Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Physiology 100
Laboratory Manual
Winter 2008
Course Chairperson
Julio L. Vergara
Laboratory Staff
Ken Roos
Courtney Gordon
Department of Physiology
David Geffen School of Medicine
UCLA
©DEPARTMENT OF PHYSIOLOGY, UCLA, 2007
ALL RIGHTS RESERVED.
Contents
Introduction ........................................................................... 1
Laboratory Groups ................................................................... 3
Nerve & Synapse Simulation Laboratories ........................................ 4
Nerve Action Potential Simulation ................................................. 5
SYNAPSE: Synaptic Transmission Simulation ................................. 13
Cardiovascular Simulation (CVSIM) Laboratory ............................... 21
Human Circulation Laboratory.................................................... 32
Human Patient Simulator Laboratory…………………………………………42
Respiratory Physiology Laboratory ............................................... 45
Physiology 100 Laboratories
1
Introduction to the
laboratories
Objectives
1.
Provide opportunities for students to perform experiments that illustrate physiological
principles taught in lecture.
2.
Provide opportunities for small group discussion of challenging physiological concepts
among students and with faculty members.
There are 6 laboratory exercises given over Friday afternoons and attendance is mandatory. The
exercises are 1-2 hours in length on a given day; there is a total of only 10 hours of lab time
during the quarter. Because of limited resources, you must attend the lab session to which you
are assigned. You may not switch lab groups or lab times without pre-authorization by Dr.
Roos. All efforts have been made to evenly distribute lab session times. There are no make up
labs. However, if you are ill and unable to make it to the lab that day, see or call Dr. Roos or Mr.
Gordon; under these circumstances, please do not come to lab and share your germs.
The Physiology 100 Laboratory Manual contains a detailed description of each laboratory
exercise. Students are expected to read and prepare for each laboratory exercise
before coming to class.
The Physiology 100 lectures and laboratories are designed to work together in order to teach and
illustrate general principles of physiology. The laboratories do not stand alone; they rely heavily
on principles taught in lecture. At the same time, the lectures do not stand alone; they rely
heavily on principles illustrated in the various laboratory exercises. Both the lectures and the
laboratories are necessary for the student to have a thorough understanding of concepts in
physiology. The laboratory also provides opportunities for students to interact with faculty in a
small group environment. Ample time is provided for discussion and answering student
questions.
The Physiology 100 Laboratories are not graded exercises; there are no laboratory reports to turn
in. However, the faculty views the laboratories as integral to the study of physiology, and
therefore material from the laboratories, including specific examples from various exercises,
comprise a significant portion of the exams.
Physiology 100 Laboratories
2
One or more of the course lecturers direct each laboratory exercise. In addition, other faculty
members from the Department of Physiology and other departments of the David Geffen School
of Medicine at UCLA will be present at each laboratory for student assistance, along with the
Physiology Student Lab staff. If you have questions regarding a specific lab exercise
after class, please direct your questions to the faculty lecturer for that topic.
The Department of Physiology is extensively involved in creating software that will enhance the
student experience. Faculty members of the Department of Physiology created the computer
simulation programs used in these laboratories. Drs. Francisco Bezanilla, Julio Vergara, and
Nikola Jurisic created the Nerve Action Potential Simulation. Drs. Michael Letinsky, Nikola
Jurisic and Julio Vergara originally created the SYNAPSE program, which was later modified
by Drs. Jonathan Monck and Sebastian Uijtdehagge (SOM-IDTU). The CARDIOVASCULAR
SIMULATION was created by Drs. Allan Brady and Earl Homsher, and modified by Drs. Ken
Roos, Gordon Ross, Oscar Scremin and Sebastian Uijtdehagge (SOM-IDTU).
Several faculty members have written the chapters in this manual, and we are grateful for their
assistance. Drs. Diane Papazian, Julio Vergara and Jonathan Monck wrote the Nerve Action
Potential / Synapse Simulation chapters. Drs. Earl Homsher, Robb MacLellan, Ken Roos, and
Oscar Scremin wrote the Cardiovascular chapters. Dr. Ken Roos and Courtney Gordon
developed the human patient simulator scenarios. Dr. Christopher Cooper wrote the Respiratory
Mechanics chapter which was modified by Drs. Ken Roos and Sally Krasne. This manual was
assembled and edited by Drs. Ken Roos and Julio Vergara.
Physiology 100 Laboratories
3
Laboratory Groups
School of Dentistry Class of 2011
GROUP 1
Abelowitz, Ryan
Fang, Qing
Gill, Sona
Gutierrez, Oscar
Haimof, Ryan
Huerta, William
Lee, Victor
Nguyen, Thomas
Pham, Philong
Prero, Yisachar Dov
Razi, Miriam
Refela, Peter
Robb, Vanessa
Shahi, Parisa
Sheng, Sally
Suktalordcheep, Shandra
Um, Suzin
Van, Vincent
Vassilieva, Veronica
Yashari, Saman
Yildirim, Yavuz
Zhou, Zhao
GROUP 2
Antonie, Laura
Baek, Joon
Barlow, Kaitlin
Cheng, Karen
Farhadian, Makhmal
Heit, Jessica
Ho, Ly
Huang, Joyce
Lee, Jay
Lee, Jin Kuk
Maya, Janet
McDonald, Jenna
Morris, Kirk
Ortega, Julio
Oyama, Jeffrey
Phung, Long
Tan, John
Vang, Kham
Wilks, Konita
Wong, Isabel
Yap, Kimberly
Zhu, Lin
GROUP 3
Alvarez, Michelle
Astete, Michael
Chen, Michelle
Erhard, Michael
Fallah, Neda
Gerges, Mickel
Hansen, Nathan
Husain, Mohammed
Johnson, Malieka
Johnson, Matthew
Kaufman, Matthew
Mardirosian, Martin
Modi, Meril
Nasseri Nosar, Nader
Olivares, Nicole
Pardo, Monica
Saadat, Nariman
Simanian, Maurice
Tong, Michael
Umof, Natalie
Zaul, Naomi
GROUP 4
Assefina, Amir
Carbonell, David
Carlson, Chuck
Chalak, Amir
Chen, Christopher
Ehsan, Bebenaz
Farshidi, Farzin
Godoy, Hector
Hartunian, Arina
Hidalgo, Geraldine
Hosseinian, Banafsheh
Hsiao, Erica
Kim, Aileen
King, Garrett
Moradi, David
Nantale, Grace
Nielsen, Brady
Park, Dawnelle
Read-Fuller, Andrew
Smith, Cicely
Truong, An
Yu, Bo
Physiology 100 Laboratories
4
Nerve & Synapse
Simulation Laboratories
In these laboratory sessions you will perform a number of experiments using computer
simulations investigate the properties of the action potential and the mechanisms of synaptic
transmission. In the first session you will use the NERVE program to explore the properties of
excitable membranes and their ability to generate actions potentials, the ionic basis of the action
potential, and how action potentials propagate along a nerve. In the second session you will use
the SYNAPSE program to study the mechanisms of transmission across a neuromuscular
junction. This laboratory will allow you to examine the Ca2+ dependence and quantal nature of
synaptic transmission, and the ionic basis for postsynaptic action potential generation.
NERVE: Action Potential Simulation………...……………...………………………
Introduction……………………………...……………...………………………………
Experiment 1. Relationship between K+ conductance and K+ current………………
Experiment 2. Relationship between Na+ conductance and Na+ current…………….
Experiment 3. Threshold for action potential firing……………………………...
Experiment 4. Refractory periods………………………………………………...
Experiment 5. Propagated action potential……………………………………….
5
5
7
8
9
10
11
SYNAPSE: Synaptic Transmission Simulation………………………..……….
Introduction………………………………………………………………………
Experiment 1. The end plate potential and end plate current……………………..
Experiment 2. The postsynaptic current and reversal potential………………….
Experiment 3. Quantal nature of synaptic transmission…………………………
Experiment 4. Presynaptic calcium current and synaptic transmission………….
13
14
15
17
18
20
Physiology 100 Laboratories
5
NERVE Action Potential Simulation
INTRODUCTION
The computer simulation experiments described below are designed to explore the properties of
excitable membranes and their ability to generate action potentials. These experiments are based
upon the squid giant axon, which was the biological preparation where all the original
experimental information was obtained by Hodgkin and Huxley. However, the principles that
you learn here can be directly applied to action potentials in the mammalian nervous system, as
well as in skeletal, cardiac and smooth muscle. An understanding of how ionic currents,
conductances, and membrane voltage are interrelated will also provide a strong foundation for
understanding synaptic function.
In each exercise there is a basic experimental setup which lets you get started, and then you are
asked several specific questions. You perform "experiments" to help you answer these questions.
Be sure to keep track of what you do experimentally, as the results from earlier experiments may
help you later with the more complicated experiments.
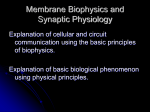
PROGRAM SETUP
Start the nerve program. If the program was
running, some of the parameters may be
different from the default values. To correct
this, press F10 (or click on RESET
parameters) which will revert most of the
parameters to their default values. The access
to the different simulation modes is by way of
the button on the left side of the main screen,
as shown in Figure 1. For example, to initiate
an action potential simulation, just click on the
Membrane AP button. This action will open a
window that has a plotting area and several
buttons to perform different operations. Some
of these operations can also be done by using
the keyboard shortcuts listed below.
Figure 1. Main Window of the Nerve Program.
Shortcut keys for Menus and Commands
F3 run Propagated AP simulation (from the Propagated AP window)
F6 Axon parameters
F7 Stimulus
F8 Concentrations
F9 Variables to Plot Menu
F10 reset parameters to default values (from main window)
ESC Close window in use.
EXP
ERI
Physiology 100 Laboratories
6
MENTS
The initial experiments are designed to familiarize you with the different variables that are useful
in understanding the generation of the action potential. Note that these experiments are done
under "current clamp" in an axon where the membrane potential is the same everywhere (see text
box for explanation).
Current Clamp vs. Voltage Clamp
The axon properties can be studied under two different kinds of stimulation conditions:
voltage clamp or current clamp. In the voltage clamp condition, the experimenter
controls the voltage and measures the current. It is the most effective way to describe
the properties of voltage dependent ion channels. Under voltage clamp, the membrane
potential is constant and therefore there is no capacitive current (except during the
instant when the voltage is stepped from one voltage to another)
In this laboratory, the experiments are in current clamp mode, in which the
experimenter applies current pulses to the interior of the axon and observes the
membrane voltage response. This is closer to the physiological conditions, and
experiments done under these conditions will give a closer insight as how the normal
axon works. However, the mechanisms involved in the genesis of an action potential
under current clamp conditions are somewhat harder to understand because the
voltage controls the conductances, which in turn allows ionic currents to flow through
the membrane, which in turn modify the membrane voltage (Hodgkin cycle). The
precise purpose of the laboratory is to allow you to fully understand the complexities of
this process.
Membrane vs. Propagated action potential.
As we are dealing with an axon, changes of membrane voltage in one spot may be
different to other regions of the axon. However, in the Membrane Action Potential
condition (Membrane AP button in Figure 1) we eliminate this problem by inserting
an axial wire and making the interior of the axon isopotential along its entire length
("space clamp condition"). In Propagated Action Potential simulations, (V vs. t Propagated AP button in Figure 1) the axon does not contain the axial wire. To
simplify the interpretation, all the initial experiments are done with the axial wire.
Physiology 100 Laboratories
7
Experiment 1. Relationship between K+ conductance and K+ current
To start, click on the Membrane AP button. We will run the simulation program using "ideal
Na and K channel properties" where only sodium and potassium ions go through their
respective channels (i.e. in an ideal Na
channel, only Na can permeate). Therefore,
click on the Axon button (or press F6) and
select Ideal channels. Now close the Axon
window and look at the AP simulation, which
should look like Figure 2. This is a plot of the
voltage as a function of time (black trace, see
Figure 2) along with the current pulse used to
stimulate axon, also as a function of time (red
trace, see Figure 2).
In this experiment, you have injected a current
pulse (of 10 µA and 0.25 ms duration) into the
axon and recorded the membrane potential.
These are the default values, but later you will
be able to change them in the course of the
laboratory.
Figure 2. Membrane Action Potential.
Let us now explore what is the time course of some of the variables that are involved during the
generation of the action potential. The program allows you to select and plot in the same screen
many of the important variables. For example, let us look at the potassium current and potassium
conductance during the action potential
l. Click on Var. to plot, (or press F9), which
will open the Variables to Plot window, and
click on the potassium conductance (gK) and the
potassium current (IK). Then close the
Variables to Plot window.
Now you should see plots of the membrane
voltage, gK, and IK (Figure 3). In which direction
is the potassium current flowing, into or out of
the cell?
By clicking several times on the right hand scale
you can display the legend for Im, gK and IK. You Figure 3. Membrane AP, IK and gK.
can also vary the range for the gK and IK plots
by expanding or compressing the plotted scales using the E and C buttons. For example, after
you have clicked to display gK, the default full scale will be ±20 mS/cm2 and if you press E, the
maximum scale will read ±10 mS/cm2 and the gK trace will be twice as big, allowing you to see
more details. Press C to go back to the original scale. To make comparisons easier between
different variables, you can select a different plotting scale for IK. Also, as before, you can
display the legend and scale for each variable by repeatedly clicking on the right hand scale. In
addition, by clicking the mouse in the plotting area, a vertical cursor appears and the values of
Physiology 100 Laboratories
8
time, voltage, and selected variable (on the right hand scale) are displayed at the time signaled by
the cursor.
Figure 3 shows an example of the screen that you will see. Notice the time courses for IK and gK
are different. The IK curve reaches its peak before gK, why? [Hint: display the equilibrium
potentials (by clicking on E's check button) and observe the relationship between EK (blue line)
and the membrane voltage (black trace). The
numeric value of EK can be found be clicking on
CONC (Concentrations, F8). Does this value seem
reasonable?]
Observe the falling phase of the potassium current.
Why does the potassium current (IK) fall to nearly
its resting level while gK is still much greater than
0? Is IK equal to 0? You can check this more
accurately by using a higher gain (higher
magnification using the E button) for the IK plot.
Once you understand the reasons for the different
Figure 6. Membrane AP, INa, gNa, m and h.
time courses of IK and gK, you can add the n curve
to your plot. The screen should look like Figure 4.
The n curve is a measure of the time course of the
opening and closing of one of the subunits of the
potassium channel (often referred to as n gate).
Click on the right hand scale until you display the
scale for the n curve. Remember that the
probability of opening of the potassium channels
is: Po = n4. Note that the n curve does not start at Figure 4. Membrane AP, IK, gK and n.
0. Why is there a very small current while the
resting value of n is ~0.25? Also, why is IK nearly
0 at the end of the action potential even though at
this time n is ~0.7, which is significantly larger than
its resting value?
Experiment 2. Relationship between Na+
conductance and Na+ current
Now you may consider how Na ions are involved in
the action potential. Click on Var. to plot and
deselect the K variables and check the Na variables,
INa and gNa. You should see plots of the membrane
voltage, gNa, and INa. Remember, as before, you can
display the legend and the plotting scales that are Figure 5. Membrane AP, INa and gNa
best for comparing gNa and INa by repeatedly
clicking on the right hand scale. Figure 5 shows the screen with gNa, INa, and membrane voltage
plotted. Notice that the time courses for INa and gNa are different. In which direction does the
sodium current flow during the action potential?
Physiology 100 Laboratories
9
There are several interesting and important features shown in the Na current trace. First, why is
there a notch in the INa trace? [Hint: display ENa and consider the relationship of ENa to the
membrane voltage V.] What does the existence of a notch tell you about the relation between INa
and gNa? Also, notice that the peak INa curve occurs later than the peak of the gNa curve, why?
Once you understand the reasons for the different time courses of INa, and gNa, add the m and h
curves to your plot. Note: these variables can best be understood if you simplify your screen by
removing the sodium current (deselect INa in Var. to plot). Now you can compare the time course
of the membrane voltage and the m and h curves during an action potential along with gNa (which
is proportional to m3h). The screen should look like Figure 6. Click on the right hand scale to
display the legend for the m or h curves.
Remember that m represents the probability that one of the subunits is in the active position, and
that in the classical Hodgkin & Huxley formulation three are required to open the channel (m3);
at the same time the inactivation particle has to be out of position for the Na channel to conduct.
[Note: the probability that the inactivating ball is in position is given by 1-h. Therefore the
probability that the Na channel is conducting will be: Po=m3h]. Thus, from these two curves you
can get an appreciation of how the two gates of the Na channel can act to regulate its
permeability. Note that the m curve does not start at 0 (what does this mean?) and that the h
curve does not start at 1 (what does this mean?). How are these features consistent with the
negligible Na+ current at the resting membrane potential? In addition, why does the sodium
conductance begin to fall while the channel's m gate is still open?
What would occur if you tried to stimulate the nerve with a second current pulse delivered at the
point in time when of the sodium conductance reaches the peak? Don't do this experiment now,
just think about it; you have enough information to make a definitive statement. In fact, now you
should be able to explain the ionic mechanisms responsible for the absolute and relative
refractory periods (more on this later).
Experiment 3. Threshold for action potential firing
We will now examine the threshold, which is a property that defines whether the action potential
will, or will not, be generated. Restore the action potential parameters to normal, making sure
that you maintain "ideal" channel properties (click on RESET parameters, or press F10 but
make sure that ideal channels is selected in the Axon parameters window).
In the pulses (F7) window set the amplitude to 10 µA and the total duration to 10 ms. Now,
experimentally determine the amplitude of the current pulse that is required to just exceed
threshold (that is, that generates an action potential). To see the relationship between different
stimulus intensities you can save each screen by clicking in SAV ALL and checking super to
superimpose the traces as you change the stimulus strength.
Physiology 100 Laboratories
10
Figure 7 shows one example of two superimposed traces, the suprathreshold stimulus was 6.7
µA and initiated an action potential but a 6.6 µA did not. Experiment with the amplitude and
observe how sharp the threshold is. Why does
the progressive reduction of the stimulus
intensity cause the onset of the action potential
to occur at progressively longer times after the
cessation of the stimulus? [Hint: One suggestion
as to how to approach answering this question is
to examine the total ionic current at high
magnification, together with the Na and K
currents. Observe the direction of the currents
just when the action potential is taking off].
Also, why does the membrane potential remain
almost flat past the turn off of the current pulse
when the stimulus is at the threshold?
Figure 7. Superimposed APs obtained with 6.6 and
6.7 µA pulses, respectively.
Try now to correlate the threshold events with
the conductances (and also plot the h variable).
Once you see how the membrane voltage is related to the membrane conductances you should be
able to explain why the stimulus that is just suprathreshold generates a smaller than normal
action potential (i.e., compared with the action potential resulting from a stimulus of 10µA).
Experiment 4. Refractory periods
So far we have examined the properties
of a single action potential; we will
study how one action potential can
affect the generation of a second action
potential.
First
restore
default
parameters (RESET parameters) and
then in the pulses window increase the
Total Time to 20 ms and add a second
pulse (set PULSE 3 to 10 µA
Amplitude, and 0.25 ms Duration.
Then modify the duration of PULSE 2
(which operates as an interval with no
pulse) to 12 ms. Make sure that the
amplitudes of the first and the third
pulses are the same.
Figure 8. Two paired stimuli separated by 12 ms generate
similar action potentials.
You should see two action potentials as
shown in Figure 8. Save this screen (click on SAV THIS). Now we will change the first
stimulus, PULSE 1, and see how this affects the second action potential. First, progressively
decrease the amplitude of PULSE 1 and observe the second action potential waveform.
When you decrease PULSE 1 to an amplitude that is near threshold (i.e., S1 set between 6.7 -7
µA), the second action potential is abolished. Try different amplitudes for PULSE 1. Why does
PULSE 3, which was previously suprathreshold, now become so much less effective in eliciting
Physiology 100 Laboratories
11
an action potential and even become subthreshold if PULSE 1 is made small enough? If you
change PULSE 3, can you elicit the second action potential?
Now let us explore the generation of a second action potential as a function of the separation of
the two stimuli. In the Stimulus window (press F7) reset the first stimulus to 10 µA and 0.25 ms
and change the Interval to 6 ms. Keep changing the stimulus amplitude of the second pulse until
you have an action potential (e.g. 50 µA, Figure 9). Then repeat this process by making the
interval even shorter and modifying the amplitude of the second pulse to recover the second
action potential. Why can you not obtain a second action potential regardless of the amplitude of
the second pulse when you decrease the interval below a critical level? What do these results
tell you about refractory periods and
threshold?
Be sure that you understand the
mechanisms underlying these processes.
Try to explain these results remembering
what you know about Na inactivation and
potassium activation. A simultaneous plot
of h and gK is very useful.
There are many physiological factors that
can affect the excitability of a cell.
Dramatic changes in excitability can
occur, for example, in response to small Figure 9. Two paired stimuli separated by 6 ms. The
second stimulus requires a larger amplitude than the first
changes ionic concentrations or when one.
cells are exposed to very small
concentrations of drugs and toxins. You
may want to study some of these effects on your own using this program.
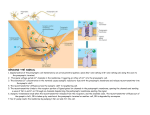
Experiment 5. Propagated Action Potentials
Close the Membrane AP window and click on the Stimulus button to set up the standard 0.25 ms
duration pulse with a 10 µA pulse amplitude stimulus and a Total Time of 10 ms. Press the
RESET parameters button (or press F10 to reset). Then click on the V vs. t-Propagated AP
button and observe the time course of the propagated action potential as detected at three points
along the axon (note the position of detecting electrodes in Figure 10).
Compute the conduction velocity. This can be easily accomplished using the cursor feature. Click
with the mouse at the peak of the blue action potential and you will get the time and the value of
the voltage at this point: take note of the time and the position of the electrode. Next, click on the
peak of the red action potential and take note of the time and position of the electrode. Knowing
the time difference and the distance between the electrodes you can compute the conduction
velocity.
Note the radius of the axon during the previous simulations and now change it to 400 µm. Run
the simulation again. What happened? You should consider how to cause an action potential in
an axon of this larger radius. [Hint: vary the stimulus intensity. Do you understand why?].
Physiology 100 Laboratories
12
Once you obtain an action potential, calculate the new conduction velocity for this larger
diameter cell. Did it increase, decrease or did not change? Did the shape of the action potential
change?
Now change the radius of the axon to 100 µm, but before running the simulation think about the
magnitude of the stimulus pulse. What type of a voltage response do you expect in the nerve if
you use the same stimulus parameters as you used with the 400 µm radius axon? After you
adjust the stimulus, calculate the conduction velocity. After completing the measurements at
several radii, what can you conclude about the effect of fiber diameter on conduction velocity?
Be sure that you can give an explanation of the mechanisms responsible for the conduction
velocity in an axon.
Figure NOTE:
10. The In
propagated
action potential
the propagated
actionrecorded at three
differentpotential
sites.
window, to see the effect of
any change in parameters, you must
rerun the simulation by clicking on the
START button (or press F3).
Physiology 100 Laboratories
13
SYNAPSE: Synaptic Transmission Simulation
In this laboratory you will be using SYNAPSE, a simulation of synaptic transmission at the
amphibian neuromuscular junction (or motor end plate), which was the experimental preparation
where most of the basic features of synaptic transmission were first worked out. The mechanisms
you will learn about are applicable to most mammalian synapses. There are several experiments
that you will work through to enhance your understanding of both postsynaptic and presynaptic
mechanisms involved in synaptic transmission. Representative examples of the types of traces
you will observe are provided in each experiment. However, because the stochastic nature of
synaptic transmission is realistically modeled in SYNAPSE, the responses that you actually
observe will be slightly different than those in the laboratory manual.
SYNAPSE is a typical Windows application that is controlled by clicking menu options. For
example, click the Run menu to run a simulation under various conditions. Choose the
Presynaptic Terminal, Synaptic Cleft, and Postsynaptic Cell menus to change conditions
inside the presynaptic terminal, at the synaptic cleft and in the postsynaptic motor end plate,
respectively. Hot key combinations for many of these operations are available.
Hot key combinations for Menus and Commands
F3
Run > Run Simulation
F4
Run > Check to Superimpose Traces
F7
Presynaptic Terminal > Stimulus
F8
Presynaptic Terminal > Physiological Parameters
F9
Presynaptic Terminal > Curves to Plot
Ctrl+F8
Synaptic Cleft > Physiological Parameters
Ctrl+F9
Synaptic Cleft > Curves to Plot
Shift+F7
Postsynaptic Cell > Stimulus
Shift+F8
Postsynaptic Cell > Physiological Parameters
Shift+F9
Postsynaptic Cell > Curves to Plot
Shift+F5
Postsynaptic Cell > Postsynaptic Cell Parameters
Ctrl+D
Experimental Preparations > Default Experimental Settings
Physiology 100 Laboratories
14
INTRODUCTION
Start by examining a typical response recorded at the neuromuscular junction. Once SYNAPSE
is running you will observe the main menu. Begin by clicking Run, then click on Run
Simulation (i.e., Run>Run Simulation) to start the simulation. Your screen should look like
Figure 1.
Figure 1
Note: If the screen does not closely resemble Figure 1,
then check the Experimental Preparations menu to see
that the Amphibian Neuromuscular Junction is
checked. Also, reset the default conditions by clicking
Experimental Preparations>Default Experimental
Settings. Note that pressing the hot key combination,
Ctrl+D, will also reset the default conditions.
Examine the voltage traces displayed in the window. The black trace is the presynaptic action
potential as recorded intracellularly at the presynaptic nerve terminal. The colored trace is the
postsynaptic membrane potential recorded at the motor end plate of the muscle fiber. Notice that
there are scale displays for both the pre- and the postsynaptic signals on the left side and the right
side of the screen. Compare the shapes of the presynaptic and postsynaptic action potentials.
What differences do you see? Note that the presynaptic action potential is similar to the action
potential you have just studied in the NERVE program. Why does the presynaptic action
potential have an undershoot (hyperpolarization) whereas the postsynaptic action potential does
not?
Hint: you can display the equilibrium potentials by clicking
View>Equilibrium Potentials and checking the appropriate
options.
Physiology 100 Laboratories
15
Note that the postsynaptic waveform is complex since it has components arising from two
contributions: a) the end plate channels (ACh receptor channels) responsible for the local
depolarization called end plate potential (e.p.p.); and b) the muscle ionic channels (Na, K, and
Cl) which are present in the neighborhood of the end plate and are responsible for the initiation
of the action potential in the muscle fiber. To better study synaptic transmission we need to
examine the synaptic potential itself, without the complications of the action potential.
Experiment 1. The end plate potential and the end plate current.
We want to study the e.p.p. in isolation. Therefore, we must eliminate the action potential
waveform that obscures the true e.p.p. time course. To do this, we need reduce the magnitude of
the local depolarization so that it is below the threshold for the initiation of the muscle action
potential. This can be achieved by using low doses of a postsynaptic blocking agent like curare,
which is a competitive inhibitor of acetylcholine. As you will see later, similar results can be
achieved by reducing the external Ca2+ concentration.
Initially, we will use curare to reduce the e.p.p. amplitude. Click on Synaptic
Cleft>Physiological Parameters and add some curare to the external solution bathing the
preparation. To change values you can either use the spin bars or directly enter values into the
field. Begin with approximately 1.0 µM curare. Once you have entered a curare concentration
click Run>Run Simulation to start the simulation. Gradually increase the curare concentration
to see how the postsynaptic response
changes. You can change the
amplification of the displayed traces to
better see the e.p.p. amplitude changes
by clicking Postsynaptic Cell>Curves
to Plot. Then modify the amplitude
scale value by clicking the spin bar.
Once you have a good understanding
of the effect of curare on e.p.p.
amplitude, set the curare concentration
to 4 µM. To best see the e.p.p., adjust
the amplitude gain of the Postsynaptic
Membrane Potential to 5 mV/div.
Your screen should look like Figure 2.
Figure 2
We have now attained a situation in
which the local depolarization of the motor end plate
through postsynaptic ligand-gated ionic channels
opened acetylcholine in the synaptic cleft
(acetylcholine receptor, or AChR, channels). To
display the current through the AChR channels,
click Postsynaptic Cell>Curves to Plot and
check Synaptic Current. Here synaptic current
(e.p.p.) results mostly from ion flow
Note: you can save experimental
parameters by clicking File>Save
Experimental Protocols.
Physiology 100 Laboratories
16
refers to the end plate current (EPC), which is the current through the AChR channel. Adjust the
current scale to 0.1 mA/cm2 and run the simulation (your display should look similar to Figure
3).
Notice the shape and time course
of the synaptic current trace. This
trace shows only the current
through the synaptic channels
opened by the neurotransmitter.
The scale values for each trace
can be selected by clicking in the
space between the scale values
(see arrowhead on the right side
in Figure 3). What is the
direction of the end plate current
flow? What ions could carry this
current?
Figure 3
Remember: an inward flow of positive
ions is depicted in the downward
direction (i.e. as a negative current).
Display the total postsynaptic membrane current by clicking Postsynaptic Cell>Curves to Plot
and checking Total Current. If you have added sufficient curare, you should see that the total
current and the EPC superimpose. Why is there only a small contribution from voltage-sensitive
Na+ and K+ channels even though the postsynaptic membrane has been depolarized?
Compare the time course of the synaptic current with the time course of the e.p.p. Why is the
time course of the synaptic current (EPC) different from the time course of the e.p.p. waveform?
Why does the EPC reach its peak before the e.p.p.?
Hint: Think back to the Nerve Lab (Experiment 3).
What is the relationship between membrane
voltage and current?
Examine the initial onset phase and the decay phase of the synaptic current trace. What do you
think is responsible for the jagged, uneven nature of the rising phase of the synaptic current
trace? You will return to this question in experiment 3.
Physiology 100 Laboratories
17
Experiment 2. The postsynaptic current and the reversal potential.
In this experiment we will analyze the properties of the synaptic current. Start by re-initializing
the system with the default settings (Experimental Preparations>Default Experimental
Settings). Run the experiment without curare (Synaptic Cleft>Physiological Parameters), at
Figure 4
20 mV/div (Postsynaptic Cell>Curves to Plot) and remove the histogram of quantal release
(Synaptic Cleft>Curves to Plot). Display the synaptic current and set the scale to 0.5 mA/div
(Postsynaptic Cell>Curves to Plot>Synaptic Current). Now you should see the presynaptic
action potential, the complex postsynaptic action potential combined waveform, and the synaptic
current (see Figure 4).
Examine the synaptic current trace. Notice that there is an inward phase (as observed in the
previous experiment), followed by an outward phase (not seen before). How can you account for
the outward direction of current flow in the synaptic current trace? Why didn’t you see this
outward flow of synaptic current in the previous experiment?
You can now display the Na+ and K+ contributions to the synaptic current by selecting
Postsynaptic Cell>Curves to Plot and checking Na and K (top right). What can you say about
these current components when the total synaptic current reverses? At what postsynaptic
membrane potential do you predict the synaptic current to reverse direction (reversal potential)?
Can you explain why the magnitude of the inward current is larger than the magnitude of the
outward current?
NOTE: There is more than one
explanation for the larger inward
current.
Think
about
what
experiments you could do with the
program to determine which is the
most important explanation here.
Physiology 100 Laboratories
18
Before proceeding, make sure that you understand the salient features of the synaptic current,
and how they are related to the e.p.p.-action potential waveform.
Experiment 3. The Quantal Nature of Synaptic Transmission.
The next series of experiments is designed to investigate the presynaptic mechanisms involved in
the release of neurotransmitters. In Experiment 1 you used curare to reduce the size of the
e.p.p., so that it could be studied without the superimposed action potential. Remember that the
onset phase of the synaptic current was ragged? What was your explanation? In this experiment
we will further study the quantal nature of the synaptic transmission at the neuromuscular
junction. As before, the amplitude of the e.p.p. must be reduced to below threshold so only its
contribution to the postsynaptic potential is seen. Now the e.p.p. amplitude will be reduced by
using a presynaptic blocking mechanism. This will be achieved by lowering the external Ca2+
concentration. Be sure that you can explain the difference between pre- and postsynaptic
methods of blocking synaptic transmission.
To begin, run the default simulation
parameters
with
the
postsynaptic
membrane potential gain set at 20 mV/div.
You can investigate the quantal nature of
synaptic transmission by also displaying a
histogram of the quanta released. First
click Synaptic Cleft>Curves to Plot and
check both the Histogram of Quantal
Released box and the Do Not
Superimpose Histograms box. Then click
View>Check to Show Quantal Content
to display a quantal content counter. This
displays the number of quanta released, Figure 5
which is equivalent to the number of synaptic vesicles fusing with the presynaptic membrane.
Rerun the simulation. Figure 5 shows a typical example in which the presynaptic response
caused the release of 208 quanta (i.e., the quantal content, m = 208). Your value will probably be
different. Why? Now, rerun the simulation several times. What did you notice about the
synaptic current trace?
To help see the difference, try
superimposing the traces by clicking
Run>Check to Superimpose Traces.
Normal amounts of transmitter are released when the Ca2+ and Mg2+ concentrations are set to 2.0
and 0.0 mM respectively (the default settings). The effect of Ca2+ on transmitter release can be
seen by progressively changing the concentrations in the external solution. To alter
concentrations click on Presynaptic Terminal>Physiological Parameters and change the
appropriate values. Try setting Ca2+ to 1.5 mM and run the simulation. How is synaptic
transmission affected by the reduction in external Ca2+ concentration to 1.5 mM?How do these
Physiology 100 Laboratories
19
changes in transmitter release affect the postsynaptic response?Under what conditions does the
postsynaptic response rise more rapidly?
Repeat this same experimental protocol using 1.0 mM Ca2+.
The e.p.p. should be significantly reduced, but still above
threshold. As you rerun the simulation at these new Ca2+
concentrations notice that the muscle fiber action potential
waveform changes. How does the shape and size of the
muscle fiber action potential change? Why does the initial
rate of onset of the e.p.p. change?
Note: To best observe the
behavior of the release
process under these varying
conditions
each
new
simulation paradigm should
be run several times while
superimposing the traces.
Continue to alter the Ca2+ concentration
until only 2 - 4 quanta are released in
each trial. As release is decreased, the
gain of the postsynaptic membrane
potential should be increased to 1
mV/div. Superimpose traces to see how
release changes. The screen should look
approximately like Figure 6.
How has the postsynaptic response
changed as the number of quanta
released has decreased?
Figure 6
Notice the shape of the e.p.p., its rise time, and its time of onset (i.e., the synaptic delay). What
causes the wide fluctuations in these features of the e.p.p.? Why does the rate of rise of the e.p.p.
seem to change in some e.p.p.’s? Why does the time of e.p.p. onset shift in different trials?
Synaptic transmission can be even further reduced so that sometimes no transmitter is released in
response to a normal presynaptic action potential (i.e., presynaptic activity produces a “failure”).
Adjust the Ca2+ value so the response fails approximately 50-70% of the time. Under these
conditions, transmitter release consists mainly of single quanta. Measure the amplitude of a
number of single quanta e.p.p.s (click View>Measure Values; click the left mouse button to
measure the e.p.p. amplitude). What could account for these e.p.p.’s having different quantal
sizes? Rerun the simulation several times. You should see that the variation in the synaptic delay
is even more clearly seen now, i.e release occurs at different times in each run. Why does the
time of release vary each time the presynaptic nerve terminal is depolarized?
Physiology 100 Laboratories
20
Experiment 4. Presynaptic Calcium Current and Synaptic Transmission.
The results in the previous experiment clearly demonstrated that synaptic transmission is highly
sensitive to the Ca2+ concentration in the external medium. However, neurotransmitter release
occurs when Ca2+ enters the presynaptic nerve terminal. To further investigate this process, we
will now examine how changes in presynaptic Ca2+ current result in changes in neurotransmitter
release. Run the same simulation protocol as above with about 50% failures with the presynaptic
Ca2+ current trace displayed (click on Presynaptic Terminal>Curves to Plot and check
Calcium Current with the scale set
to 0.005 mA/cm2 ). First run
simulation as just described above
(i.e., as the control for this
experiment). Then, change the
external Ca2+ concentration slightly
and rerun the simulation with
superimposition of traces turned on.
Observe how the Ca2+ current trace
changes and how this is reflected in
the amount of neurotransmitter
released.
Figure 7 is an example of typical
results you might see. Try several
Figure 7.
different Ca2+ levels, e.g. 0.5, 1.0 and
2.0mM. How would you describe the
sensitivity of the neurotransmitter release mechanism and changes in Ca2+ current to changes in
external Ca2+ concentration?
The final experiment we will look at the effect of Ca2+ channel blockers. Restore the external
Ca2+ concentration to 2mM. Rerun the simulation. You can test the effect of nifedipine (a Ca2+
channel blocker of the dihydropyridine class; related drugs are sometimes used to treat heart
disease) by selecting Synaptic Cleft>Physiological Parameters and increasing the
concentration of nifedipine with the spin bar. Try 5, 10, and 50µM. What happens to the Ca2+
current? What happens to the quantal content and the e.p.p.? What can you conclude about the
role of Ca2+ in synaptic transmission? What is the site of action (presynaptic or postsynaptic;
intracellular or extracellular)?
Physiology 100 Laboratories
21
Cardiovascular Simulation
(CV-SIM) Laboratory
Introduction
CV-Sim is a computer simulation of a simplified circulatory system developed by the faculty of
the UCLA Department of Physiology. With this simulation, students can observe how the
circulatory system behaves when variables normally controlled by the autonomic nervous system
or mechanisms intrinsic to the heart and vasculature are changed. In this model, the reflexes and
most of the feedback loops which normally maintain the system constant are removed so that the
student commands the controlling variables: heart rate, cardiac contractility, systemic
vascular resistance (SVR, or as text book calls it, the total peripheral resistance, TPR), the
compliance of the veins, blood volume, and posture. The student can see how alterations in
these variables change the hemodynamics of the circulation without being counteracted by the
reflexes. In the intact animal, some of these parameters can only be changed indirectly. The
model avoids the use of experimental animals and represents a reasonably accurate view of the
human circulatory system.
Some short-cuts were made in this simulation to conceptually simplify the system and speed
computation. Thus, the circulatory system has been reduced to only its essential elements (Figure
1). In this model there is only a left ventricular pump, a composite arterial component, a
composite systemic vascular resistance, and a composite venous compartment. Each composite
component has physical characteristics (pressure-volume behavior, total compartment size,
resistance, and responses to stimulation) similar to the group of tissues they represent.
Figure. 1
Physiology 100 Laboratories
22
“Blood” flows from the arteries to the veins through a resistance equivalent to the systemic
vascular resistance (SVR, or TPR). However, the low-pressure pulmonary circulation has been
omitted and there are no atria. Thus waveforms normally seen in the atria and distinctions
normally seen between the left and right ventricles are absent. [See the question later relating to
the Vander/Widmaier text figure 12-19, the “Wigger’s Diagram”.]
In the model, cardiovascular data is presented in a fashion comparable to that seen in an
Intensive Care Unit from patients instrumented with catheters. The student can choose the
parameters to display (arterial blood pressure, left ventricular pressure, central venous pressure,
and left ventricular volume). An electrocardiogram (ECG) is displayed at the same time base in
the window below the pressure and volume traces as a timing reference. Ventricular PressureVolume loops are displayed in a separate window. The model allows the student to click “on”
the “Show Time Bar” box above the recordings to obtain all the parameter values. Thus
measurements and computations of the systolic and diastolic blood pressure, mean arterial blood
pressure, left ventricular end-diastolic and left ventricular end-systolic volume, stroke volume,
cardiac output, and systemic vascular resistance can quickly be made.
This laboratory consists of two basic exercises. The first part guides you through the system
controls to obtain a set of baseline observed and calculated cardiovascular parameters. The
second tests your knowledge of the cardiac cycle and how its parameters change with heart rate.
Procedures
In the laboratory, CV-Sim will be running when you arrive. Though these exercises are designed
to take no more than the 2 hour lab period, you may wish to access the program for review by
downloading it from the course website. For downloading, pay close attention to the instructions
on the website. You will need at least a Pentium III-500 mHz with 128 MB RAM. In both cases,
the start page will prompt you to click the “CV-Sim” button starting a separate window for the
simulation traces.
You operate the simulation by manipulating the buttons and scrollbars within the program
display; do not use the browser controls. Select the desired display traces on the graphics screen
by clicking the appropriate color-coded box immediately above the recording window. You must
have at least one trace displayed for the program to run. You can display the following traces:
arterial pressure (red), ventricular pressure (black), ventricular volume (blue), or central venous
pressure (pink), Note that the arterial and central venous pressures are measured at the level of
the ventricle. There are also separate windows for the ECG and pressure-volume loop data. The
default scale is as follows: all pressures, 0-200 mm Hg; ventricular volume, 0-200 ml; common
time base, 8 seconds/sweep. The display trace and time base scaling may be changed with the
“Option” / “Graph Options” button (top line). You may also adapt the actual display trace speed
to match the computer clock speed with the “Option” / “Calibrate” button. Finally, you can print
your display by using the “File” / “Print” button using standard Windows procedures.
Physiology 100 Laboratories
23
The five variables we will use can be set by means of scrollbars on the right hand side of the
screen
heart rate (variable between 1-220 bpm, default value is 75 bpm)
contractility (variable between 1-100%. In the resting supine individual, the extent to
which the heart is activated by the release of calcium is only 30-40% of maximal. This
means that only 30-40% of the potential crossbridges are activated. The program default
value is 40%.)
systemic vascular resistance (this can range from 5-500% of normal. The 100% default
or resting control in this case corresponds to about 17 mm Hg/L/min (Wood Units) or
1350 dynes-s-cm-5 (SI units).
total blood volume (variable between 3-8 liters. The normal blood volume for a properly
hydrated 70-kg man is about 7% of the body weight or 5 liters, the default value.)
venous compliance (variable between 1-300% with 100% as normal default value. The
venous system is 10-20 times more compliant than the arterial tree and consequently in
normal supine individuals contains about 75% of all the blood in the body. Arteries
contain 20% of the blood, while capillaries hold <5 % of the total.
Three types of mouse actions change the variables on the scrollbar: clicking on the right or left
arrow boxes changes them by a single unit; clicking on the bar itself changes them by 10 units;
or the scrollbar may be dragged to any position.
To use the program in conjunction with this manual, note that bold print indicates scrollbar or
display actions to be performed by the user. To use the program, you click on the appropriate
buttons at the top of the window: run, stop, clear, and reset. Clear, clears the screen, but retains
the scrollbar settings. Reset returns all scrollbars to default conditions, but does not clear the
screen. To obtain the trace values and the time from the left edge of the display for each variable,
click “on” the “Show Time Bar” feature. Point to a specific point on the traces, left click the
mouse, and immediately obtain a value for all of the pressure and volume traces at the same
point in time (in ml or mm Hg and time). The time point is identified in the separate box for the
“Pressure-Volume Loop”. You can therefore determine the systolic blood pressure (SBP) and
diastolic blood pressure (DBP) from the arterial pressure trace. One determines the end-diastolic
volume (EDV) and the end-systolic volume (ESV) from the ventricular volume trace. From the
venous pressure trace, one can measure the central venous pressure (CVP). The ECG and
Pressure-Volume traces are provided in separate data windows for reference. Though data values
cannot be obtained within these windows, the circle in the PV loop is referenced to the time bar.
The following exercises (1) acquaint you with the operation of this simulation, (2) supplement
the lectures on the cardiac cycle, chronotropic regulation and on the effects of preload and
afterload, and (3) provide practice in estimating clinically important cardiovascular values.
Physiology 100 Laboratories
24
EXERCISE 1: Familiarization with CV-SIM
Default parameters for the CVSIM model are:
Heart rate
75 bpm
Systemic vascular resistance
100% normal
Venous compliance
100% normal
Contractility
40% maximum
Total blood volume
5000 ml
Posture
Supine
CLICK the appropriate boxes to display only the:
Arterial pressure
(Central) Venous pressure
Ventricular volume
TO GENERATE DISPLAY TRACES
Click “Run” with the left mouse button in Menu Bar to initiate the simulation.
Observe the tracings of arterial pressure, central venous pressure, and ventricular volume.
When this model starts running the first time, the system starts with the arterial and venous
pressures both at about 7-8 mm Hg. The pump elevates the arterial pressure and lowers the
venous pressure, reaching a steady state after several beats. Make sure you wait at least 10 beats
after each change in a parameter for the system to reach a new steady state. Note that the
pressure values are measured close to the pump and can be considered to be equivalent to central
venous “filling” and aortic pressures.
STEADY STATE RECORDINGS
For this experiment to work properly, your system must have reached a steady state. The system
reaches a steady state after about 10 cardiac cycles or two full display screens under default
conditions. When the system has reached a steady state, Click the “Stop” button to stop the
screen and make measurements.
To make measurements of values, left click on the “Show Time Box”, move the cursor into
the display window and onto a trace. Then click on the left mouse button to find the pressure,
volume or time values. You may also drag the bar with the mouse to any position. The
ventricular volume is displayed on a scale of 0-200 ml. The arterial, central venous and
ventricular pressures are displayed on a scale of 0-200 mm Hg.
Physiology 100 Laboratories
25
Observe, identify and discuss the arterial and venous pressure and ventricular volume traces
during steady-state operation.
Measurements to Make
Arterial diastolic pressure (DBP)
_____ mm Hg
Arterial systolic pressure (SBP)
_____ mm Hg
End diastolic volume (EDV)
_____ ml
End systolic volume (ESV)
_____ ml
Central venous pressure (CVP)
_____ mm Hg
[Round off the top 4 values to the nearest whole number]
Calculate the following values
Mean arterial pressure (MAP): MAP = PP/3 + DBP
(where PP = Pulse Pressure = SBP - DBP)
_____ mm Hg
Stroke volume (SV): SV = EDV - ESV
_____ ml
Ejection fraction (EF): EF = SV/EDV x 100
_____ %
Cardiac output (CO): CO = HR x SV/1000
_____ L/min
Calculated Systemic vascular resistance (SVR):
c SVR = (MAP - CVP)/CO
c SVR = (MAP - CVP)/CO x 80
_____ mmHg/l/min*
_____ dynes-sec-cm-5
* Clinically, SVR (or TPR) is expressed in “SI units” of dynes-sec-cm-5. To obtain SVR in these
units, simply multiply the value calculated value in “Wood units” (mm Hg/l/min) by 80.
Now that you have made these baseline calculations at steady state, remember that we noted that
all the pressures (ventricular, arterial, venous) were about 7-8 mmHg prior to the beginning of
the beating of the CV-Sim heart. Now you can see that the mean arterial pressure rose to about
96 mm Hg while the central venous pressure fell to about 5.5 mm Hg when the heart started
beating at 75 bpm.
Thought Question: Explain why arterial pressure rose, venous pressure fell as the
system started. Why did the arterial pressure rise so much more than the venous pressure
drop?
Note: Being able to calculate such physiological values from the information on the display
screen is essential to your use of the CV-SIM and to your understanding of cardiovascular
physiology.
Physiology 100 Laboratories
EXERCISE 2:
26
The Cardiac Cycle
Set Graph Scaling as follows to better correspond to Figure 2 on page 30.
Click ON the Ventricular Pressure Display Trace. [all traces on]
Click “Options/Graph Options”
Set:
Sweep Time Scale to:
New Value
3 Sec
(Previous)
8 Sec
Click Apply.
Click RUN and wait until the screen is filled with at least five complete screen cycles,
then Click STOP before the screen resets.
Questions
Measure the beat-to-beat interval. _________ sec. Round off this and all other time values to
two decimal places. Please enter this value in the appropriate box of Table 1 on page 29.
Calculate the heart rate. ___________ beats/min.
Reset the HR on the scrollbar to another value and recalculate the beat-to-beat interval and
calculated HR. (When finished, reset HR back to the default of 75.)
When you changed the HR, what happened to the timing interval of the EKG trace?
What electrical event in the EKG just precedes the onset of ventricular contraction?
Physiology 100 Laboratories
27
Identify the point in time at which the aortic valve opens. (label on Figure 2)
[Note: the beginning of contraction (the rapid upsweep of the ventricular pressure trace) is
arbitrarily indicated as the beginning of the first cycle at time = 0 sec on Figure 2]
The aortic valve is open when the ___________________ pressure exceeds the
____________________ pressure.
Measure the time from the onset of contraction, to the opening of the aortic valve.
____________ sec.
Define “rapid ejection”; Label on Figure 2.
What is the ventricular volume when contraction begins? _______ml
What is the ventricular volume when the aortic valve opens? _______ml
Explain the term ISOVOLUMETRIC CONTRACTION. (label on Figure 2)
How can you tell when the aortic valve closes
1) graphically? (label on Figure 2)
2) in a patient?
Physiology 100 Laboratories
28
What electrical event on the EKG is associated with aortic valve closure?
Measure the time period the aortic valve is open. _______ sec.
This time period in the cardiac cycle is known as the __________________time.
At this heart rate, the ejection time is what percent of the cardiac cycle? ______%
When does systole begin and end? Label on Figure 2.
Calculate the duration of systole. Enter this value in the appropriate box in Table 1 (next
page).
The duration of systole is also related to which events of the EKG?
Measure the time between the closing of the aortic valve and the beginning of filling of the
heart. ___________sec.
During this interval, what happens to:
Ventricular pressure?
Arterial pressure?
Ventricular volume?
Physiology 100 Laboratories
29
Define the term ISOVOLUMETRIC RELAXATION; Label on Figure 2.
When does diastole begin and end? Label on Figure 2.
Calculate the duration of diastole. Enter this value in the appropriate box of Table 1 (below).
Calculate the percentage of time in the cardiac cycle that is diastole and enter the value in
Table 1.
[% diastole = duration of diastole/beat to beat interval]
You have now completed the default (HR=75) values for Table 1. Now measure the
durations of systole, diastole and the beat to beat intervals at heart rates other than default.
Use the scrollbar to set the rates at 40, 100 and 160 beats/minute and determine each value.
Determine the percentage of the beat to beat interval occupied by diastole at each of these
rates. Interpret the results. Why is there a change in the systolic-diastolic ratio?
Table 1
HR
40
75 (default)
100
160
Duration of
Systole
(sec)
Duration of
Diastole
(sec)
beat-to-beat
interval
(sec)
diastole % of
beat-to-beat
interval
Physiology 100 Laboratories
Identify the following events/values/phases on the tracings below.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
Diastole
Diastolic pressure (arterial)
End diastolic volume
Systole
Systolic pressure (arterial)
End systolic volume
Venous pressure
Ejection time
Beginning of contraction
AV valve closes
First heart sound
Isovolumetric contraction
Aortic valve opens
Rapid ejection
Aortic valve closes
Second heart sound
Isovolumetric relaxation
AV valve opens
Rapid filling
Dicrotic notch
Figure 2
30
Physiology 100 Laboratories
31
Compare Figure 2 with the "Wiggers" diagram of the cardiac cycle from the text (Vander /
Widmaier, Fig 12-19). How and why might they differ?
Identify portions of the records shown in Figure 2 which correspond to:
a) Preload
b) Afterload
How could the records be used to assess changes in contractility?
How does this differ from any changes that might occur by altering the preload?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
The goal of this laboratory is to ensure that you have a basic understanding
of the cardiac cycle and of the regulatory factors that control the function of
the heart as a pump. Your instructors will lead discussions to help you
achieve this goal, but because previous academic experiences among the
class vary greatly, certain aspects of cardiac physiology will be crystal clear
to some but totally obscure to others.
It is each student’s responsibility to bring up for discussion those aspects
which he or she has found difficult or confusing.
Physiology 100 Laboratories
32
Human Circulation Laboratory
Overall Objective
The goal of today=s session will be to provide a basic “hands-on” introduction to the
measurement and interpretation of arterial blood pressure and its reflex regulation. This lab using
non-invasive methods is divided into 2 parts: the measurement of blood pressure via the cuff
method and an evaluation of coordinated cardiovascular responses. One half of the students will
do Part I and the other half part II for the first hour. The groups will swap places for the second
hour to complete the lab.
Since this lab falls after all the lectures, no new material will be presented. All the fundamental
concepts in this lab will have already been presented in lecture. The lab is designed to review and
reinforce the cardiovascular material. The practical aspects of taking a proper blood pressure are
to assist you in your future professional career.
Materials
Please bring your class notes, stethoscope, blood pressure cuff, and a watch with a second hand
to the lab at your assigned time.
Part I: The Measurement of Arterial Blood
Pressure
Objective
To obtain the practical skills necessary for accurate heart rate and blood pressure measurement
via the cuff and stethoscope method. To observe the normal variations in blood pressure over
time in same subject and between subjects.
Procedure
For this part of the lab, students will pair up to measure and record blood pressure and heart rate
on each other.
To measure heart rate:
Place your fingers over the radial pulse. Count the number of pulses in 15 seconds. (Begin your
count with zero.) Multiply this number by four to obtain a heart rate.
To measure blood pressure:
Examine the cuff. There is an area marked "bladder center@ or a white line. This is placed over
the brachial artery above the elbow. Leave enough space for the diaphragm of your stethoscope
Physiology 100 Laboratories
33
to be placed clear of the lower cuff border (Figure 1 – next page). When applying the cuff,
wrapped arm circumference must fall within the range marked on the cuff in order for the
reading to be accurate. Inflate the cuff by squeezing the bulb (making sure the valve of the bulb
is closed) until the pulse at the wrist disappears. Make a note of the pressure and deflate the cuff.
Re-inflate the cuff to about 40 mmHg above this pressure and then deflate the cuff slowly (about
3 mmHg/sec) while listening for the Korotkoff sounds with the diaphragm placed over the
brachial artery in the antecubital fossa. Note the pressure when the sounds first appear (systolic
pressure) and when they disappear (diastolic pressure). Often the sounds become muffled just
before they disappear. Refer to Figure 2 (next page) for additional assistance in the
interpretation of the sounds.
Obtain initial values and record on the data chart on the next page. Repeat these measurements
three more times at two-minute intervals.
If time permits, a demonstration of the effect of exercise on blood pressure and heart rate will be
given after these resting values have been discussed.
Figure 1: Cuff Placement and Principle of Operation.
Physiology 100 Laboratories
34
Figure 2: Sounds heard through a stethoscope while the cuff pressure is lowered.
(Vander / Widmaier text Figure 12-32.)
Data Table
Yourself
SBP/DBP
Initial
2 minutes
4 minutes
6 minutes
Partner
Pulse
SBP/DPB
Pulse
Physiology 100 Laboratories
35
Part II: Coordinated Cardiovascular
Responses
Objectives:
1.
2.
To elicit reflex and centrally mediated cardiovascular responses in a normal subject to
facilitate the understanding of the time course and the extent of those changes in real life
situations.
To analyze peripheral vascular changes secondary to postural changes and static exercise
to reveal the importance of those factors in the control of the circulation.
The instructor will request one volunteer per group to be monitored using the non-invasive
techniques described below. By analyzing the recorded parameters, the volunteer and students
should be able to predict the overall pattern of the cardiovascular responses and then discuss the
mechanisms involved.
Equipment:
The following equipment will be used in this station:
a.
Continuous non-invasive blood pressure monitor. [NIBP] A continuous, non-invasive,
recording of arterial blood pressure is obtained via a technique called arterial tonometry.
The arterial tonometer uses a sensor placed on the wrist over the radial artery that exerts
sufficient pressure on the skin to partially flatten the underlying radial artery. The intraarterial pressure is transmitted through the skin to the sensor. The sensor unit will be
placed over the subject’s radial artery and secured via a wrist brace and strap. A standard
blood pressure cuff is placed on the arm at the usual location to provide an automated
calibration value via the oscillometric method. Then the arm and wrist are placed in a
sling so that the wrist is at the level of the heart. NOTE: Small movements of the sensor
relative to the wrist can produce large changes in the readings. Then a 7-minute
calibration and equilibration period is initiated. When complete, the instrument can then
non-invasively display the arterial blood pressure waveform and determine the heart rate,
the systolic & diastolic pressures during the study protocol. Only averaged HR, SBP &
DBP values are displayed on the device itself.
b.
Continuous HR monitoring via the NIBP: The NIBP pressure waveform is fed to the
large display computer system for easy viewing as the top trace on the screen. The
computer software also displays numerical beat by beat (unaveraged) systolic, diastolic
and mean arterial pressure values. The beat by beat heart rate is determined by the
computer software from the peak systolic pressure of the NIBP. This is displayed as a
solid line on the second trace on the monitor and listed numerically below the pressures.
c.
Breath manometer to increase intrathoracic pressure for the Valsalva maneuver.
d.
Dynamometer to perform isometric exercise by handgrip.
Physiology 100 Laboratories
36
Protocol:
2a - Valsalva Maneuver:
This is the name given to any event in which we perform an expiratory movement against
a totally or partially occluded glottis. This is a very frequent act that includes coughing,
defecating, lifting heavy weights, singing or playing wind instruments. For this exercise the
volunteer will perform a Valsalva maneuver, that is, a sustained forced expiration against the
breath manometer to increase intrathoracic pressure between 40 to 80 mmHg, for at least 15
seconds. Pulse pressure will be used as indirect measure of systemic resistance. The
cardiovascular effects of an idealized Valsalva maneuver are summarized in the figure below.
Figure 3: Effects of the Valsalva maneuver on arterial blood pressure
and heart rate. Shading and arrows indicate period of expiratory effort.
Phase 1 is characterized by a transient increase in blood pressure due to compression of
intrathoracic blood vessels by respiratory muscles performing forced expiration.
Phase 2 - This increase in thoracic pressure subsequently inhibits venous return,
dropping preload and hence stroke volume. This results in a drop in systemic and pulse pressure
that trigger a reflex response mediated by the baroreceptors in the aortic arch and carotid
bifurcation, and is manifested as an increase in heart rate (tachycardia) and an increase in
systemic vascular resistance.
Phase 3 - Upon termination of the expiratory effort, pressure drops suddenly and
transiently, as blood fills the no longer compressed thoracic vessels. Venous return then
increases, leading to restoration of stroke volume.
Physiology 100 Laboratories
37
Phase 4 - During this phase, venous return is high, as are systemic vascular resistance
and heart rate, because of the activation of the baroreceptor reflex during the previous Phase. The
consequence is that arterial pressure rapidly increases above normal immediately after the
termination of the Valsalva maneuver. In response to this change the baroreceptor reflex is
triggered, but this time in the “opposite” direction. The reflex response is displayed as cardiac
deceleration (bradycardia) and decrease in systemic vascular resistance. The latter is manifest by
the increase in pulse pressure.
Comparable rapid changes in arterial pressure and heart rate may be observed in
everyday life during the performance of ‘mini-Valsalva” maneuvers like straining or coughing.
This maneuver can be provoked to compensate for a sudden loss of systemic arterial pressure,
and fighter plane pilots in high g-force maneuvers sometimes use it. The baroreceptor
mechanism provides means of stabilizing arterial blood pressure in the face of maneuvers
involving changes in intrathoracic pressure that we perform frequently. The Valsalva maneuver
constitutes a simple test of the baroreceptor reflex function. Lack of reflex bradycardia and
tachycardia signal a defect in the autonomic nervous system. Patients with this disturbance are
prone to postural hypotension.
Data: From the data obtained with your volunteer, fill in the following table.
Phase 1
Phase 2
Phase 3
Phase 4
HR
BP
Pulse Pressure
Thought Questions:
1) Identify all four phases of the Valsalva maneuver on your printout.
2) In what phase does someone with autonomic dysfunction “pass out?”
3) How much of an increase was there in the volunteer’s BP in Phase 4 as compared to
baseline values? Was this similar to the idealized response?
Physiology 100 Laboratories
38
2b - Postural Changes
Simple postural changes pose a severe challenge to the normal homeostasis of the circulatory
system. Redistribution of blood when changing from a supine to standing position results in a
20% reduction in intrathoracic blood volume. This reduction in venous return can drop the
stroke volume by as much as 30-40%. However, in normal subjects, BP drops only transiently.
The transient decrease in BP results in decreases in carotid baroreceptor and cardiopulmonary
receptor activity. This reduced input to the nucleus tractus solitarius elicits a reduction in vagal
output to the heart and a corresponding increase in sympathetic stimulation of both heart and
vasculature. Heart rate increases by 15-20 beats/min. (primarily due to carotid sinus reflex).
Increased sympathetic flow increases contractility and vascular resistance preserving BP.
Once the instrumented volunteer has been standing for a few minutes, a baseline
recording is obtained. Then, the volunteer slowly crouches down into a squatting position. After
squatting for at least two minutes, the volunteer will stand rapidly. This maneuver will be
performed promptly but in a careful manner, to prevent artifacts in the recording. Continue
recording for two more minutes after standing. Be sure to place event markers after each change
in position to facilitate the data analysis at the end of the exercise. Enter your results below.
Data:
Standing
Baseline
Squat for
2 minutes
Standing
Immediate
Standing
for
2 minutes
BP
HR
Thought Questions:
1) Did the volunteer get “dizzy” (pre-syncopal) during the squat-to-stand maneuver?
Discuss the potential effects of dehydration upon the observed compensatory blood pressure
and heart rate responses.
2) Use of antihypertensive medications (e.g. Beta-blockers or ACE inhibitors) leads to many
elderly patients presenting to an emergency department with a complaint of fainting. This
could also happen under the stress of a dental procedure. Why might this be?
3) Compare the Valsalva to the stand-squat study. What compensatory mechanisms are
recruited to maintain BP in each maneuver? Assume the volunteer had a neurological
disease that prevented use of the “skeletal muscle pump.” What changes might have been
different in this case?
Physiology 100 Laboratories
39
2c - Static (Isometric) exercise (if time permits)
Static or Isometric exercise as occurs when lifting or pushing heavy objects is a common
occurrence. In static exercise, a restricted set of muscles is used during a sustained contraction as
opposed to the alternating contraction-relaxation of isotonic exercise. In brief muscle
metaboreceptors elicit increased sympathetic activity and decreased vagal activity (can you
predict the effects on HR, cardiac output, BP and SVR/TPR of this response?).
Baseline measurements will be taken with the volunteer resting comfortably in a chair.
The subject will then perform a maximal voluntary contraction for one minute, using the
dynamometer (handgrip device). BP and HR will be determined at baseline, at the end of the
one-minute handgrip exercise, after a 5 minutes rest (if time permits).
Data:
Baseline
Maximal
Handgrip for
one-minute
5 Minute postmax handgrip
HR
BP
Pulse Pressure
Thought Questions:
1) How high did the volunteer’s BP rise above baseline with maximal effort.
2) Are the results similar to what you would expect with a dynamic exercise like running,
biking or swimming?
3) Why should patients with heart failure be discouraged from becoming “Olympic
weightlifters?” For that matter, would you encourage or discourage your patients from
carrying heavy baggage on their next air trip?
Physiology 100 Laboratories
40
Human Patient Simulator
Laboratory
Overall Objective
The goal of this exercise (Introductory lecture & formal laboratory) is to provide a basic “hand’son introduction to integrated patient management related to cardiovascular physiology and dental
anesthesia. The scenarios presented will allow the student to see how cardiovascular physiology
relates to their clinical practice especially with patients that have underlying cardiovascular
disease. The emphasis will be upon patient observation, the identification of normal vs. abnormal
parameters and potential emergency treatment plans during a dynamic exercise with the
simulated patient. These scenarios are based on actual incidents that occurred at the UCLA
Dental clinic. The details of the formal laboratory scenario will be handed out prior to the lab.
Materials
Please bring your class notes and stethoscope to the lab at your assigned time.
Overview of the Human Patient Simulator
The following information is provided for the student to become familiar with the common
features of UCLA School of Medicine’s Human Patient Simulator (HPS). For this first exposure
to the simulator, we will only utilize a sub-set of its features as listed below.
The HPS is a programmable, high-fidelity patient simulator designed for training in a variety of
healthcare scenarios. The HPS provides respiratory gas exchange, vital sign responses, lung and
airway resistance, as well as the provision for administering treatments. The HPS allows for
intubation, fluid management, cardiac defibrillation and pacing, chest tube drainage, needle
decompression, and lavage. There is also a provision for verbal responses from the manikin.
In the context of a simulation exercise, the HPS should be treated as one would a standardized
patient. A student may be called upon to assess the patient and employ an appropriate treatment
protocol. During simulation exercises, the student should feel free to utilize any and all possible
assessment and treatment strategies they have learned.
Prior to beginning a simulation exercise, students should take the time to orient themselves to the
simulator and identify the following landmarks for their reference. This will make the exercise
progress more smoothly and efficiently.
Physiology 100 Laboratories
41
Brachial
Pulse
Radial Pulse
Bilateral
Carotid
Pulses
Bilateral
Femoral
Pulses
Red = Pulse Locations
Pedal Pulses
Physiology 100 Laboratories
42
Heart
Sounds
Vocal
sounds
Lung Sounds
Bowel
Sounds
Physiology 100 Laboratories
43
Respiratory Physiology
Laboratory – Spirometry
Objectives
Measure pulmonary function as it is commonly done in clinical practice.
Define and measure slow vital capacity, tidal volume, inspiratory and expiratory reserve
volumes, total lung capacity, residual volume, forced vital capacity, FEV1 and FEV1
/FVC ratios in a normal human volunteer. Repeat these measurements under conditions
of simulated obstructive and restrictive lung disorders.
Compare results to each other and to normal human values. Discuss the implications of
these data for pulmonary function and its evaluation.
Reading
Before the lab, please review the laboratory description and the relevant pages in the text,
(Vander / Widmaier, 10th ed., Chap 13, pgs 491-494; 11th ed, Chap 13, pgs 454-457).
Introduction
The aim of these laboratory sessions is for you to gain first-hand experience of measurement in
respiratory physiology. The activities have been developed to consolidate the knowledge that
you acquired in class. Through understanding how certain physiological principles apply in
normal human subjects you will obtain insights into the problems that occur in patients with
respiratory disorders.
Apply yourself seriously and methodically to complete the lab in the allotted time. Provided that
you do this, you should find that the session is fun and instructive. It is the things that you do for
yourself that you will find easiest to remember, so get involved.
You will be confronted with a series of problems relating to the use of apparatus, methods of
measurement, calibration, and interpretation of results. This manual will enable you to solve the
problems systematically but it will not give you all the answers. Try to deduce for yourselves
how the experiment is intended to work and what important findings you are looking for.
Various members of the staff will be available during the laboratory. They will demonstrate the
use of the more complex pieces of equipment but they will not do the experiments for you or tell
you the answers.
Physiology 100 Laboratories
44
The purpose of these experiments is to characterize the mechanical properties of the lungs and
chest wall by examining the volume changes that accompany specific respiratory maneuvers.
You will measure vital capacity and its component lung volumes. Then you will study forced
expiratory maneuvers in the normal situation and under conditions which simulate obstructive
and restrictive lung disease.
IRV
ERV
Figure 1: Measurement of lung volumes using a water-seal spirometer.
Apparatus
You are provided with the following:
1
1
1
1
1
1
1
3
Mouthpiece
Sterile filter
Electronic spirometer with bi-directional turbine flow transducer
Computer with large screen for data acquisition, analysis and display
3-liter calibration syringe
Prediction table for FVC, FEV1 and FEV1/FVC
Rubber bung (stopper) with a small hole in the middle
Elastic bandages and clips
Physiology 100 Laboratories
45
Set-up and Demonstration
For many years we used traditional water seal spirometers for this laboratory. One of these
instruments is on display in the lab. It consists of a counterbalanced, hollow, cylindrical bell
riding in a bath of water. The volume of gas in the bell will increase as the subject exhales and
decrease as the subject inhales causing the bell to rise and fall, respectively. The vertical motion
of the bell is recorded on a motor-driven drum resulting in a plot of volume versus time or
spirogram (Figure 1). The beauty of this system was the visual impression of air moving
between the bell and the lungs directly resulting in the spirogram.
We now use a modern bi-directional turbine flow transducer mounted on an adjustable stand.
Please note that his instrument is very delicate and must be handled with the utmost care. The
turbine spins to and fro as the subject breathes in and out. Its speed of rotation is proportional to
the flow. The transducer output is connected to a computer that integrates the flow signal to give
volume changes that are then displayed in real-time as a plot of volume versus time. In other
words we see the same type of spirogram on the computer screen as shown in Figure 1.
The instructor will help you identify the parts of this spirometer system and discuss its
calibration with a 3-liter calibration syringe.
Grouping and Task Assignments
When instructed, you should divide up into groups of about 4 students. Each group will work
with their own spirometer. Each student within the group will have an assigned task for the
experiments. These tasks are:
Subject
The same subject will perform all the experiments for the group.
Commander
This person instructs and monitors the subject in the relevant tasks.
Equipment Supervisor
This person monitors the apparatus, inserts the rubber bung when
needed and leads the elastic strapping procedure.
Computer Operator
This person operates the computer system to acquire the data and leads
the data analysis.
All students will participate in the data analysis and interpretation.
Physiology 100 Laboratories
46
Preparation for the Experiments
Recording of Subject Characteristics
Prior to acquiring data from the subject, the group needs to gather some important information
from the subject in order to make predictions about their respiratory function. These data are age
and height. You can measure the subject’s height in centimeters using the meter stick placed at
the front of the adjacent classroom (don’t forget to add 100 cm for the displacement of the meter
stick from the floor), or you may calculate it by multiplying his/her known height in inches by
2.54. Fill in the required data on the top line of the data table (last page of the manual).
Derivation of Predicted Values
Using the separate chart of predicted values for Forced Vital Capacity (FVC) in healthy men and
women, obtain a "Predicted" FVC value for your subject. Record this value in the “Predicted”
column (#1) of your data table at the end of this manual. (Skip the shaded cells, as you do not
have sufficient information for them). Calculate the predicted value of Forced Expired Volume
in 1 second (FEV1) as 80% of predicted FVC (i.e. FVC x 0.8). The ratio is filled in for you.
You are now set to make measurements in your subject and to compare them with these
predicted values.
Experiment 1. Normal Breathing
Aim
The aim of this experiment is to measure pulmonary function as it is commonly done in clinical
practice.
Procedure for Normal Breathing, Tidal Volume (VT) and Slow Vital Capacity (SVC).
1.
2.
3.
4.
5.
The Equipment Supervisor obtains a clean mouthpiece and filter from the table and asks
the Subject to attach them to the flow transducer inlet as shown by the faculty instructor.
The Subject stands in front of the spirometer and adjusts the mouthpiece to a comfortable
position. The stand can be adjusted up and down at the base for course positioning with
fine positioning achieved with the flexible arm.
The Subject then puts on a nose clip so that all the air will pass through the mouth and
ultimately in and out of the spirometer transducer.
The Commander asks the Computer Operator to start recording.
The Computer Operator then toggles on the acquisition via the HEM program. He/she
should consult the computer command sheet for relevant commands and ask the faculty
instructor for guidance as needed.
Physiology 100 Laboratories
6.
7.
8.
47
Once the computer is recording, the Commander will ask the Subject to place his/her
mouth completely onto the mouthpiece and breathe normally. The traces on the computer
display should then move up and down.
Observe the rhythmical changes in lung volume on the display. These should be fairly
consistent in magnitude and timing; however there will be some variation from breath to
breath. If there is a large amount of variation or if the record drifts consistently up or
down (suggesting air leakage through the nose), the Commander should stop the subject
after about 30–40 seconds and start over.
Once consistent breathing is achieved for at least 4 breaths (this should not take more
than 12 breaths total!), the Commander will give the following instructions:
“After the next breath, breathe in all the way to fill your lungs. Hold the air in for just
a moment. Then breathe out all the way, to empty your lungs completely. Then return
to normal breathing for a couple of breaths.”
9.
10.
Note that this deep inhalation and exhalation should be done at a normal rate of
breathing. You should obtain a spirogram similar to that shown in Figure 1.
The Commander then tells the subject to step back from the spirometer and tells the
Computer Operator to stop acquisition.
With the assistance of the faculty instructor, the Computer Operator should adjust the
display time-base so that the entire spirogram is within the display. Again, it should
appear similar to that shown in figure 1. Print a copy for each student.
Analysis of Results
11.
12.
13.
Study the printed spirogram. Identify the end of expiration and mark this point as the
functional residual capacity (FRC). Mark the point of maximum inspiration as the total
lung capacity (TLC). Mark the point of maximal expiration as the residual volume
(RV).
Go to the data table locating the “Normal” column (#2). For the top box, calculate the
slow vital capacity (SVC) from the traces. Values are obtained directly from the screen
by left clicking the mouse on the point of interest. The HEM program gives the x & y
values. The “y” value is the calibrated volume at that point in time. The SVC is the
difference between the maximum and minimum values during the maneuver (SVC =
TLC – RV). You can measure this difference in volume on the computer screen even
though you did not determine absolute values for TLC and RV.
Next, determine the tidal volume (VT), expiratory reserve volume (ERV) and
inspiratory reserve volume (IRV) from your spirogram and fill the values in the
appropriate boxes on your data table. Refer to Figure 1 to understand the designation of
these values. Verify that SVC = ERV + VT + IRV.
Physiology 100 Laboratories
48
Procedure for Forced Vital Capacity (FVC) and Forced Expired Volume in One
Second (FEV1)
1.
2.
3.
When the group is ready to begin this next procedure, repeat steps 2-6 in the above
section on slow vital capacity (i.e. start computer recording, nose clip on subject, subject
on mouthpiece).
If the display trace is near the top or bottom of the screen, the Equipment Supervisor
needs to reset its position to the middle by toggling off/on the flow transducer power box.
You need to start near the middle of the screen to insure all the volume can be recorded.
After the subject has taken three or four normal (tidal) breaths, the Commander instructs
the subject as follows:
"On your next breath, exhale all the way to empty your lungs, then take a deep breath
to fill your lungs completely and HOLD IT."
4.
Once the trace on the screen has leveled off (flat) for 0.5-1.0 seconds, the Commander
must quickly give the following, instruction:
“BLOW! –as hard as you can and keep going … keep going … keep going.”
5.
6.
7.
At this point, the subject should breathe out as fast as he/she can and keep going until
his/her lungs feel empty. The entire group should encourage the subject in his/her effort
by vigorously chanting, “Blow! Blow! Blow!” until the subject is forced to inhale.
When this maneuver is complete, the Commander asks the subject to step back from the
spirometer and tells the Computer Operator to stop acquisition.
As before, the Computer Operator should adjust the display time-base so that the entire
spirogram from the forced maneuver is within the display. The tracing should have a flat
top, a sharp corner at the start of the forced expiration, and a smooth exponential curve
during the forced expiration. Check with the faculty instructor. Repeat if necessary. Print
a copy for each student.
Analysis of Results
8.
9.
10.
11.
12.
Study the spirogram of the forced expiratory maneuver. Use the computer mouse as
before but this time measure the forced vital capacity (FVC) from TLC to the horizontal
portion towards the end of the forced maneuver (RV). Go to the data table and locate the
“Normal” column (#2). Fill in the appropriate box in the table.
Compare your measured FVC with the predicted value for your subject. Compare FVC
with SVC. If they are different, consider why this might occur.
Determine the forced expired volume in the first second (FEV1). In this case, take the
mouse and hold down the left button and drag it from the inflection point at the start of
the forced maneuver and drag it to the right until the “x” value = 1 second. Determine the
“y” value on the curve at that point for FEV1. Fill in the appropriate box in the table.
Compare your measured FEV1 with the predicted value. Are they similar?
Calculate the forced expiratory ratio (FEV1/FVC) and fill in the box in the table. How
does this value compare with the expected ratio of 80%?
Physiology 100 Laboratories
49
Experiment 2. Simulated Obstruction
Aim
During this experiment you will "obstruct" airflow by introducing a resistance into the
mouthpiece and record the effects on the pattern of volume changes during the same respiratory
maneuvers.
Procedure
1.
2.
3.
4.
The Equipment Supervisor should locate the rubber bung (stopper) and help the Subject
insert it so that it lies completely within the neck of the mouthpiece. You will have to
remove the mouthpiece from the filter to do this; the feat is most easily accomplished if
the bung is inserted into the end of the mouthpiece that attaches to the filter, shoving in
the small end of the bung first. Reattach to the filter.
Repeat the sequence of tidal breathing followed by the forced vital capacity maneuver as
described in # 3-6 of the section on performance of the FVC above.
When the maneuver with the bung in place is complete, toggle off the program and allow
the subject to rest.
Review the tracing with the faculty instructor. It should look different from the previous
“normal” tracing. Repeat the maneuver if necessary.
Analysis of Results
5.
6.
7.
If the faculty instructor approves, analyze the tracing as described above to determine
FVC, FEV1 and FEV1/FVC. Tabulate your results in the “Obstruction” column of the data
table below.
Compare these values with the normal situation noting any similarities and differences.
When completed, the Equipment Supervisor should remove the rubber bung from the
mouthpiece before the next study.
Physiology 100 Laboratories
50
Experiment 3: Simulated Restriction
Aim
During this experiment you will "restrict" the movements of the chest wall by strapping the rib
cage, shoulders, and abdomen, and recording the effects on the pattern of volume changes during
the same respiratory maneuvers.
Procedure
1.
2.
3.
4.
5.
6.
The Equipment Supervisor should lead the strapping procedure.
Ask the subject to breathe shallowly. Quickly wrap the short, heavy elastic bandage
tightly around the subject’s waist and secure it with the Velcro strip (if accessible) or
with a safety pin. Next, bind the chest wall tightly by winding the two elastic bandages
around the lower rib cage and upper abdomen and the shoulders as shown by the faculty
instructor. Be sure to bring the bandage over the shoulder towards the lateral end rather
than by the neck. Secure all the bandages tightly. Note that the subject might feel
somewhat uncomfortable during this part of the experiment so your aim is to get
completed quickly.
Repeat the sequence of tidal breathing followed by the forced vital capacity maneuvers
as described in # 3-6 of the section on performance of the FVC above.
When the maneuver with the binding in place is complete, toggle off the program and
quickly review the tracing with the instructor. It should look different from the previous
“normal” tracing. Repeat the maneuver if necessary.
If the faculty instructor approves, immediately release the subject from the bindings and
roll them up leaving them as you found them.
The Equipment Supervisor needs to remind the Subject to place the rubber mouthpiece,
rubber bung and nose clip in the wash basin. Do Not Throw them Away! You may throw
away the filter.
Analysis of Results
7.
8.
Analyze the tracing as described before to determine FVC, FEV1 and FEV1/FVC.
Tabulate your results in the “Restriction” column of the data table below.
Compare these values with the normal situation noting any similarities and differences.
Physiology 100 Laboratories
51
Data Table
SUBJECT AGE: _____
Predicted
GENDER: F
Normal
M
HEIGHT: _________ cm
Obstruction
SVC
TV
ERV
IRV
FVC
FEV1
FEV1/FVC
0.80
Discuss these results among yourselves and with the instructor.
Restriction
Physiology 100 Laboratories
52