Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drosophila melanogaster wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
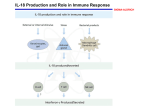
DOI: 10.1093/humrep/deh356 Human Reproduction Vol.19, No.9 pp. 1968–1973, 2004 Advance Access publication June 10, 2004 Detectable levels of interleukin-18 in uterine luminal secretions at oocyte retrieval predict failure of the embryo transfer N.Lédée-Bataille1,2,4, F.Olivennes3, J.Kadoch3, S.Dubanchet1, N.Frydman3, G.Chaouat1 and R.Frydman2 1 INSERM U131, Equipe Cytokines et Relation Materno-Fœtale Clamart, France, 2E.A 3538, qualité gamétique et implantation, Clamart, France and 3Service de Gynécologie-Obstétrique et Médecine de la Reproduction, Hôpital Antoine Béclère, Clamart, France 4 To whom correspondence should be addressed at: Service de Gynécologie-Obstétrique, Centre Hospitalier de poissy, 10, Rue du Champ Gaillard, 78300 Poissy, France. E-mail: [email protected] BACKGROUND: Most implantation failures after successful in vitro fertilization-embryo transfer (IVF-ET) result from inadequate uterine receptivity. There is currently no way to predict this receptivity. METHODS: We investigated whether the detection of interleukin-(IL)18 by ELISA in uterine luminal secretions might predict implantation failure. Secretions of 133 patients enrolled in our IVF-ET program were sampled by uterine flushing immediately before oocyte retrieval. We assessed the following outcomes: pregnancy rate, multiple pregnancy rate, and implantation rate per embryo transferred. RESULTS: Interleukin-18 was detected in the flushing fluid of 38 patients (28.6%). Although the two groups were comparable for all other characteristics (age, etiology, ovarian reserve, number of embryos transferred, quality of embryos), all outcome variables differed significantly. The pregnancy rate was 37.9% in the IL-18 2ve group and 15% in the IL-18 1 ve group, the multiple pregnancy rate 27.7% and 0%, and the implantation rate per embryo transferred 19.4% and 6.7% (all comparisons, P 5 0.02). Only embryos meeting good quality criteria were transferred to 65 patients: 50 IL-18 2ve and 15 IL-18 1ve. The pregnancy rate was 51% for the IL-18 2ve group and 20% for the IL-18 1ve group, the multiple pregnancy rate 36% and 0.0%, respectively, and the implantation rate 29% and 8.3% (P 5 0.02). CONCLUSION: This noninvasive and simple method predicted inadequate uterine receptivity, independent of embryo quality. Key words: cytokines/implantation/interleukin-18/in vitro fertilization/embryo transfer (IVF-ET)/uterine flushing/uterine receptivity Introduction The implantation process, a complex and poorly understood phenomenon, is currently the most critical problem in reproductive medicine, especially in assisted reproductive technology (ART). Only 15 to 20% of the embryos transferred after in vitro fertilization (IVF) lead to the birth of a healthy baby (ASRM/SART, 2002). When the quality of the embryo is good, most implantation failures are imputable to inadequate uterine receptivity (Smart et al., 1982; Simon et al., 1998) and occur during the peri-implantation period (Racowsky, 2002). Progress in improving the rate of implantation depends on a better understanding of the mechanisms underlying its success or failure. Because of the low implantation rate after IVF and embryo transfer (IVF-ET), multiple embryos are usually transferred simultaneously to increase the likelihood of obtaining a pregnancy. This practice unfortunately also increases the rate of multiple pregnancies. In 1998, the percentage of multiple pregnancies reported after IVF-ET was 26.3% in Europe and 38% in North America (Toner, 2002). ART practitioners 1968 have long known that multiple pregnancies cause significant maternal and especially fetal risk, in addition to their high financial costs (Gardner et al., 2000; Gerris and Van Royen, 2000; Fanchin, 2001). The study of uterine receptivity in humans relies primarily on non-invasive methods such as ultrasound exploration, but their predictive value and reproducibility are limited (Fanchin, 2001). New methods are clearly needed to assess uterine receptivity. Possible candidates include the measurement of various molecules involved in implantation, sampled by uterine flushing or endometrial biopsy (Laird et al., 1997). Mediators such as metalloproteases (Bischof, 2001), integrins (Lessey et al., 1996) and cytokines (Delage et al., 1995; Simon et al., 1995) have been successfully quantified with these procedures. Cytokines are among the most important of those mediators: implantation is controlled mainly, although not exclusively, by locally acting growth factors and cytokines, some under steroid control (Giudice, 1994; Tabibzadeh et al., 1995). The steroid hormones may initiate a downstream cascade of molecular events through local Human Reproduction vol. 19 no. 9 q European Society of Human Reproduction and Embryology 2004; all rights reserved IL-18 in uterine secretion predicts IVF failure paracrine/autocrine molecules; these events include the intricate and entwined mechanisms of uterine receptivity and preimplantation embryo development. IL-18 in vitro induces IFN-g and aberrant matrix metalloproteinase activity in the presence of IL-12. In its absence, IL-18 causes the production of anti-inflammatory cytokines, such as IL-4 and IL-13 (Smeltz et al., 2001; Abraham et al., 2002). The administration of either IL-18 or IL-12 is abortifacient in mice (Kawamura et al., 1998; Hayakawa et al., 1999). Thus, IL-18 induces both Th-1 and Th-2 cells, depending on the local environment. Its pivotal role in the Th1/Th2 balance (Lewkowich et al., 2002), its presence in the endometrium (Yoshino et al., 2001) and its detrimental effects during pregnancy (Ida et al., 2000) suggested to us that its level in uterine luminal secretions might function as an indicator of the cytokine environment. Cytokines are not usually measured in uterine secretions during cycles in which treatment procedures and IVF-ET take place, for fear that direct access to the uterine cavity might adversely affect the chance of pregnancy. Results are thus extrapolated to other cycles, i.e. considered to remain consistent. Because clear evidence shows that an individual’s cycles vary in many ways, however, consistency cannot be presumed. Once we had conducted a preliminary study to confirm the safety of the procedure of uterine flushing performed at oocyte retrieval (i.e. during the treatment cycle, 48 h before embryo transfer) for implantation and pregnancy rates (Olivennes et al., 2003), we were able to attempt to correlate the levels of some molecular mediators with the cycle outcome. We used ELISA to assess the IL-18 concentration in luminal uterine secretions at oocyte retrieval of 140 patients enrolled in our IVF program. At the same time, we measured the IL-18 concentration in follicular fluid (pooling the fluid for all follicles for each woman) for 50 of them. The study outcomes were the rates of pregnancy and implantation following those IVF-ET cycles. Methods Patients Between July 2001 and July 2002, 140 patients enrolled in our IVF program underwent a uterine flushing during the same procedure as, but immediately before, oocyte retrieval. The choice of patients, while not random, was essentially arbitrary: it depended on whether two specific physicians (F.O., J.K.) were performing the procedure. We included only patients with controlled ovarian hyperstimulation before the IVF procedure. All patients enrolled in the program had previously undergone hysteroscopy and ultrasound assessment of their uterine cavity to measure its size and assess any particularities. Patients with tumors, a septate uterus, or any other uterine malformations were excluded. All patients provided informed consent, and our Institutional Review Board approved this investigation (CCPPRB, protocol 01 – 78). Protocol for the controlled ovarian hyperstimulation Most patients (71.4%, n ¼ 100) received a standard gonadotrophinreleasing hormone agonist (GnRH-ag) regimen, beginning on day 21 of a spontaneous menstrual cycle. Leuprolide acetate (1 mg per day, Lucrin, Takeda Pharmaceuticals, Paris, France) was administered subcutaneously for 10 – 14 days, until complete suppression of pituitary activity. The remaining 40 patients (21.8%) received a GnRH antagonist (Cetrotide, Serono, France) during stimulation, without prior pituitary desensitization. Stimulation began once serum oestradiol was , 50 pg/ml and sonographic evidence indicated no follicular activity and an endometrial lining ,5 mm thick. Recombinant (rFSH: Puregon, Organon Pharmaceuticals, Saint Denis, France or Gonal F, Serono, France) or purified urinary gonadotrophin (FSH-LH: Menopur, Ferring, France) treatment then began, at a daily dose of 225 IU, subcutaneous. The duration of these doses depended on the standard criterion of follicular maturation, assessed by both ultrasound and serum oestradiol measurements. HCG (‘endo’ chorionic gonadotrophin; Organon Pharmaceuticals, Saint Denis, France, 10000 IU, intramuscular) was administered when at least three follicles were mature (. 17 mm in diameter) and the estrogen level per mature follicle was .250 pg/ml. Thirty-six hours after HCG administration, the uterine flushing was performed as described below and oocytes were retrieved by needle aspiration, with transvaginal ultrasound guidance under intravenous sedation or local anesthesia. All patients received antifungus pessaries (Gynomyk, Labo, France, two doses vaginally) the day before and the morning of oocyte retrieval and an intravenous bolus of antibiotics (amoxicillin and clavulanic acid, Augmentin, Adventis, France, 1 g) during the procedure. For 50 women, we also kept a sample of follicular fluid, pooled from all the follicles used. The uterine flushing and follicular fluids were stored separately at 2 208C in mini-vials until IL-18 measurement by ELISA. All patients received the same treatment after oocyte retrieval: micronized progesterone (Utrogestan; Besins-Iscovesco Pharmaceuticals, Paris, France) (400 mg daily, vaginally) and ciprofloxacin (Ciflox, Adventis, France) (1000 mg daily for 5 days). Embryo quality was evaluated according to the regularity of the blastomere and the percentage of fragmentation (Veeck, 1990). The blastomeres in grades A and B were even, with no fragmentation in grade A and , 20% in grade B. Both were defined as good-quality embryos. Grade C had either uneven blastomeres or . 20% fragmentation, and grade D . 50%. Of 140 patients who underwent uterine flushing, 133 had an embryo transfer on day 2 or 3. Uterine flushing The uterine flushing took place just before the oocyte retrieval and before intravenous sedation or local anesthesia. All information about difficulties in accessing the uterus were recorded, so that the flushing also served as a dry run for the embryo transfer 48 h later. The in vivo method for uterine flushing is neither painful nor invasive. As we have described previously, we gently insert an embryo transfer catheter (Frydman catheter, CCD Laboratories, Paris, France), connected to a 10 ml syringe. We then instill 1 ml of saline water, immediately and gently aspirate it, and repeat these two steps. The low quantity and lack of viscosity of the saline water instilled minimizes leakage (Ledee-Bataille et al., 2002; Olivennes et al., 2003). The liquid was then stored for 140 patients at 2 208C in minivials until the assays. Flushing samples were discarded before storage in 15% of the cases because either its fluid volume was too small (, 200 ml) or it contained mucus. Cytokine assays Il-18 concentrations in uterine flushing and follicular fluids were assayed by enzyme-linked immunosorbent assay (ELISA) according to the manufacturer’s instructions (Quantitine Human IL-18 ELISA kit, R&D, ref no. 7620). This test had a sensitivity limit of 12.5 pg/ml. Intra-assay coefficients of variation were 4.45, 3.55 1969 N.Lédée-Bataille et al. Table I. Clinical patients’ characteristics Group IL-18 2ve n ¼ 100 (%) Mean [IL-18] pg/ml IL-18 þ ve n ¼ 40 (%) Mean [IL-18] pg/ml No. of patients and mean [IL-18] (pg/ml) Age Parity Nulliparity Primiparity 100 33 ^ 0.4 90 (90%) 10 (10%) 0 40 32 ^ 0.6 47 (92%) 3 (8%) 63 ^ 10 Etiology Male factors Permanent tubal factors Partial tubal factors Endometriosis Unexplained infertility Preimplantation diagnosis No. of previous attempts FSH on Day 3 (mIU/ml) E2 on Day 3 (pg/ml) 48 (48%) 16 (16%) 9 (9%) 5 (5%) 14 (14%) 8 (8%) 2 ^ 0.3 6 ^ 2 0.2 36 ^ 3 0 0 0 0 0 0 0 0 17 (45%) 4 (10%) 4 (10%) 5 (12.5%) 5 (12.5%) 4 (10%) 2 ^ 0.1 6 ^ 0.3 26 ^ 3 60 ^ 15 48 ^ 10 66 ^ 16 41 ^ 7 78 ^ 28 39 ^ 10 86 ^ 30 23 ^ 7 140 patients underwent in vitro fertilization. The clinical characteristics of patients with detectable IL-18 in their uterine flushing fluid (IL-18 þ ve: 40 patients) were compared with those without (IL-18 2ve: 100 patients). The details of the respective etiology in each group is described with the correspondent mean and standard error of IL-18 in each group. The two groups were comparable for all the indicators we examined. We did not observed statistical differences in function of the etiology. and 4.59%, respectively, for IL-18 at concentrations of 80, 400 and 1000 pg/ml and Inter-assay coefficients of 4.26, 3.42 and 1.02%. For calculating purposes, samples with a concentration below that limit were assumed to contain 0 pg/ml of IL-18. Statistical analysis The results were expressed as the mean ^ standard error. All variables for the IL-18 þve and IL-18 2 ve groups were compared with a standard Student’s t-test, run under StatView software (Abacus Concepts, Inc., Berkeley, CA). Clinical pregnancy was defined by ultrasound identification of at least one gestational sac with cardiac activity; it did not include biochemical pregnancy. The pregnancy rate was defined as the ratio of the number of clinical pregnancies to the number of transfers, and the implantation rate, the ratio of the number of gestational sacs to the number of embryos transferred. A P-value of 0.05 or less was considered significant. Results IL-18 was detected in the flushing fluid of 40 of the 140 samples tested (28.57%) (IL-18 þ ve group). The mean IL-18 concentration in this group was 63.42 ^ 10 pg/ml (14 – 330). The IL-18 þ ve group did not differ significantly from the IL-18 2 ve group for any other variables except outcomes. Their clinical profiles (age, ovarian reserve, parity, number of IVF attempts, causes of sterility) were non significantly different and are detailed in Table I. However, among patients with detectable IL-18, the higher concentrations of IL-18 were described for patients with idiopathic and partial tubal sterility (none had hydrosalpinx diagnosed at the ultrasound evaluation). In contrast, the lowest concentrations were traced in those fertile patients who were enrolled in IVF for preimplantation diagnosis. However, the observed differences were not significant. The protocols used for the controlled ovarian hyperstimulation, the respective hormonal and biological responses in the IL-18 þ ve and 2 ve groups are detailed in Table II. In patients with IL-18 detectable, the concentration of IL-18 was not significantly higher in those patients who received an 1970 antagonist protocol than in patients who received GnRH agonist (P ¼ 0.77). IL-18 þ ve and 2 ve groups did not differ for the number of oocytes collected, the number of embryos produced, or the number of embryos transferred. Even the quality of the embryos was the same. Embryos were transferred into 95 of the 100 IL-18 2 ve patients and 38 of the 40 IL-18 þ ve patients. The outcome, however, differed dramatically according to whether IL-18 was detectable (Table III). The clinical pregnancy rate was 16% in the IL-18 þ ve group and 38% in the IL-18 2 ve group (P ¼ 0.02), and the implantation rates were 6.7% and 19% respectively (P ¼ 0.02). As expected, embryo quality also affected pregnancy rates significantly: they were best (47.75%) among the 65 patients with only good-quality embryos (grade A or B) transferred, and intermediate (34%) among the 40 patients with mixed embryos transferred (AB þ CD). No pregnancies occurred among the 35 patients who had only low-quality embryos (grade C or D). Of the 65 patients who had only good quality embryos transferred, 15 were IL-18 þ ve and 50 IL-18 2 ve. In this subgroup, for which embryo quality was controlled, the implantation rate also differed dramatically according to IL-18 status: 8.3% in the IL-18 þ ve group compared with 29% in the IL-18 2 ve group (P ¼ 0.02). The multiple pregnancy rates were respectively 0% and 36% (P ¼ 0.03). The sensitivity of the detection of IL-18 to not predict further pregnancy or multiple pregnancy is high: 85% and 100%, respectively. But the specificity of the detection of IL-18 for the pregnancy and multiple pregnancy rate is low (no detection of IL-18 does not predict pregnancy): 35% and 34%, respectively. The detection of IL-18 has a high negative predictive value for further pregnancy but a poor positive predictive value. The mean concentration of Il-18 in the follicular fluid from 51 samples was 240 ^ 96 pg/ml. However only six IL-18 in uterine secretion predicts IVF failure Table II. Characteristics of the ovarian hyperstimulation Group Protocol GnRH Agonist protocol GnRH antagonist E2 Day HCG (pg/ml) Endometrial thickness (mm) No. of oocytes collected No. of embryos of quality A þ B transferred No. of embryos of quality C þ D transferred No. of embryos transferred No. of patients with transfers IL-18 2ve [IL-18] pg/ml IL-18 þve [IL-18] pg/ml 74 (74%) 26 (26%) 2808 ^ 182 9 ^ 0.35 10 ^ 0.7 2 ^ 0.2 1.1 ^ 0.2 2.6 ^ 0.1 95 0 0 26 (65%) 14 (35%) 2444 ^ 109 9 ^ 0.1 9 ^ 0.5 2 ^ 0.1 0.9 ^ 0.24 2.6 ^ 0.1 38 73 ^ 16 49 ^ 9 P-value (t-test) 0.71 0.89 0.46 0.56 0.24 0.8 140 patients underwent in vitro fertilization. The characteristics of the ovarian stimulation (protocol, concentration of IL-18, ovarian response) of patients with detectable IL-18 in their uterine flushing fluid (IL-18 þ ve: 40 patients) were compared with those without (IL-18 2ve: 100 patients). The repartition for the agonist and antagonist protocols in each group is detailed with the correspondent mean and standard error of IL-18. The two groups were comparable for all the indicators we examined. Neither was there a statistical difference in the protocol used (P ¼ 0.29). Table III. Outcome Group All patients transferred (n = 133) IL-18 2ve 95 IL-18 þ ve 38 P-value Implantation Rate Pregnancy rate Multiple pregnancy Rate Transfer of only embryos A þ B (n = 65) Implantation Rate Pregnancy rate Multiple Pregnancy rate Transfer of only embryos C þ D (n ¼ 35) Implantation Rate Pregnancy rate 19.4% 37.8% 27.7% 50 6.7% 15.7% 0% 15 0.02 0.02 0.04 0.02 29% 51% 36% 26 8.3% 20% 0% 9 0.04 0.03 0% 0% 0% 0% NS NS NS Implantation Rate (IR), Pregnancy Rate (PR) and Multiple Pregnancy Rate (MPR) are reported for patients in the IL-18 þ ve and 2ve groups. IR is calculated independently of embryo quality, when only embryos of quality A þ B were transferred and when only embryos of quality C þ D were transferred. patients with detectable uterine luminal IL-18 were evaluated for their follicular fluid IL-18 concentration versus 45 in the group with no luminal IL-18 detectable. We thus could not conclude if IL-18 concentration in follicular fluid differed according to whether the patient’s uterine flushing contained IL-18. The concentration of IL-18 however in the uterine flushing fluid was not significantly correlated with that in the follicular fluid for the six patients observed. Follicular fluid concentration was not correlated to the basal FSH level, the number of oocytes collected, the embryos number or quality and the implantation rate. Discussion The detection of IL-18 in the uterine lumen, i.e. at the time of oocyte retrieval, 48 h before embryo transfer, is associated with a poor implantation rate. To understand this finding, we must consider here the implications of the presence of this cytokine. We begin by assuming that the IL-18 detected in the flushing liquid is of local origin, i.e. secreted by the uterus. IL-18 is synthesized as a 24 kDa molecule that requires cleavage by IL-1 converting enzyme (ICE, also known as caspase-1) to generate a biologically active 18 kDa monomer (Ghayur et al., 1997; Gu et al., 1997). These functions are mediated through the IL-18 receptor (IL-18R), which is identical in sequence to a member of the IL-1 receptor family previously designated IL-1 receptor-related protein (Torigoe et al., 1997). A constitutively secreted and soluble binding protein for IL-18 was recently purified from human urine (IL-18 BP) (Novick et al., 1999). It neutralizes IL-18 effector functions (Novick et al., 1999). Yoshino et al. (2001) report that the complete system is present in the human endometrium. In contrast to other pro-inflammatory cytokines, which are expressed cycle-dependently and usually peak in the luteal phase, expression of the IL-18 family (IL-18, IL-18R, IL-18BP) shows no characteristic variations during the menstrual cycle (Yoshino et al., 2001). Expression of the IL-18 protein appears to occur mainly in endometrial epithelial cells, almost entirely as its 24 kDa precursor protein, which is biologically inactive and is not secreted unless it undergoes cleavage (Yoshino et al., 2001). Nonetheless, the mature IL-18 protein may be secreted by some human epithelial cells in situations such as Chlamydia trachomatis infection (Lu et al., 2000). Because the percentage of tubal sterility was equal (23%) in the Il-18 þ ve and IL-18 2 ve groups in our series, this factor is not exclusive to explain the differences observed. However, the high IL-18 concentrations observed in some patients in the partial tubal and unexplained infertility groups, suggest that these patients should be tested for existence of a latent Chlamydia infection and then, if positive, accordingly treated. However, the five patients with unexplained infertility and a high IL-18 luminal concentration were negative for C. trachomatis. This suggests that this etiology is not exclusive and that some underlying uterine dysregulation should also be searched for. Detection of Il-18 in the uterine lumen suggests that local factors not yet defined induce the transformation of pro-IL-18 into mature IL-18 and then modify the local environment. We thus hypothesize that detectable level of IL-18 in the uterus reveals a pre-implantation stage-specific 1971 N.Lédée-Bataille et al. defect in the implantation process that results in improper uterine preparation and thus inadequate receptivity during the implantation window. IL-18 was initially described as an interferon (IFN)-g inducing factor in human that acts in synergy with IL-12 to enhance the cytotoxic activity of human natural killer (NK) cells and promote T-helper 1 (Th-1) response by production of TNF and IFNg (Nakamura et al., 1989; Matikainen et al., 2001). In mice, high NK activity (cytostatic or cytotoxic), high levels of LFN-g or TNF and low levels of such Th-2 cytokines as IL-10 are known to be abortifacient (Chaouat et al., 1995). Studies on animal model also shown that IL-18 was able limit the induction of type 2 immunity in vivo (Lewkowich et al., 2002) and leads to aberrant matrix metalloproteinase (MMP) activity with IL-12 (Abraham et al., 2002). We can therefore hypothesize that detectable IL-18 in the uterus at the time of oocyte retrieval indicates cytotoxic NK cell activity, accompanied by dysregulation of both type 2 immunity and MMP activity; both of these are associated with implantation failure (Lin et al., 1993; Wegmann et al., 1993; Chaouat et al., 1995). This outline, attractive as it seems, may nonetheless be too simplistic in view of the complexity of the IL-18 system (Hoshino et al., 2001). Indeed, IL-18 has been demonstrated to be positively involved in the implantation process in mice (Ostojic et al., 2003) and human (Lédée-Bataille et al., in press). Furthermore, vascular remodeling of the spiral arteries appears to require IL-18 activity to stimulate NK cells to produce angiopoietin-2 (Croy et al., 2000, 2003). The effects of Il-18 are highly dependent on the presence (and absence) of other cytokines (amongst which IL-12 and IL-4 have been most studied). The presence, quantity and ratio of these cytokines determine whether IL-18 shifts the immune system towards differentiation of Th-2 cells or promotes Th-1 cell proliferation (Smeltz et al., 2001). IL-18 BP (mostly expressed in endometrial stromal cells) can also decrease IL-18 activity by reducing IFN-g-mediated responses (Reznikov et al., 2000). A complete interpretation of our results therefore requires further documentation of other cytokines, including IL-12 and IL-18BP (an IL-18 antagonist), by simultaneous human endometrial biopsy. The expression of the cytokines in the uterine luminal compartment does not reflect the evolving complexity of the endometrial cytokine network itself but is a selection of one type of expression/secretion in a specific phase of the cycle. As for leukaemia inhibitory factor (LIF), intrauterine secretion of these cytokines, by the uterine epithelium in the pre-implantation period, may not reflect the situation in the peri-implantation/immediate post-implantation period, in the endometrium itself, especially right around spiral arteries (Ledee-Bataille et al., 2002). Regardless of the underlying pathology, however, excess luminal IL-18 constitutes for the clinician an immunological marker that can predict implantation failure with a significant degree of accuracy (strong negative predictive value and specificity) and is detectable relatively rapidly by a noninvasive method before embryo transfer. Furthermore, this 1972 marker is predictive independently of embryo status, another factor that strongly affects implantation rates. Its detection should invite the clinician in case of failure to further uterine exploration especially in context of unexplained sterility or partial tubal sterility in order to enhance the uterine receptivity. As is the case for most of the markers of uterine receptivity, detection of IL-18 has a poor positive predictive value and sensitivity since others factors as the embryo quality will interact to predict the pregnancy. The absence of detection of IL-18 should therefore be associated with these others prognosis parameters to evaluate the risk of multiple pregnancy. Today, most policies to reduce the percentage of multiple pregnancies either select the best embryo to transfer by predefined criteria (the TOP embryo), (Gerris et al., 2000) or by in vitro culture until the blastocyst stage (Gardner et al., 2000; Schoolcraft et al., 2001). Combining this approach of embryo selection with assessment of the local cytokine environment in the uterine cavity could theoretically improve our transfer strategies: we might either reduce the number of embryos transferred if they are of good quality and IL-18 is not detected (high risk of multiple pregnancy) or choose either to freeze them or to replace up to three embryos if IL-18 is detected and the embryos quality non optimal (low risk of multiple pregnancy). In the near future, we will understand the full significance and origin of this IL-18 dysregulation and be able to propose adequate molecular corrections. Acknowledgements We thank Jo Ann Cahn for revising the manuscript. This work was supported by INSERM and the Fondation de la Recherche Médicale. References ASRM/SART (2002) Assisted reproductive technology in the United States: 1999 results generated from the American Society for Reproductive Medicine/Society for Assisted Reproductive Technology Registry. Fertil Steril 78,918–931. Abraham M, Shapiro S, Lahat N and Miller A (2002) The role of IL-18 and IL-12 in the modulation of matrix metalloproteinases and their tissue inhibitors in monocytic cells. Int Immunol 14,1449–1457. Bischof P, Meisser A and Campana A (2001) Biochemistry and molecular biology of trophoblast invasion. Ann NY Acad Sci 943,157–162. Chaouat G, Assal Meliani A, Martal J, Raghupathy R, Elliot J, Mosmann T and Wegmann TG (1995) IL-10 prevents naturally occurring fetal loss in the CBA £ DBA/2 mating combination, and local defect in IL-10 production in this abortion-prone combination is corrected by in vivo injection of IFN-tau. J Immunol 154,4261–4268. Croy BA, Ashkar AA, Minhas K and Greenwood JD (2000) Can murine uterine natural killer cells give insights into the pathogenesis of preeclampsia? J Soc Gynecol Investig 7,12–20. Croy BA, Esadeg S, Chantakru S, van den Heuvel M, Paffaro VA, He H, Black GP, Ashkar AA, Kiso Y and Zhang J (2003) Update on pathways regulating the activation of uterine Natural Killer cells, their interactions with decidual spiral arteries and homing of their precursors to the uterus. J Reprod Immunol 59,175–191. Delage G, Moreau JF, Taupin JL, Freitas S, Hambartsoumian E, Olivennes F, Fanchin R, Letur-Konirsch H, Frydman R and Chaouat G (1995) In-vitro endometrial secretion of human interleukin for DA cells/leukaemia inhibitory factor by explant cultures from fertile and infertile women. Hum Reprod 10,2483–2488. Fanchin R (2001) Assessing uterine receptivity in 2001: ultrasonographic glances at the new millennium. Ann NY Acad Sci 943,185– 202. IL-18 in uterine secretion predicts IVF failure Gardner DK, Lane M, Stevens J, Schlenker T and Schoolcraft WB (2000) Blastocyst score affects implantation and pregnancy outcome: towards a single blastocyst transfer. Fertil Steril 73,1155–1158. Gerris J and Van Royen E (2000) Avoiding multiple pregnancies in ART: a plea for single embryo transfer. Hum Reprod 15,1884–1888. Ghayur T, Banerjee S, Hugunin M et al. (1997) Caspase-1 processes IFNgamma-inducing factor and regulates LPS-induced IFN-gamma production. Nature 386,619–623. Giudice LC (1994) Growth factors and growth modulators in human uterine endometrium: their potential relevance to reproductive medicine. Fertil Steril 61,1–17. Gu Y, Kuida K, Tsutsui H, Ku G et al. (1997) Activation of interferongamma inducing factor mediated by interleukin-1beta converting enzyme. Science 275,206– 209. Hayakawa S, Nagai N, Kanaeda T, Karasaki-Suzuki M, Ishii M, Chishima F and Satoh K (1999) Interleukin-12 augments cytolytic activity of peripheral and decidual lymphocytes against choriocarcinoma cell lines and primary culture human placental trophoblasts. Am J Reprod Immunol 41,320–329. Hoshino T, Kawase Y, Okamoto M, Yokota K, Yoshino K, Yamamura K, Miyazaki J, Young HA and Oizumi K (2001) Cutting edge: IL-18-transgenic mice: in vivo evidence of a broad role for IL-18 in modulating immune function. J Immunol 166,7014–7018. Ida A, Tsuji Y, Muranaka J, Kanazawa R, Nakata Y, Adachi S, Okamura H and Koyama K (2000) IL-18 in pregnancy; the elevation of IL-18 in maternal peripheral blood during labour and complicated pregnancies. J Reprod Immunol 47,65–74. Kawamura T, Takeda K, Mendiratta SK, Kawamura H, Van Kaer L, Yagita H, Abo T and Okumura K (1998) Critical role of NK1 þ T cells in IL-12-induced immune responses in vivo. J Immunol 160,16–19. Laird SM, Tuckerman EM, Dalton CF, Dunphy BC, Li TC and Zhang X (1997) The production of leukaemia inhibitory factor by human endometrium: presence in uterine flushings and production by cells in culture. Hum Reprod 12,569–574. Lédée-Bataille N, Lapree-Delage G, Taupin JL, Dubanchet S, Frydman R and Chaouat G (2002) Concentration of leukaemia inhibitory factor (LIF) in uterine flushing fluid is highly predictive of embryo implantation. Hum Reprod 17,213–218. Lédée-Bataille N, Dubanchet S, Bonnet-Chea K, Coulomb-L’hermine, Durand-Gasselin I, Frydman R and Chaouat G (2004) A new role for Natural Killer cells, IL-12 and IL-18 in repeated implantation failure after IVF-ET? Fertil Steril (in press). Lessey BA, Ilesanmi AO, Lessey MA, Riben M, Harris JE and Chwalisz K (1996) Luminal and glandular endometrial epithelium express integrins differentially throughout the menstrual cycle: implications for implantation, contraception, and infertility. Am J Reprod Immunol 35,195– 204. Lewkowich IP and HayGlass KT (2002) Endogenous IFN-gamma and IL-18 production directly limit induction of type 2 immunity in vivo. Eur J Immunol 32,3536–3545. Lin H, Mosmann TR, Guilbert L, Tuntipopipat S and Wegmann TG (1993) Synthesis of T helper 2-type cytokines at the maternal-fetal interface. J Immunol 151,4562–4573. Lu H, Shen C and Brunham RC (2000) Chlamydia trachomatis infection of epithelial cells induces the activation of caspase-1 and release of mature IL-18. J Immunol 165,1463–1469. Matikainen S, Paananen A, Miettinen M, Kurimoto M, Timonen T, Julkunen I and Sareneva T (2001) IFN-alpha and IL-18 synergistically enhance IFN-gamma production in human NK cells: differential regulation of Stat4 activation and IFN-gamma gene expression by IFN-alpha and IL-12. Eur J Immunol 31,2236–2245. Nakamura K, Okamura H, Wada M, Nagata K and Tamura T (1989) Endotoxin-induced serum factor that stimulates gamma interferon production. Infect Immun 57,590–595. Novick D, Kim SH, Fantuzzi G, Reznikov LL, Dinarello CA and Rubinstein M (1999) Interleukin-18 binding protein: a novel modulator of the Th1 cytokine response. Immunity 10,127–136. Olivennes F, Ledee-Bataille N, Samama M, Kadoch J, Taupin JL, Dubanchet S, Chaouat G and Frydman R (2003) Assessment of leukemia inhibitory factor levels by uterine flushing at the time of egg retrieval does not adversely affect pregnancy rates with in vitro fertilization. Fertil Steril 79,900–904. Ostojic S, Dubanchet S, Chaouat G, Abdelkarim M, Truyens C and Capron F (2003) Demonstration of the presence of IL-16, IL-17 and IL-18 at the murine fetomaternal interface during murine pregnancy. Am J Reprod Immunol 49,101– 112. Racowsky C (2002) High rates of embryonic loss, yet high incidence of multiple births in human ART: is this paradoxical? Theriogenology 57,87– 96. Reznikov LL, Kim SH, Westcott JY, Frishman J, Fantuzzi G, Novick D, Rubinstein M and Dinarello CA (2000) IL-18 binding protein increases spontaneous and IL-1-induced prostaglandin production via inhibition of IFN-gamma. Proc Natl Acad Sci USA 97,2174–2179. Schoolcraft WB and Gardner DK (2001) Blastocyst versus day 2 or 3 transfer. Semin Reprod Med 19,259–268. Simon C, Moreno C, Remohi J and Pellicer A (1998) Molecular interactions between embryo and uterus in the adhesion phase of human implantation. Hum Reprod 13 (Suppl. 3),219–232; discussion 233-236. Simon C, Pellicer A and Polan ML (1995) Interleukin-1 system crosstalk between embryo and endometrium in implantation. Hum Reprod 10 (Suppl. 2),43– 54. Smart YC, Fraser IS, Roberts TK, Clancy RL and Cripps AW (1982) Fertilization and early pregnancy loss in healthy women attempting conception. Clin Reprod Fertil 1,177–184. Smeltz RB, Chen J, Hu-Li J and Shevach EM (2001) Regulation of interleukin (IL)-18 receptor alpha chain expression on CD4(þ) T cells during T helper (Th)1/Th2 differentiation. Critical downregulatory role of IL-4. J Exp Med 194,143–153. Tabibzadeh S, Kong QF, Babaknia A and May LT (1995) Progressive rise in the expression of interleukin-6 in human endometrium during menstrual cycle is initiated during the implantation window. Hum Reprod 10, 2793–2799. Toner JP (2002) Progress we can be proud of: U.S. trends in assisted reproduction over the first 20 years. Fertil Steril 78,943–950. Torigoe K, Ushio S, Okura T et al. (1997) Purification and characterization of the human interleukin-18 receptor. J Biol Chem 272,25737–25742. Veeck L (1990) The morphological assessment of human oocytes and early concepti. In Keel BAW (ed.) Handbook of laboratory diagnosis and treatment of infertility. CRC Press, Boca Raton, 353 pp. Wegmann TG, Lin H, Guilbert L and Mosmann TR (1993) Bidirectional cytokine interactions in the maternal-fetal relationship: is successful pregnancy a TH2 phenomenon? Immunol Today 14,353–356. Yoshino O, Osuga Y, Koga K, Tsutsumi O, Yano T, Fujii T, Kugu K, Momoeda M, Fujiwara T, Tomita K and Taketani Y (2001) Evidence for the expression of interleukin (IL)-18, IL-18 receptor and IL-18 binding protein in the human endometrium. Mol Hum Reprod 7,649–654. Submitted on March 10, 2003; accepted on May 14, 2004 1973