elevation of vWF and
FVIIl levels, providing adequate hemostasis in the majority of patient^.^',^^ This treatment is much less effective in
the type 111and type I1 variants and may be contraindicated
in type IIB
In this latter group of patients, as well
as type I vWD patients who have otherwise failed DDAVP,
the treatment of choice is replacement of vWF either in the
form of pooled plasma fractions (cryoprecipitate) or, more
recently, partially purified FVIII concentrates that also
contain intact vWF m~ltimers.~'
These latter products are
thought to be free of viral transfusion risks on the basis of
heat or detergent treatment. Whether cryoprecipitate or
one of the purified products should be the first line
treatment for severe (type 111) vWD and type I1 variants
remains controversial.
ANIMAL MODELS FOR vWD
In addition to its high prevalence in human populations,
vWD has also been frequently encountered in other animal
species, including dogs, rabbits, cats, mice, pigs, and
horses.52,69-74
Heterogyzotes for porcine vWD are generally
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
2510
GINSBURG AND BOWIE
asymptomatic, while homozygotes have less than 1% of
normal vWF levels and a severe bleeding diathesis closely
resembling type I11 human V W D . ~ * , ’vWD
~ - ~ ~ has been
recognized in over 30 breeds of dogs, including examples of
type 111, type I, and type I1 vWD. The prevalence of vWD is
extremely high in several inbred dog strains (up to 65% of
Doberman Pinchers and Airedale terrier^).^^ Murine vWD
has been recently described in the RIIIS/J mouse, identified by a screen of 25 inbred mouse strains, again suggesting
a high spontaneous frequency for this disorder among
mammalian species. vWD in the RIIIS/J mouse appears to
most closely resemble human type I vWD. It is autosomal
dominant in inheritance associated with a partial defect in
plasma vWF, prolonged bleeding time, and decreased
platelet aggregation. Type I vWD in this animal model
appears to be a “true dominant” disorder with homozygotes and heterozygotes having similar phenotype^.^^ These
data also suggest that type I11 vWD is not simply the
homozygous form of type I vWD (see below).
The reason for the high frequency of vWD in humans and
other mammalian species remains unclear. vWD may have
a protective effect against atherosclerosis in the porcine
mode1,72,74,75
although no such effect has yet been shown in
humans.7hHowever, given the generally late age of onset for
clinically significant heart disease, a protective effect from
vWD probably would not exert a strong evolutionary
pressure and should be easily outweighed by even mild
changes in hemorrhagic risk. Interestingly, vWD also appears to afford some resistance to bacterial endocarditis in
the porcine
In addition, a sequence similarity has
recently been noted between the YopM outer membrane
protein of the Yersinia pestis organism (the pathogenic
bacteria of plague) with the a-chain of GPIb,78,79the
platelet surface receptor for vWF. YopM- mutants of
Yersinia pestis show decreased virulence in mice.7y If an
interaction between YopM and vWF is important for
virulence, a potential relative protection from this or other
pathogenic bacteria may have provided a strong selective
pressure for vWD. The large size of the vWF gene may also
afford an ample target for mutation, a proposed explanation for the high mutation rates observed in several other
disorders associated with unusually large proteins and
genes, such as hemophilia A and muscular dystrophy.8D
For any autosomal dominant disease, the proportion of
cases representing new mutations should be directly related
to the decrease in reproductive fitness associated with the
disorder.s1 Because vWD is in general a mild disorder, the
decrease in reproductive fitness would be expected to be
small, and thus the relative proportion of new mutations in
von Willebrand disease should be low. Consistent with this
hypothesis only a few patients have been identified in whom
vWD appears to have arisen as a new genetic event (see
below).
GENETIC LINKAGE ANALYSIS IN vWD
Given the complexity of vWF biosynthesis, secretion, and
function, defects at a variety of genetic loci could potentially result in a vWD phenotype. As an example, platelettype vWD, clinically very similar to type IIB vWD, is now
known to be due to a molecular defect in the GPIba chain
genes2 (see below). Indeed, genetic locus heterogeneity
could be partially responsible for the extensive phenotypic
heterogeneity observed in vWD. Such a mechanism could
also explain the apparent discordance between the relative
frequencies of type I and type 111 vWD; ie, if the true
incidence of type I vWD is 1%to 3%,61362this would imply a
gene frequency of 0.015 to 0.005, which should translate
into a homozygote frequency (expected to have severe
vWD) of 1:4,000 to 1:40,000, much greater than the observed frequency of approximately 1:1,000,000.56~60
Similarly, the “true autosomal” pattern of murine vWD might
also suggest a regulatory locus outside of the vWF gene.
In studies of porcine vWD, a restriction fragment length
polymorphism (RFLP) identified within the porcine vWF
gene was shown to be tightly linked to the inheritance of
vWD with a LOD score of 5.3 (at 0 = 0). Southern blot
analysis showed no evidence of gene deletion or rearrangement. Taken together, these observations suggest a point
mutation or small insertion or deletion within the vWF gene
as the molecular basis for porcine v W D . A
~ ~large number
of RFLPs have been identified within the human vWF gene,
including a highly polymorphic tetranucleotide repeat in
intron 40.83-85
For polymorphismslocated within the midportion of the vWF gene, care must be taken to distinguish
RFLPs within the authentic gene from pseudogene polymorp h i s m ~I . ~ ~ ~ ~
Linkage analysis of type I vWD is complicated by
problems inherent in the incomplete penetrance of this
disorder and low sensitivity and specificity of conventional
diagnostic tests. Tight linkage has been demonstrated for
two human type IIA vWD pedigrees (LOD scores of 3.68h
and 5.7*’). Although RFLP analyses in a number of other
vWD pedigrees have been consistent with linkage,s3,ss-94
none have individually obtained statistical significance (LOD
score > 3.0). Taken together with the recent identification
of specific vWF gene mutations in several groups of
patients, these data indicate that vWD is generally due to
defects within the vWD gene itself. With the exception of
platelet-type vWD, defects at other loci have not yet been
identified.
GENE DELETIONS IN vWD
Gene delection or rearrangement is a common mechanism for human genetic disease. Once DNA probes for
vWF became available, large numbers of patients were
screened by Southern blot analysis for the presence of such
a b n o r m a l i t i e ~ . ~ ~However,
’ * J ~ ~ ~ ~gene deletions have only
been reported in six families, associated with type 111 vWD
in five (Table 2).12J3,y5
The one exception is a patient with
an apparent de novo deletion in the midportion of the vWF
gene resulting in a type I1 vWD phenotype (Table 3).yh
Although the numbers are small, there appears to be a
correlation between the presence of vWF inhibitors (antivWF allo-antibody) and the presence of gene deletion.
Similar correlations have been noted in the hemophilias,
particularly hemophilia B.I2 Give the low incidence of type
I11 vWD (see above) and the presence of deletions in only a
small subset of these patients, this would appear to be a
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
VON WILLEBRAND DISEASE
251 1
Table 2. Type 111 vWD
Amino Acid
Substitution
No. of
Independent
Families Reference
Molecular
Defect
-
lg gene deletion (? entire gene)
lg gene deletion (? entire gene)
2.3 kb deletion (exon 42)
cis-defect i n vWF mRNA expression
Rpro365* C1093T
R1772’
C7603T
cis-defect in vWF mRNA expression
2
2
1
1
1
3t
3t
12
13
95
84
98
97
97
‘Termination codon.
t A l l 3 alleles have identical RFLP haplotypes.
rare mechanism for vWD. However, it is certainly possible
that some deletions have been missed due to the large size
of the vWF gene and cross-hybridization to the pseudogene.
Southern blots spanning the entire vWF gene are necessarily very complex and deletions involving only one vWF allele
could easily be missed, particularly in the region of the
pseudogene duplication. In the latter instance, deletion
would be manifested as only a 25% reduction in intensity of
the relevant bands. Although 50% dose reduction has been
detected by careful den~itometry,’~
such detailed quantitative analysis has not generally been performed on routine
Southern blots.
NONDELETION vWF DEFECTS IN TYPE 111 vWD
Once deletion has been excluded as a molecular mechanism, the search for subtle mutations resulting in quantitative decreases in vWF presents a formidable problem. Such
defects could lie anywhere within the 178-kb vWF gene (on
either of two alleles) or potentially in distant regulatory
sequences located hundreds of kilobases upstream or downstream of the gene. Direct sequence analysis of such a large
region of DNA is currently impractical. A method for
indentifying the presence of a subset of such defects has
recently been described.84In this approach, DNA sequence
polymorphisms, identified within vWF exons, are assessed
Table 3. Miscellaneous Defects
Amino Acid
Substitution
FVlll binding mutants
R19W
T28M
R53W
R91Q
Nucleotide
Substitution
No. of
Independent Functional
Families
Studies References
+
C2344T
C2372T
C2446T
G2561A
1
1
2
4
Gene deletion
(exons 26-34)
G3970A
T4105A
1
1
1
-
96
140
139
(GPlb a-chain)
(GPlb a-chain)
1
1
-
82
141
+132
+lX
+ 128.129
133
127,132
130,134
128-130
Other variants
G561S
F6061
Platelet type
(“pseudo-vWD)
G233V
M239V
+
by polymerase chain reaction (PCR) from both genomic
DNA and platelet vWF messenger RNA (mRNA). Any
molecular defect resulting in loss of vWF mRNA expression from one allele would result in detection of both alleles
at the level of genomic DNA but only the normal allele in
platelet mRNA. Defects that could be detected in this way
include any cis-acting mutation affecting mRNA transcription, nuclear processing, or mRNA stability. Given the
complexity of the vWF gene (51 introns), aberrant splicing
might present a particularly likely mechanism for vWD. By
this analysis, Nichols et als4 demonstrated defective vWF
mRNA expression from both maternal and paternal alleles
in one type I11 vWD pedigree. All offspring inheriting both
aberrant alleles were affected with type I11 vWD, whereas
both parents (obligate carriers) and five heterozygous
siblings were asymptomatic and had normal vWF plasma
levels. In additional preliminary studies, a similar “null”
allele has been identified in another type I11 vWD family.
Analysis in three type I vWD pedigrees demonstrated equal
expression of both vWF alleles (W.C. Nichols and D.
Ginsburg, unpublished data). In a preliminary report,
defective mRNA expression was detected from 2 different
alleles in the Dutch population by a similar approach, with
one allele also associated with a nonsense mutation.97 A
nonsense mutation has also been identified in another type
I11 vWD pedigree by screening 18 families at 2 potential
sites.98The currently identified molecular defects in type I11
vWD are summarized in Table 2.
TYPE 111 VERSUS TYPE I vWD
Type I11 and type I vWD are both quantitative defects,
the former characterized by total or near complete absence
of vWF and the latter by partial vWF reduction of 50% or
more. In the simplest model, these two disorders could be
viewed as the homozygous and heterozygous states for the
same defect. Mutations within the vWF gene resulting in
loss of expression would manifest as type I vWD in the
heterozygote and type I11 in the homozygote. In this model,
vWD would be more properly classified as an autosomal
codominant disorder. However, several lines of evidence
argue against this model. Although some investigators use
the term type I11 vWD synonymously with severe vWD,
others require clear autosomal recessive inheritance as a
condition for this classification. Of note, for the majority of
severely affected vWD patients, both parents, who would be
assumed to be obligate heterozygotes, are completely asymptomatic. In the three reported type 111 vWD gene deletion
fa mi lie^^*.*^^^^ and the nondeletion RNA expression defect
family,84parents, as well as sibling carrier, were all asymptomatic with essentially normal plasma vWF levels. Although there are occasional patients with type I11 vWD for
whom one or both parents appear to have a mild form of
vWD, this presentation is less common. Similarly, in the
animal models described above, two patterns seem to
emerge. The porcine model shows a recessive pattern of
inheritance quite similar to human type 111 vWD and by
linkage is due to a defect within the vWF gene.52 By
contrast, the murine model shows a pure dominant inheritance, potentially analogous to type I vWD, with both
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
2512
GINSBURG AND BOWlE
heterozygotes and presumed homozygotes having identical
vWD phenotypes.70 Taken together, these observations
suggest that type 111 and type I vWD may arise via different
molecular mechanisms.
Despite considerable progress in characterizing vWD
mutations in a variety of vWD subtypes, the molecular
defects responsible for type I vWD remain unknown. Gene
deletions, and presumably other defects resulting in complete loss of vWF expression from the vWF gene, appear to
result in recessive type I11 vWD. If loss of vWF expression
from one allele results in a silent carrier for type 111 vWD,
an alternative mechanism must be proposed for the autosomal pattern of type I vWD inheritance. Type I vWD could
be due to defects within the vWF gene giving rise to an
abnormal protein whose function interferes with the normal allele in a "dominant-negative'' manner. The multimeric nature of vWF provides a plausible mechanism for
such an interaction because an abnormal protein product
from one allele could affect not only its own secretion,
assembly, or function, but also the product of the normal
allele with which it forms heteromultimers. Similar interactions between mutant and normal a1 subunits in the
trimeric type I collagen molecule account for the autosomal
dominance of osteogenesis imperfecta type II.99 Alternatively, type I vWD could be due to a defect(s) at another
genetic locus, perhaps in a gene involved in vWF biosynthesis, processing, or secretion.
TYPE HA vWD
Identifying single point mutations within the vWF gene is
a difficult problem. As noted above, because of its large
size, direct sequence analysis of the entire vWF gene is not
currently a practical approach. Concentrating on qualitative vWF variants, in which a mutation within the coding
sequence might be expected, narrows the search to the
coding exons (or mRNA). DNA sequence analysis is also
complicated by the autosomal dominant nature of most
vWD variants, requiring distinction between the single
mutant allele and the other normal allele. In addition,
mutations located within the mid portion of the vWF gene
must be distinguished from the two pseudogene alleles. The
pseudogene problem can be circumvented by directly
analyzing vWF mRNA1" or, alternatively, using allelespecific PCR strategies to amplify only the authentic
gene.51,84,86JM)-102
The latter approach is facilitated by knowledge of the authentic and pseudogene sequences determined by Mancuso et al.50951
The first point mutations responsible for vWD were
reported for the type IIA variant.lo0 A 176-Kd proteolytic
fragment present in normal plasma and localized to the
C-terminus of the mature vWF subunit has been observed
to be markedly increased in the plasma of type IJA vWD
patients.Io3 A similar proteolytic fragment and the associated vWF multimer satellite bands were also shown to
result from proteolytic degradation in studies of cultured
human umbilical vein endothelial cells derived from a
patient with type IIA vWD.IM The hypothesis that increased sensitivity to proteolysis in the vicinity of a type IIA
vWD mutation might account for the 176-Kd fragment
focused attention on the corresponding segment of vWF in
exon 28. PCR sequence analysis of vWF mRNA obtained
from platelets or directly from exon 28 genomic DNA
sequences has led to the identification of a number of
mutations in type IIA vWD patients, generally all clustered
within the A2 homologous repeat (Table 4 and Fig 1).
Expression of mutant vWF sequences by transfection in
mammalian cells has provided important insights into the
molecular basis of type IIA vWD. Transfection results allow
subclassification of type IIA vWD patients into two distinct
s u b g r o ~ p s . In
~ ~group
J ~ ~ 1, the associated point mutation
leads to a defect in intracellular transport with vWF
observed to be retained within the endoplasmic reticul ~ m .In' ~the
~ heterozygous state, increased retention of the
larger multimers (more likely to contain one or more
variant subunits) could result in relatively more efficient
secretion of the smaller multimers, accounting for the
characteristic pattern observed in type IIAvWD plasma. By
contrast, expression of recombinant vWF from group 2
results in normal appearing vWF multimers in tissue
culture cells.105One of these mutations (Arg834 -+Trp)
has been identified on at least two distinct genetic backgrounds in six unrelated type IIA vWD patients DNAs
(Table 4).
The characteristic loss of large multimers in group 2
appears to occur via a second mechanism. Several studies
have reported that large multimer loss in some type IIA
vWD patients results from proteolysis occurring after
synthesis and secretion1MJ06-1w
mediated by a plasma or
platelet specific protease, possibly a calpain.lOsJ1O
The site
of proteolysis within vWF generating the characteristic
176-Kd fragment has recently been localized to Tyr842Met843, in close proximity to many of the identified type
IIA mutations (Table 4).lI0 A model for loss of large vWF
multimers as a result of this single proteolytic cleavage has
been proposed.I1l Collection of blood from some type IIA
patients into a cocktail of protease inhibitors results in
relative preservation of multimer s t r u c t ~ r e . This
~ ~ ~group
J~~
of patients may well correspond to the group 2 mutations.
In support of this hypothesis, a close correlation was
observed between preservation of vWF multimer structure
Table 4. Type IIA vWD Mutations
Amino Acid
Substitution
Nucleotide
Substitution
V551F
G742R
G742E
S743L
L777P
V802L
R834W
V844D
S850P
1865T
E875K
G3940T
G4513C
G4514A
C4517T
T4619C
G4693T
C4789T
T4820A
T4837C
T4883C
G4912A
No. of
Independent
Families
1
1
1
2
1
1
6*
1
1
1
1
Functional
Studies
-
+
+
+lo5
+".'O5
+
+
-
References
143
105
105
105,144
105
143
100,105,144,145
100,105
146
86
143
There are a total of 11 mutations in 17 families
*Greater than or equal to 2 independent alleles, based on haplotype
analysis.lo5
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
VON WILLEBRAND DISEASE
2513
in platelet vWF (protected from proteases within the
platelet a-granule) and expression of intact multimers in in
vitro transfection studies.105Interestingly, in 1983 Weiss et
a1 first suggested a subdivision of type IIA vWD based on
platelet multimer pattern,Il2 a subclassification that probably will correspond to the subgroups now suggested on the
basis of molecular pathogenesis.105The list of currently
reported potential type IIA mutations is shown in Table 4.
In all, 11 mutations have been identified in 17 families. In
one study, mutations were identified in 9 of 11 patients
studies.lo5 Thus, it is likely that a panel of mutations
accounting for the vast majority of type IIA vWD may
eventually be established, permitting accurate diagnosis
and classification at the DNA level for this common vWD
subtype.
TYPE llB vWD
Type IIB vWD is a relatively uncommon variant characterized by a unique “gain of function.” In this disorder,
vWF demonstrates an increased reactivity with its platelet
receptor GPIb, resulting in spontaneous vWF/platelet
interaction and subsequent clearance from the circulation.
The larger vWF multimers are more reactive with platelets
and are thus selectively cleared, resulting in the characteristic low molecular weight multimer pattern observed in type
IIB vWD plasma. Since the vWF GPIb binding domain had
been localized to a peptide fragment within vWF exon 28,
several groups have analyzed DNA sequence from type IIB
vWD patients, concentrating on this region. By this approach, seven specific single amino acid substitutions (and
one insertion) have been identified in type IIB vWD
patients (see Table 5) all clustered within a small segment
of the vWF A1 repeat (Fig 1). Expression of the Trp550 -+
Cys mutation in a recombinant vWF fragment resulted in
increased binding to platelets, consistent with the type IIB
vWD phenotype.Il3 Full-length recombinant vWF containing the Arg543
Trp mutation also demonstrated increased platelet binding, most marked for the large multimers, accounting for the characteristic vWF multimer
-
Table 5. Type llB vWD Mutations
No. of
Amino Acid Nucleotide Independent Functional
Substitution Substitution
Families
Studies
-
540insM 39lOinsATG
R543W C3916T
1
8*
R545C
W550C
V551L
V553M
P574L
R578Q
8t
-
1
I*
79
I
2
+
C3922T
G3939C
G3940C
G3946A
C4010T
G4022A
+114
-
+
+I15
References
147
101,102,114,117,119,144
101,102
113
119
101,102,117,120
116
101.115.117
There are a total of 7 mutations in 28families.
*Greater than or equal to two independent alleles based on haplotype analysis (in two different s t ~ d i e s ~ ~ ~ , ~ ~ ~ ) .
tGreater than or equal to three independent alleles based on
haplotype analysis.102
*New mutation.
§Greater than or equal to three independent alleles based o n
haplotype analysis, including two new m ~ t a t i o n s . ~ ~ ~ ~ ’ 1 ~
pattern observed in type IIB vWD plasma.Il4 Preliminaq
expression studies have also demonstrated increased platelet binding as a result of the Arg.578 + Gln and Pro574 +
Leu substitutions, confirming their identify as authentic
type IIB vWD m u t a t i o n ~ . ~ ~ ~ J l 6
Four mutations account for nearly 90% of the type IIB
vWD patients studied to date (Table 5). Several of these
mutations have been demonstrated to be recurrent independent genetic events on the basis of RFLP haplotype
analysis101,102
and in at least three cases, the amino acid
substitution appears to be a new m~tation.’~*J
l7-Il9 In one
of these cases, the mutation was shown to have originated
on one allele during the development of the germ-line in
the founder and was subsequently passed on to a subset of
his offspring inheriting that allele (germ-line mosaicism).lZ0
Five of the eight substitutions represent C + T transitions
at CpG dinucleotides, proposed hot spots for mutation
within the human genome.101J02Thus, in the case of type
IIB vWD, screening for a small panel of mutations should
have a high sensitivity for the detection of type IIB vWD,
and should facilitate precise diagnosis and classification of
this disorder at the DNA level.
vWF/FVlll INTERACTION AND AUTOSOMAL HEMOPHILIA
As discussed above, vWF and FVIII are closely associated in plasma as a noncovalent molecular complex. vWF is
critical for FVIII transport and stability in plasma and the
decreased vWF levels resulting from most vWD variants are
also generally associated with a proportional decrease in
FVIII antigen and procoagulant activity. In patients with
severe or type 111vWD, FVIII levels are markedly reduced
and contribute significantly to the resulting bleeding diathesis.56,58
The close association of vWF and FVIII led to initial
difficulties in distinguishing classic hemophilia A from
“pseudohemophilia” ( V W D ) . ’ . ~ ~ ~
Hemophilia A is an X-linked disorder due to mutations
within the FVIII gene on the X chromosome long arm. In
the past few years, over 100 distinct mutations responsible
for the hemophilia phenotype have been identified, most
through the use of PCR techniques.Iz1 Female patients
affected with hemophilia are rarely encountered, often
ascribed to unequal lyonization in a carrier. However, in
several pedigrees this unusual form of hemophilia appears
to be inherited in an autosomal f a s h i ~ n . In
~ ~several
~-~~~
cases, plasma vWF was demonstrated to have a markedly
decreased binding capacity for FVITI.124-126
One of these
original reports suggested the name vWD “Normandy”
(the patient’s province of origin) for vWF variants defined
by deficient FVIII binding without other qualitative or
quantitative a b n ~ r m a l i t i e s .With
~ ~ ~ the identification of
additional patients with similar defects from a number of
locations in the United States as well as Europe, a more
general terminology should probably be a d ~ p t e d . I ~ ~ - * ~ ’
Recently, specific mutations within the vWF genes have
been identified as the apparent explanation for the decreased vWF FVIII binding (Table 3). A single amino acid
substitution, Thr28 + Met, has been identified in one of the
original vWD “Normandy” p e d i g r e e ~ . l ~Recombinant
~J~~
vWF containing this substitution demonstrated markedly
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
2514
GINSBURG AND BOWIE
Some of these variants may represent compound heterozydecreased FVIII binding.132A study of three additional
gosity for other known subtypes. Preliminary reports of
patients with low FVIII levels (6% to 22%) identified a
potential mutations responsible for several rare variants
homozygote for an Arg91 + Gln substitution, a homozyhave recently appeared.139~140
gote for Arg53 + Trp, and a third patient who was a
compound heterozygote for both of these latter mutaSeveral families have been reported with a unique
t i o n ~The
. ~ Arg91~~
Gln mutation was also identified on 1
disorder termed platelet-type or “pseudo”-vWD. This condition is remarkably similar to type IIB vWD, with devWF allele in each of two unrelated mild type I vWD
patients with disproportionately low FVIII levels.128J29 creased large vWF multimers, thrombocytopenia, and increased vWF/platelet interaction. However, unlike type
Plasma vWF from one of these patients had previously been
shown to exhibit an abnormal interaction with FVIII.131
IIV vWD, in which the defect has been shown to lie within
the GPIb binding domain of vWF (Table 5), the defect in
Recombinant vWF containing the Arg91-+ Gln substitution demonstrated markedly decreased capacity for FVIII
platelet type vWD is in the platelet itself, specifically within
binding.128,L29
Interestingly, an amino acid polymorphism
the GPIb/IX complex. The two disorders can be distinwas identified on the other vWF allele from one of the type
guished by platelet and plasma mixing studies. Point mutaI patients,lZ9 located just 2 amino acids upstream and
tions within the GPIba chain gene potentially responsible
resulting in the similar substitution, Arg89 + Gln. Expresfor platelet-type vWD in two families have recently been
sion of vWF containing this latter substitution resulted in
reported (Table 3).82,141
FVIII binding indistinguishable from ~ i 1 d - t y p e . lThe
~~
PRENATAL DIAGNOSIS
functional significance of the Arg53 + Trp mutation, along
With the dramatic advances in our understanding of
with a fourth substitution (Argl9 + Trp) have also recently
genetics, powerful tools are now available
been confirmed by recombinant expression s t ~ d i e s . ~ ~ ~ vWD
, ~ ~ molecular
~
for
potential
prenatal
diagnosis. In those cases in which the
All of these vWF mutations are located within the
precise
molecular
defect
is known (Tables 2 through 5 ) ,
N-terminal portion of vWF, the region implicated in bindreliable
and
accurate
diagnosis
can easily be achieved from
ing to FVIII. As noted above, two independent monoclonal
amniotic fluid or chorionic villus biopsy by PCR techniques,
antibodies that block FVIII binding to vWF have been
as now regularly applied for a variety of genetic disorlocalized to a 19 amino acid peptide (Thr78-Thr96) with the
d e r ~ . As
~ ~noted
, ~ ~above,
~
a large number of polymorN-terminal ~ e g m e n t . *Interestingly,
~%~~
the Arg91 + Gln
phisms
within
the
vWF
gene
have now been identified
substitution is localized in the middle of this small epitope.
including a highly informative variable number tandem
Together, these data provide strong evidence that this
repeat (VNTR) in intron 40.83-85,xs,89
Using these markers,
region plays a critical role in the FVIII/vWF interaction.
prenatal
diagnosis
has
been
successfully
performed by
The corresponding segment within FVIII that binds vWF
genetic
linkage
a
n
a
l
y
s
i
~
.
However,
~
~
.
~
~
,
~
given
~
the potential
has been localized to an acidic peptide, spanning amino
for locus heterogeneity in vWD (ie, vWD resulting from
acids 1677 to 1684.135The Thr78-Thr96 epitope is markedly
defects in genes other than vWF; see above), caution should
basic, and the Arg91 substitution results in a loss of one of
be
exercised in interpreting these results.
these basic residues. However, the finding that Arg89 +
Gln has no effect on FVIII binding indicates that this
CONCLUSIONS
interaction is not simply based on charge.129
Since the cloning of vWF cDNA in 19857,xJ0,13
and
Thus, these mutations at the vWF N-terminus (Table 3)
characterization of the complete genomic structure of the
all interfere with the ability of vWF to bind FVIII and
vWF gene in 1989:O considerable progress has been made
define a new variant of vWD. In the homozygote (or
in characterizing the specific molecular defects responsible
compound heterozygote) this defect results in an autosomal
for the heterogeneous disorder known as vWD. A large
form of hemophilia characterized by decreased FVIII levels
number of specific molecular defects have now been identiand a clinical pattern indistinguishable from mild to moderfied and precise characterization may now be possible in the
ate classic hemophilia A.127J30,132J34
In the heterozygote,
majority of type IIA, type IIB, and potentially also type 111
this defect is generally silent and only detected by incidenvWD cases. However, the most common variant, type I
tal screening, or when it occurs in conjunction with a
vWD, still remains a major challenge. Continued progress
coexistent type I or other vWD variant.128J29s131J33
Coinherin this area will not only improve our understanding of the
itance of a FVIII binding defective vWF could account for
pathogenesis of vWD, but should also lead to more rapid
some of the phenotypic heterogeneity occasionally oband precise diagnosis and classification for this common
served among hemophilia A patients with identical FVIII
disorder. The problems of incomplete vWD penetrance and
gene m u t a t i o n ~ . ~ ~ ~ - ’ 3 ~
poor diagnostic sensitivity and accuracy for the currently
available clinical laboratory tests provide strong incentives
OTHER vWD VARIANTS
for the development of DNA-based diagnostics. In addition, prenatal diagnosis is now possible either at the level of
A large number of other vWD variants have been
single point mutations or by RFLP analysis (assuming
described, most as single case reports, generally identified
by subtle abnormalities in vWF multimeric structure (Table
linkage to the vWF gene) and will probably be applied with
l).I9 Diagnosis of these variants requires high quality
increasing frequency. Understanding the molecular basis of
mulimer analysis, generally available at only a few reference
vWD also has important implications for vWF structure and
function and is helping to define critical binding domains
laboratories. Thus, their frequency may be underestimated.
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
VON WILLEBRAND DISEASE
2515
within the vWF molecule. Insights gained from these
studies may
lead to improved therapeutic approaches not only for VWD, but for a variety of other
genetic and acquired hemorrhagic and thrombotic disorders.
ACKNOWLEDGMENT
We thank J.E. Sadler and members of our labs for thoughtful
comments and discussion and S.E. Labun for careful preparation
of the manuscript.
REFERENCES
1. von Willebrand EA: Hereditar Pseudohemofili. Finska
Lakarsallskapetes Hand1 67:7,1926
2. Minot GR, Lee RI: Miscellaneous hemorrhagic conditions, in
Nelson Loose-Leaf Medicine. New York, NY, Nelson & Sons,
1920, p 155
3. Bowie EJW, Didisheim P, Thompson JH Jr, Owen CA Jr: von
Willebrand’s disease: A critical review. Hematol Rev 1:1, 1968
4. Nilsson IM: In memory of Erik Jorpes. von Willebrand’s
disease from 1926-1983. Scand J Haematol Suppl40:21,1984
5. Gitschier J, Wood WI, Goralka TM, Wion KL, Chen EY,
Eaton DH, Vehar GA, Capon DJ, Lawn RM: Characterization of
the human factor VI11 gene. Nature 312:326,1984
6. Toole JJ, Knopf JL, Wozney JM, Sultzman LA, Buecker JL,
Pittman DD, Kaufman RJ, Brown E, Shoemaker C, Orr EC,
Amphlett GW, Foster WB, Coe ML, Knutson GJ, Fass DN,
Hewick RM: Molecular cloning of a cDNA encoding human
antihaemophilic factor. Nature 312:342, 1984
7. Ginsburg D, Handin RI, Bonthron DT, Donlon TA, Bruns
GAP, Latt SA, Orkin SH: Human von Willebrand factor (VWF):
Isolation of complementary DNA (cDNA) clones and chromosomal localization. Science 228:1401, 1985
8. Lynch DC, Zimmerman TS, Collins CJ, Brown M, Morin MJ,
Ling EH, Livingston DM: Molecular cloning of cDNA for human
von Willebrand factor: Authentication of a new method. Cell 41:49,
1985
9. Sadler JE, Shelton-Inloes BB, Sorace JM, Harlan JM, Titani
K, Davie EW: Cloning and characterization of two cDNAs coding
for human von Willebrand factor. Proc Natl Acad Sci USA
82:6394,1985
10. Verweij CL, de Vries CJM, Distel B, van Zonneveld A-J, van
Kessel AG, van Mourik JA, Pannekoek H: Construction of cDNA
coding for human von Willebrand factor using antibody probes for
colony-screening and mapping of the chromosomal gene. Nucleic
Acids Res 13:4699,1985
11. Gitschier J, Wood WI, Tuddenham EGD, Shuman MA,
Goralka TM, Chen EY, Lawn RM: Detection and sequence of
mutations in the factor VI11 gene of haemophiliacs. Nature
315:427,1985
12. Shelton-Inloes BB, Chehab FF, Mannucci PM, Federici AB,
Sadler JE: Gene deletions correlate with the development of
alloantibodies in von Willebrand disease. J Clin Invest 79:1459,
1987
13. Ngo KY, Glotz VT, Koziol JA, Lynch DC, Gitschier J,
Ranieri P, Ciavarella N, Ruggeri ZM, Zimmerman TS: Homozygous and heterozygous deletions of the von Willebrand factor gene
in patients and carriers of severe von Willebrand disease. Proc Natl
Acad Sci USA 85:2753,1988
14. Saiki RK, Gelfand DH, Stoffel S, Scharf SJ, Higuchi R, Horn
GT, Mullis KB, Erlich HA: Primer-directed enzymatic amplification of DNA with a thermostable DNA polymerase. Science
239:487, 1988
15. Kogan SC, Doherty M, Gitschier J: An improved method for
prenatal diagnosis of genetic diseases by analysis of amplified DNA
sequences. N Engl J Med 317:985,1987
16. Wagner DD: Cell biology of von Willebrand factor. Annu
Rev Cell Biol6:217, 1990
17. Ruggeri ZM, Zimmerman TS: von Willebrand factor and
von Willebrand disease. Blood 702395,1987
18. Girma J-P, Meyer D, Verweij CL, Pannekoek H, Sixma JJ:
Structure-function relationship of human von Willebrand factor.
Blood 70:605,1987
19. Ruggeri ZM: Structure and function of von Willebrand
factor: Relationship to von Willebrand’s disease. May Clin Proc
66:847, 1991
20. Sadler JE: von Willebrand factor. J Bil Chem 266:22777,
1991
21. Bonfanti R, Furie BC, Furie B, Wagner DD: PADGEM
(GMP140) is a component of Weibel-Palade bodies of human
endothelial cells. Blood 73:1109, 1989
22. McEver RP, Beckstead JH, Moore KL, Marshall-Carlson L,
Bainton D: GMP-140, a platelet a-granule membrane protein, is
also synthesized by vascular endothelial cells and is localized in
Weibel-Palade bodies. J Clin Invest 84:92, 1989
23. Foster PA, Fulcher CA, Marti T, Titani K, Zimmerman TS:
A major factor VI11 binding domain resides within the aminoterminal 272 amino acid residues of von Willebrand factor. J Biol
Chem 262:8443,1987
24. Takahashi Y, Kalafatis M, Girma J-P, Sewerin K, Anderson
LO, Meyer D: Localization of a factor VI11 binding domain on a 34
kilodalton fragment of the N-terminal portion of von Willebrand
factor. Blood 70:1679, 1987
25. Bahou WF, Ginsburg D, Sikkink R, Litwiller R, Fass DN: A
monoclonal antibody to von Willebrand factor (vWF) inhibits
factor VI11 binding. Localization of its antigenic determinant to a
nonadecapeptide at the amino terminus of the mature vWF
polypeptide. J Clin Invest 8456, 1989
26. Ginsburg D, Bockenstedt PL, Allen EA, Fox DA, Foster
PA, Ruggeri ZM, Zimmerman TS, Montogomery RR, Bahou WF,
Johnson TA, Yang AY: Fine mapping of monoclonal antibody
epitopes on human von Willebrand factor using a recombinant
peptide library. Thromb Haemost 67:166,1991
27. Wise RJ, Dorner AJ, Krane M, Pittman DD, Kaufman RJ:
The role of von Willebrand factor multimers and propeptide
cleavage in binding and stabilization of factor VIII. J Biol Chem
266:21948,1991
28. Leyte A, Voorberg J, van Schijndel HB, Duim B, Pannekoek
H, van Mourik JA: The pro-polypeptide of von Willebrand factor is
required for the formation of a functional factor VIII-binding site
on mature von Willebrand factor. Biochem J 274:257,1991
29. Fujimura Y, Titani K, Holland LZ, Russell SR, Roberts JR,
Elder JH, Ruggeri ZM, Zimmerman TS: von Willbrand factor: A
reduced and alkylated 52/48-kDa fragment beginning at amino
acid residue 449 contains the domain interacting with platelet
glycoprotein Ib. J Biol Chem 261:381, 1986
30. Fujimura Y, Titani K, Holland LZ, Roberts JR, Kostel P,
Ruggeri ZM, Zimmerman TS: A heparin-binding domain of
human von Willebrand factor. J Biol Chem 262:1734,1987
31. Mohri H, Fujimura Y, Shima M, Yoshioka A, Houghten RA,
Ruggeri ZM, Zimmerman TS: Structure of the von Willebrand
factor domain interacting with glycoprotein Ib. J Biol Chem
263:17901,1988
32. Pareti N, Niiya K, McPherson JM, Ruggeri ZM: Isolation
and characterization of two domains of human von Willebrand
factor that interact with fibrillar collagen types I and 111. J Biol
Chem 262:13835,1987
33. Roth GJ, Titani K, Hoyer LW, Hickey MJ: Localization of
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
2516
binding sites within human von Willebrand factor for monomeric
type 111 collagen. Biochemistry 25:8357,1986
34. Titani K, Kumar S, Takio K, Ericsson LH, Wade RD, Sahida
K, Walsh KA, Chopek MW, Sadler JE, Fujikawa K Amino acid
sequence of human von Willebrand factor. Biochemistry 25:3171,
1986
35. Bonthron DT, Handin RI, Kaufman RJ, Wasley LC, Orr
EC, Mitsock LM, Ewenstein B, Lmcalzo J, Ginsburg D, Orkin SH:
Structure of pre-pro-von Willebrand factor and its expression in
heterologous cells. Nature 324:270,1986
36. Bonthron DT, Orr EC, Mitsock LM, Ginsburg D, Handin
RI, Orkin SH: Nucleotide sequence of pre-pro-von Willebrand
factor cDNA. Nucleic Acids Res 14:7125,1986
37. Shelton-Inloes BB, Broze GJ Jr, Miletich JP, Sadler JE:
Evolution of human von Willebrand factor: cDNA sequence
polymorphisms, repeated domains, and relationship to von Willebrand antigen 11. Biochem Biophys Res Commun 144:657,1987
38. Shelton-Inloes BB, Titani K, Sadler E: cDNA sequences for
human von Willebrand factor reveal five types of repeated domains
and five possible protein sequence polymorphisms. Biochemistry
25:3164, 1986
39. Venveij CL, Diergaarde PJ, Hart M, Pannekoek H: Fulllength von Willebrand factor (vWF) cDNA encodes a highly
repetitive protein considerably larger than the mature vWF subunit. EMBO J 51839,1986
40. Fay PJ, Kawai Y, Wagner DD, Ginsburg D, Bonthron D,
Ohlsson-Wilhelm BM, Chavin SI, Abraham GN, Handin RI, Orkin
SH, Montgomery RR, Marder VJ: Propolypeptide of von Willebrand factor circulates in blood and is identical to von Willebrand
antigen 11. Science 232:995, 1986
41. Montgomery RR, Zimmerman TS: von Willebrand’s disease
antigen 11. J Clin Invest 61:1498,1978
42. Verweij CL, Hart M, Pannekoek H: Expression of variant
von Willebrand factor (vWF) cDNA in heterologous cells: Requirement of the pro-polypeptide in vWF multimer formation. EMBO J
6:2885,1987
43. Wise RJ, Pittman DD, Handin RI, Kaufman RJ, Orkin SH:
The propeptide of von Willebrand factor independently mediates
the assembly of von Willebrand multimers. Cell 52:229,1988
44. Venveij CL, Hart M, Pannekoek H: Proteolytic cleavage of
the precursor of von Willebrand factor is not essential for multimer
formation. J Biol Chem 263:7921, 1988
45. Wagner DD, Saffaripour S, Bonfanti R, Sadler JE, Cramer
EM, Chapman B, Mayadas TN: Induction of specific storage
organelles by von Willebrand factor propolypeptide. Cell 64:403,
1991
46. Wise RJ, Barr PJ, Wong PA, Kiefer MC, Brake AJ,
Kaufman RJ: Expression of a human proprotein processing enzyme: Correct cleavage of the von Willebrand factor precursor at a
paired basic amino acid site. Proc Natl Acad Sci USA 87:9378,1990
47. Colombatti A, Bonaldo P: The superfamily of proteins with
von Willebrand factor type A-like domains: One theme common to
components of extracellular matrix, hemostasis, cellular adhesion,
and defense mechanisms. Blood 77:2305,1991
48. Hunt LT, Barker WC: von Willebrand factor shares a
distinctive cysteine-rich domain with thrombospondin and procollagen. Biochem Biophys Res Commun 1445376,1987
49. Patracchini P, Calzolari E, Aiello V, Palazzi P, Banin P,
Marchetti GB: Sublocalization of von Willebrand factor pseudogene
to 22q11.22-q11.23 by in situ hybridization in a 46,X,t(X,22)(pter;
q11.21) translocation. Hum Genet 83:264,1989
50. Mancuso DJ, Tuley EA, Westfield LA, Worrall NK, SheltonInloes BB, Sorace JM, Alevy YG, Sadler JE: Structure of the gene
for human von Willebrand factor. J Biol Chem 264:19514,1989
GINSBURG AND BOWIE
51. Mancuso DJ, Tuley EA, Westfield LA, Lester-Mancuso TL,
Le Beau MM, Sorace JM, Sadler J E Human von Willebrand factor
gene and pseudogene: Structural analysis and differentiation by
polymerase chain reaction. Biochemistry 30:253,1991
52. Bahou WF, Bowie EJW, Fass DN, Ginsburg D: Molecular
genetic analysis of porcine von Willebrand disease: Tight linkage to
the von Willebrand factor locus. Blood 72:308,1988
53. Collins CJ, Underdahl JP, Levene RB, Ravera CP, Morin
MJ, Dombalagian MJ, Ricca G , Livingston DM, Lynch D C
Molecular cloning of the human gene for von Willebrand factor
and identification of the transcription initiation site. Proc Natl
Acad Sci USA 84:4393,1987
54. Bonthron D, Orkin SH: The human von Willebrand factor
gene: Structure of the 5’ region. Eur J Biochem 17151,1988
55. Berkowitz SD, Ruggeri ZM, Zimmerman TS: von Willebrand disease, in Zimmerman TS, Ruggeri ZM (eds): Coagulation
and Bleeding Disorders. The Role of Factor VI11 and von
Willebrand Factor. New York, NY,Marcel Dekker, 1989, p 215
56. Bloom A L von Willebrand factor: Clinical features of
inherited and acquired disorders. Mayo Clin Proc 66:743,1991
57. Aledort LM: Treatment of von Willebrand’s disease. Mayo
Clin Proc 66:841,1991
58. Triplett DA: Laboratory diagnosis of von Willebrand’s
disease. Mayo Clin Proc 66:832,1991
59. Holmberg L, Nilsson IM: von Willebrand disease. Clin
Haematol 14:461,1985
60. Weiss HJ, Ball AP,Mannucci PM: Incidence of severe von
Willebrand’s disease. N Engl J Med 307:127, 1982
61. Rodeghiero F, Castaman G, Dini E: Epidemiological investigation of the prevalence of von Willebrand’s disease. Blood 69:454,
1987
62. Miller CH, Lenzi R, Breen C: Prevalence of von Willebrand’s disease among U.S. adults. Blood 70:377a, 1987 (abstr,
SUPPI 1)
63. Miller CH, Graham JB, Goldin LR, Elston RC: Genetics of
classic von Willebrand’s disease. I. Phenotypic variation within
families. Blood 54:117,1979
64. Gill JC, Endres-Brooks J, Bauer PJ, Marks WJ, Montgomery
RR: The effect of A B 0 blood group on the diagnosis of von
Willebrand disease. Blood 69:1691, 1987
65. Orstavik KH, Kornstad L, Reisner H, Berg K Possible effect
of secretor locus on plasma concentration of factor VI11 and von
Willebrand factor. Blood 73:990,1989
66. Rose EH, Aledort LM: Nasal spray desmopressin (DDAVP)
for mild hemophilia A and von Willebrand disease. Ann Intern
Med 114:563,1991
67. Holmberg L, Nilsson IM, Borge L, Gunnarsson M, Sjorin E.
Platelet aggregation induced by 1-desamino-8-D-arginine vasopressin (DDAVP) in type IIB von Willebrand’s disease. N Engl J
Med 309:816,1983
68. Casonato A, Sartori MT, De Marco L, Girolami A: 1-Desamino-8-D-arginine vasopressin (DDAVP) infusion in type IIB
von Willebrand’s disease: Shortening of bleeding time and induction of a variable pseudothrombocytopenia. Thromb Haemost
64:117,1990
69. Johnson GS, Turrentine MA, Kraus KH: Canine von Willebrand’s disease A heterogeneous group of bleeding disorders. Vet
Clin North Am Small Anim Pract 18:195,1988
70. Sweeney JD, Novak EK, Reddington M, Takeuchi KH,
Swank R T The RIIISiJ inbred mouse strain as a model for von
Willebrand disease. Blood 76:2258,1990
71. Brooks M, Leith GS, Allen AK, Woods PR, Benson RE,
Dodds W L Bleeding disorder (von Willebrand disease) in a
quarter horse. J Am Vet Med Assoc 198:114,1991
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
VON WILLEBRAND DISEASE
72. Brinkhous KM, Reddick RL, Read MS, Nichols TC, Bellinger DA, Griggs TR: von Willebrand factor and animal models:
Contributions to gene therapy, thrombotic thrombocytopenic purpura, and coronary artery thrombosis. Mayo Clin Proc 66:733,1991
73. Fass DN, Bowie EJW, Owen CA, Zollman PE: Inheritance
of porcine von Willebrand’s disease: Study of a kindred of over 700
pigs. Blood 53:712,1979
74. Bowie EJW, Owen CA Jr, Giles AR: Animal models for the
study of factor VI11 and von Willebrand factor, in Zimmerman TS,
Ruggeri ZM (eds): Coagulation and Bleeding Disorders. New
York, NY,Marcel Dekker, 1989, p 305
75. Fuster V, Badimon L, Badimon JJ, Ip JH, Chesebro J H The
porcine model for the understanding of thrombogenesis and
atherogenesis. Mayo Clin Proc 66:818,1991
76. Gunby P: Do von Willebrand victims have less plaque?
JAMA 244:2400, 1980
77. Johnson CM, Stewart M, Zoecklein LJ, Bowie EJW: Pigs
with von Willebrand’s disease are resistant to the development of
experimental infective endocarditis. Thromb Haemost 62:34, 1989
(abstr)
78. Leung KY, Straley SC: The yopM gene of Yersinia pestis
encodes a released protein having homology with the human
platelet surface protein GPIba. J Bacteriol 171:4623,1989
79. Leung KY, Reisner BS, Straley SC: YopM inhibits platelet
aggregation and is necessary for virulence of Yersinia pestis in
mice. Infec Immun 58:3262,1990
80. Monaco AF’,Kunkel LM: Cloning of the Duchenne/Becker
muscular dystrophy locus. Adv Hum Genet 17:61, 1988
81. Vogel F, Motulsky AG: Population genetics, in Human
Genetics Problems and Approaches. New York, NY, SpringerVerlag, 1986, p 447
82. Miller JL, Cunningham D, Lyle VA, Finch CN: Mutation in
the gene encoding the a chain of platelet glycoprotein Ib in
platelet-type von Willebrand disease. Proc Natl Acad Sci USA
88:4761,1991
83. Peake IR, Bowen D, Bignell P, Liddell MB, Sadler JE,
Standen G, Bloom A L Family studies and prenatal diagnosis in
severe von Willebrand disease by polymerase chain reaction
amplification of a variable number tandem repeat region of the von
Willebrand factor gene. Blood 76555, 1990
84. Nichols WC, Lyons SE, Harrison JS, Cody RL, Ginsburg D:
Severe von Willebrand disease due to a defect at the level of von
Willebrand factor mRNA expression: Detection by exonic PCRrestriction fragment length polymorphism analysis. Proc Natl Acad
Sci USA 88:3857,1991
85. Ploos van Amstel HK, Reitsma PH: Tetranucleotide repeat
polymorphism in the vWF gene. Nucleic Acids Res 18:4957, 1990
86. Iannuzzi MC, Hidaka N, Boehnke ML, Bruck ME, Hanna
WT, Collins FS, Ginsburg D: Analysis of the relationship of von
Willebrand disease (vWD) and hereditary hemorrhagic telangiectasia and identification of a potential type IIA vWD mutation (IIe865
to Thr). A m J Hum Genet 48:757,1991
87. Venveij CL, Quadt R, Briet E, Dubbeldam K, van Ommen
GB, Pannekoek H: Genetic linkage of two intragenic restriction
fragment length polymorphisms with von Willebrand’s disease type
IIA. J Clin Invest 81:1116, 1988
88. Bignell P, Standen GR, Bowen DJ, Peake IR, Bloom AL:
Rapid neonatal diagnosis of von Willebrand’s disease by use of the
polymerase chain reaction. Lancet 336:638, 1990
89. Standen GR, Bignell P, Bowen DJ, Peake IR, Bloom AL:
Family studies in von Willebrand’s disease by analysis of restriction
fragment length polymorphisms and an intragenic variable number
tandem repeat (VNTR) sequence. Br J Haematol76:242,1990
90. Bernardi F, Marchetti G, Casonato A, Gemmati D, Patracchini P, Legnani C, DeRosa V, Girolami A, Conconi F: Character-
2517
ization of polymorphic markers in the von Willebrand factor gene
and pseudogene. Br J Haematol74:282,1990
91. Caekebeke-Peerlinck K, Bakker E, Britt E: An infrequent
DNA polymorphism associated with severe von Willebrand’s
disease. Br J Haematol75:78,1990
92. Bernardi F, Guerra S, Patracchini P, Volinia S, Buzzoni D,
Ballerini G, Casonato A, Marchetti G: von Willebrand disease
investigated by two novel RFLPs. Br J Haematol68:243,1988
93. Bahnak BR, Lavergne J-M, Venveij CL, Rothschild C,
Pannekoek H, Larrieu M-J, Meyer D: Carrier detection in severe
(type 111) von Willebrand disease using two intragenic restriction
fragment length polymorphisms. Thromb Haemost 60: 178,1988
94. Mannhalter C, Kyrle PA, Brenner B, Lechner K: Rapid
neonatal diagnosis of type IIB von Willebrand disease using the
polymerase chain reaction. Blood 77:2538,1991
95. Peake IR, Liddell MB, Moodie P, Standen G, Mancuso DJ,
Tuley EA, Westfield LA, Sorace JM, Sadler JE, Venveij CL,
Bloom AL: Severe type 111 von Willebrand’s disease caused by
deletion of Exon 42 of the von Willebrand factor gene: Family
studies that identify carriers of the condition and a compound
heterozygous individual. Blood 75:654,1990
96. Bernardi F, Marchetti G, Guerra S, Casonato A, Gemmati
D, Patracchini P, Ballerini G, Conconi F: A de novo and heterozygous gene deletion causing a variant of von Willebrand disease.
Blood 75:677,1990
97. Eikenboom JCJ, Britt E, Reitsma PH, Ploos van Amstel
H K Severe type 111 von Willebrand’s disease in the Dutch
population is often associated with the absence of von Willebrand
factor messenger RNA. Thromb Haemost 65:1127, 1991 (abstr)
98. Bahnak BR, Lavergne J-M, Rothschild C, Meyer D: A stop
codon in a patient with severe, type 111, von Willebrand disease.
Blood 78:1148,1991
99. Prockop DJ: Mutations that alter the primary structure of
type I collagen. The perils of a system for generating large
structures by the principle of nucleated growth. J Biol Chem
265:15349,1990
100. Ginsburg D, Konkle BA, Gill JC, Montgomery RR, Bockenstedt PL, Johnson TA, Yang A Y Molecular basis of human von
Willebrand disease: Analysis of platelet von Willebrand factor
mRNA. Proc Natl Acad Sci USA 86:3723,1989
101. Cooney KA, Nichols WC, Bruck ME, Bahou WF, Shapiro
AD, Bowie EJW, Gralnick HR, Ginsburg D: The molecular defect
in type IIB von Willebrand disease: Identification of four potential
missense mutations within the putative GpIb binding domain. J
Clin Invest 87:1227,1991
102. Randi AM, Rabinowitz I, Mancuso DJ, Mannucci PM,
Sadler JE: Molecular basis of von Willebrand disease type IIB.
Candidate mutations cluster in one disulfide loop between proposed platelet glycoprotein Ib binding sequences. J Clin Invest
87:1220, 1991
103. Berkowitz SD, Dent J, Roberts J, Fujimura Y, Plow EF,
Titani K, Ruggeri ZM, Zimmerman TS: Epitope mapping of the
von Willebrand factor subunit distinguishes fragments present in
normal and type IIA von Willebrand disease from those generated
by plasmin. J Clin Invest 79524,1987
104. Levene RB, Booyse FM, Chediak JR, Zimmerman TS,
Livingston DM, Lynch DC: Expression of abnormal von Willebrand factor by endotheolial cells from a patient with type IIA von
Willebrand disease. Proc Natl Acad Sci USA 84:6550,1987
105. Lyons SE, Bruck ME, Bowie EJW, Ginsburg D: Impaired
intracellular transport produced by a subset of type IIA von
Willebrand disease mutations. J Biol Chem 267:4424, 1992
106. Gralnick HR, Williams SB, McKeown LP, Maisonneuve P,
Jenneau C, Sultan Y , Rick M E In vitro correction of the abnormal
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
2518
multimeric structure of von Willebrand factor in type IIA von
Willebrand’s disease. Proc Natl Acad Sci USA 82:5968,1985
107. Batlle J, Lopez Fernandez MF, Campos M, Justica B,
Berges C, Navarro JL, Diaz Cremades JM, Kasper CK, Dent JA,
Ruggeri ZM, Zimmerman TS: The heterogeneity of type IIA von
Willebrand’s disease: Studies with protease inhibitors. Blood
68:1207,1986
108. Kunicki TJ, Montgomery RR, Schullek J: Cleavage of
human von Willebrand factor by platelet calcium-activated protease. Blood 65:352,1985
109. Zimmerman TS, Dent JA, Ruggeri ZM, Hannini LH:
Subunit composition of plasma von Willebrand factor. J Clin Invest
77:947, 1986
110. Dent JA, Berkowitz SD, Ware J, Kasper CK, Ruggeri ZM:
Identification of a cleavage site directing the immunochemical
detection of molecular abnormalities in type IIA von Willebrand
factor. Proc Natl Acad Sci USA 87:6306,1990
111. Dent JA, Galbusera M, Ruggeri ZM: Heterogeneity of
plasma von Willebrand factor multimers resulting from proteolysis
of the constituent subunit. J Clin Invest 88:774,1991
112. Weiss HJ, Pietu G, Rabinowitz R, Girma J-P, Rogers J,
Meyer D: Heterogeneous abnormalities in the multimeric structure, antigenic properties, and plasma-platelet content of factor
VIIIivon Willebrand factor in subtypes of classic (type I) and
variant (type IIA) von Willebrand’s disease. J Lab Clin Med
101:411,1983
113. Ware J, Dent JA, Azuma H, Sugimoto M, Kyrle PA,
Yoshioka A, Ruggeri ZM. Identification of a point mutation in
type IIB von Willebrand disease illustrating the regulation of von
Willebrand factor affinity for the platelet membrane glycoprotein
Ib-IX receptor. Proc Natl Acad Sci USA 88:2946,1991
114. Cooney KA, Lyons SE, Ginsburg D: Functional analysis of
a type IIB von Willebrand disease missense mutation: Increased
binding of large von Willebrand factor multimers to platelets. Proc
Natl Acad Sci USA 89:2869,1992
115. Randi AM, Tuley EA, Jorieux S, Rabinowitz I, Sadler JE:
A missense mutation (R578Q) in von Willebrand disease (vWD)
type IIB affects von Willebrand factor (vWF) binding to GPIB but
not to collagen or heparin: Studies with recombinant vWF. Blood
78:179a, 1991 (abstr, suppl 1)
116. Kroner PA, Kluessendorf ML, Scott JP, Montgomery RR:
A
-+ LEU substitution in von Willebrand factor enhances
the binding of expressed protein to platelets and is linked to type
IIB von Willebrand’s disease. Thromb Haemost 65:763, 1991
(abstr)
117. Murray EW, Giles AR, Lillicrap D: Recurring mutations at
CpG dinucleotides and germ line mosaicism in the von Willebrand
factor (vWF) gene as a cause of type IIB von Willebrand’s disease
(vWD). Am J Hum Genet 49:4:199,1991 (abstr)
118. Murray EW, Giles AR, Bridge PJ, Peake IR, Lillicrap DP:
Cosegregation of von Willebrand factor gene polymorphisms and
possible germinal mosaicism in type IIB von Willebrand disease.
Blood 77:1476,1991
119. Holmberg L, Donner M, Dahlback B, Nilsson IM: Apparently recessive IIB von Willebrand disease (vWD) is caused by de
novo mutations (ARG543+ TRP; VAL551+ LEU). Blood 78:
150a, 1991 (abstr, suppl 1)
120. Murray EW, Giles AR, Lillicrap D: Germ-line mosaicism
for a valine-to-methionine substitution at residue 553 in the
glycoprotein Ib-binding domain of von Willebrand factor, causing
type IIB von Willebrand disease. Am J Hum Genet 50:199,1992
121. Furie B, Furie BC: Molecular basis of hemophilia. Semin
Hematol27:270,1990
122. Veltkamp JJ, van Tilburg NH: Autosomal haemophilia: A
variant of von Willebrand’s disease. Br J Haematol26:141,1974
GINSBURG AND BOWlE
123. Graham JB, Barrow ES, Roberts HR, Webster WP, Blatt
PM, Buchanan P, Cederbaum AI, Allain JP, Barrett DA, Gralnick
HR: Dominant inheritance of hemophilia A in three generations of
women. Blood 46:175,1975
124. Mazurier C, Gaucher C, Jorieux S, Parquet-Gernez A,
Goudemand M: Evidence for a von Willebrand factor defect in
factor VI11 binding in three members of a family previously
misdiagnosed mild haemophilia A and haemophilia A carriers:
Consequences for therapy and genetic counselling. Br J Haematol
76:372, 1990
125. Mazurier C, Dieval J, Jorieux S, Delobel J, Goudemand M:
A new von Willebrand factor (vWF) defect in a patient with factor
VI11 (FVIII) deficiency but with normal levels and multimeric
patterns of both plasma and platelet vWF. Characterization of
abnormal vWFiFVIII interaction. Blood 75:20,1990
126. Nishino M, Girma J-P, Rothschild C, Fressinaud E, Meyer
D: New variant of von Willebrand disease with defective binding to
factor VIII. Blood 74:1591, 1989
127. Gaucher C, Jorieux S, Mercier B, Oufkir D, Mazurier C
The “Normandy” variant of von Willebrand disease: Characterization of a point mutation in the von Willebrand factor gene. Blood
77:1937,1991
128. Kroner PA, Friedman KD, Fahs SA, Scott JP, Montgomery
RR: Abnormal binding of factor VI11 is linked with the substitution
of glutamine for Arginine 91 in von Willebrand factor in a variant
form ofvon Willebrand disease. J Biol Chem 266:19146,1991
129. Cacheris PM, Nichols WC, Ginsburg D: Molecular characterization of a unique von Willebrand disease variant. A novel
mutation affecting von Willebrand factorifactor VI11 interaction. J
Biol Chem 266:13499,1991
130. Gaucher C, Mercier B, Jorieux S, Oufkir D, Mazurier C:
Identification of two point mutations in the von Willebrand factor
gene of three families with the ‘Normandy’ variant of von Willebrand disease. Br J Haematol78:506,1991
131. Montgomery RR, Hathaway WE, Johnson J, Jacobson L,
Muntean W A variant of von Willebrand’s disease with abnormal
expression of factor VI11 procoagulant activity. Blood 60:201,1982
132. Tuley EA, Gaucher C, Jorieux S, Worrall NK, Sadler JE,
Mazurier C: Expression of von Willebrand factor “Normandy”: A n
autosomal mutation that mimics hemophilia A. Proc Natl Acad Sci
USA 88:6377,1991
133. Kroner PA, Fahs SA, Vokac EA, Friedman KD, Montgomery RR: Novel missense mutations in von Willebrand factor (vWF)
associated with defective vWFifactor VI11 interaction in a patient
with type I von Willebrand disease. Blood 78:178a, 1991 (abstr,
SUPPI 1)
134. Jorieux S, Tuley EA, Gaucher C, Mazurier C, Sadler JE:
The mutation Arg(53) -+ Trp causes von Willebrand disease Normandy by abolishing binding to factor VIII. Studies with recombinant von Willebrand factor. Blood 79563,1992
135. Foster PA, Fulcher CA, Houghten RA, Zimmerman TS: A
synthetic factor VI11 peptide of eight amino acid residues (16771684) contains the binding region of anti-factor VI11 antibody
which inhibits the binding of factor VI11 to von Willebrand factor.
Thromb Haemost 63:403,1990
136. Schwaab R, Ludwig M, Oldenburg J, Brackmann HH, Egli
H, Kochhan L, Olek K Identical point mutations in the factor VI11
gene that have different clinical manifestations of hemophilia A.
Am J Hum Genet 47:743,1990
137. Arai M, Higuchi M, Antonarakis SE, Kazazian HH Jr,
Phillips JA 111, Janco RL, Hoyer LW: Characterization of a
thrombin cleavage site mutation (Arg 1689 to Cys) in the factor
VIII gene of two unrelated patients with cross-reacting materialpositive hemophilia A. Blood 75:384,1990
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
VON WILLEBRAND DISEASE
138. Levinson B, Lehesjoki A-E, de la Chapelle A, Gitschier J:
Molecular analysis of hemophilia A mutations in the Finnish
population. Am J Hum Genet 4653,1990
139. Mancuso DJ, Montgomery RR, Adam P: The identification
of a candidate mutation in the von Willebrand factor gene of
patients with a variant form of type I von Willebrand disease.
Blood 78:67a, 1991 (abstr, suppl 1)
140. Rabinowitz I, Mancuso DJ, Tuley EA, Randi AM, Firkin
BG, Howard MA, Sadler JE: von Willebrand disease (vWD) type
B, a variant with absent ristocetin- but normal botrocetin-cofactor
activity, is caused by a missense mutationin the GPIB binding
domain of von Willebrand factor (vWF). Blood 78:179a, 1991
(abstr, suppl 1)
141. Russell SD, Roth GJ: A mutation in the platelet glycoprotein (GP) Ib alpha gene associated with pseudo-von Willebrand
disease. Blood 78:281a, 1991 (abstr, suppl 1)
142. Antonarakis SE: Diagnosis of genetic disorders at the DNA
level. N Engl J Med 320:153, 1989
143. Lavergne JM, Ribba AS, Bahnak BR, de Pailette L, Derlon
A, Meyer D, PiCtu G: The use of denaturing gradient gel
electrophoresis to detect base changes in the von Willebrand factor
2519
gene from type IIA von Willebrand disease patients. Thromb
Haemost 65738,1991 (abstr)
144. Sugiura I, Matsushita T, Tanimoto M, Takamatsu J, Kamiya T, Saito H, Furuya H, Kat0 Y: The molecular defects in
Japanese patients with type I1 von Willebrand disease. Thromb
Haemost 65:763,1991 (abstr)
145. Bowen DJ, Standen GR, Bignell P, Peake IR: A C-T
transition in the gene for von Willebrand factor effects the
replacement of ARG 1597 (CGG) with TRP (TGG) in affected
members of a family with type IIA von Willebrand’s disease. Br J
Haematol76:36, 1990 (abstr, suppl 1)
146. Chang H-Y, Chen Y-P, Chediak JR, Levene RB, Lynch
DC: Molecular analysis of von Willebrand factor produced by
endothelial cell strains from patients with type IIA von Willebrand
disease. Blood 74:482a, 1989 (abstr, suppl 1)
147. Ribba AS, Lavergne JM, Bahnak BR, Derlon A, P i h G,
Meyer D: Duplication of a methionine within the glycoprotein Ib
binding of von Willebrand factor detected by denaturing gradient
gel electrophoresis in a patient with type IIB von Willebrand
disease. Blood 78:1738,1991
From www.bloodjournal.org by guest on August 3, 2017. For personal use only.
1992 79: 2507-2519
Molecular genetics of von Willebrand disease
D Ginsburg and EJ Bowie
Updated information and services can be found at:
http://www.bloodjournal.org/content/79/10/2507.citation.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.