Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Behçet's disease wikipedia , lookup
Acute pancreatitis wikipedia , lookup
Atherosclerosis wikipedia , lookup
Ankylosing spondylitis wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Inflammation wikipedia , lookup
Neuromyelitis optica wikipedia , lookup
Inflammatory bowel disease wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Autoimmune encephalitis wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
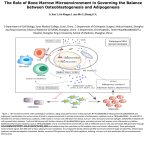
Journal of the American College of Cardiology © 2001 by the American College of Cardiology Published by Elsevier Science Inc. Vol. 38, No. 7, 2001 ISSN 0735-1097/01/$20.00 PII S0735-1097(01)01660-6 Increased Production of Inflammatory Cytokines in Patients With Silent Myocardial Ischemia Antonino Mazzone, MD,* Chiara Cusa, MD,* Iolanda Mazzucchelli, BSC,* Monia Vezzoli, MD,* Elena Ottini, MD,* Roberta Pacifici, BSC,† Piergiorgio Zuccaro, MD,† Colomba Falcone, MD‡ Milan, Rome and Pavia, Italy The aim of the study was to examine the inflammatory cytokines in patients with myocardial ischemia to evaluate whether silent ischemia patients exibit any particular cytokine pattern. BACKGROUND Silent myocardial ischemia is frequently observed in patients with coronary artery disease. Various endogenous mechanisms control a patient’s perceived intensity of pain. Among them, the inflammatory process and the related cytokine production are known to modulate the threshold for activating the primary afferent nociceptors. METHODS Seventy-eight patients with reproducible exercise-induced myocardial ischemia were studied: 34 symptomatic patients, with rest and/or stress angina; 44 asymptomatic patients, with no symptoms during daily life activities or during positive exercise stress test. Venous blood samples were taken from all patients to evaluate the expression of CD11b receptors both on neutrophils and monocytes. Frozen plasma samples (at ⫺80°C) were used to quantify the anti-inflammatory (interleukin-4 and -10, transforming growth factor-) and the proinflammatory cytokines (tumor necrosis factor-␣, interferon-␥, interleukin-1 and -6). RESULTS In asymptomatic patients lower CD11b receptor expression and higher concentration of anti-inflammatory cytokines were observed. Proinflammatory cytokine production was similar in the two groups. CONCLUSIONS The data suggest that an “anti-inflammatory pattern” of cytokine production correlates with silent ischemia and that the immune and inflammatory system activation may be crucial for angina symptoms. (J Am Coll Cardiol 2001;38:1895–901) © 2001 by the American College of Cardiology OBJECTIVES Immunocytes and cytokines are known to play a key role in the pathogenesis of the atherosclerotic process and coronary artery disease (CAD) (1,2). Silent myocardial ischemia frequently occurs at rest, during daily life activities or after physical or emotional exertion (3– 6); moreover, history of anginal pain might not be reported after acute myocardial infarction (MI) or during an angioplasty-induced coronary occlusion (7,8). The mechanisms responsible for silent ischemia are not well understood, and individual differences in pain threshold may only partially explain the variability in pain perception (3– 6). Patients with silent ischemia usually show a generalized hyposensitivity and higher pain threshold as compared with symptomatic patients (5– 8); production of the endogenous opiates may be partially responsible for decreased perception of pain (3). The relationship between inflammatory process and atherosclerosis has been extensively debated, but no data have yet been reported to describe the link between inflammatory system activation and silent myocardial ischemia. All stages of the atherosclerotic process are characterized by systemic endothelial dysfunction with subsequent endothelial damage and inflammation (1,2); these mechanisms are also involved in the atherosclerotic plaque instability and rupture (1,9 –12), which may occur in acute ischemic event. Several From the *Department of Internal Medicine, Legnano Hospital, Milan; †Clinical Biochemistry Department, National Institute of Health, Rome; and ‡Department of Cardiology, IRCCS S. Matteo Hospital, Pavia, Italy. This work was supported by grant 03/99 from IRCCS, S. Matteo Hospital, Pavia, Italy. Manuscript received March 20, 2001; revised manuscript received August 7, 2001, accepted August 27, 2001. other studies suggest that inflammatory cytokines may directly damage the endothelial surface, leading to ischemia, underlining the direct link between proinflammatory cytokine blood concentrations and cardiovascular risk (13–15). Cytokine production also correlates with clinical manifestations of acute coronary syndrome (14,15). Local vascular and perivascular inflammation occurs within the injured tissue. Immunocyte recruitment results from a multistep, sequential engagement of various adhesion molecules (1,9,11,16,17). The activated phagocytes (granulocytes and monocytes) express the CD11b/CD18 adhesion molecule, thus mediating their sticking adhesion to the endothelial cells and leading to phagocyte chemotaxis toward the inflamed tissue. In addition, the CD11b/CD18 binds to the activated complement factor (C3a), enhancing the inflammatory process, and recognizes fibrinogen-coated surfaces, leading to neutrophil-clot adhesion and fibrin digestion (11,17). Within the inflammatory site, the activated phagocytes release the cytokines interferon-gamma (IFN-␥), interleukin (IL)-4, IL-10 and transforming growth factor-beta (TGF-), which further enhance cellular migration; other proinflammatory cytokines such as IL-1, tumor necrosis factor (TNF)-␣ and IL-6 are known to be released within inflamed tissue (18 –20). Peripheral inflammation stimulates peripheral nerve endings causing hyperalgesia, which is due to enhanced localized inflammatory mediators (18,19); the local release of cytokines and endogenous opioids might be able to modulate the threshold for peripheral nerve-ending activation. Pain perception may result from microenviron- 1896 Mazzone et al. Silent Myocardial Ischemia and Inflammatory Cytokines Abbreviations CAD ⫽ CGRP ⫽ ECG ⫽ IFN-␥ ⫽ IL ⫽ MAb ⫽ MESF ⫽ MI ⫽ NF-B ⫽ PBR ⫽ SP ⫽ TGF- ⫽ TNF-␣ ⫽ and Acronyms coronary artery disease calcitonin gene-related peptide electrocardiogram or electrocardiographic interferon-gamma interleukin monoclonal antibodies molecules of equivalent soluble fluorescein myocardial infarction nuclear factor-B peripheral benzodiazepine receptor substance P transforming growth factor-beta tumor necrosis factor-alpha mental balances between proinflammatory (IL-1, TNF-␣, IL-6, and IFN-␥) and anti-inflammatory (IL-4, IL-10) cytokines (19,20). In our study we investigated inflammatory cytokines in patients with transient myocardial ischemia to determine whether silent ischemia correlates with any particular pattern of cytokine production. Inflammatory system activation markers were detected in patients with symptomatic angina and in patients with silent myocardial ischemia episodes. The CD11b adhesion molecule expression was detected on phagocytes, and proinflammatory (IL-1, TNF-␣, IL-6 and IFN-␥) and anti-inflammatory cytokine (IL-4, IL-10 and TGF-) production was quantified in ischemic patients. METHODS Patient selection. Seventy-eight male patients were studied: 34 patients with anginal pain during daily life activities (group P) and 44 patients with silent ischemia (group A). Two positive exercise stress tests documenting transient myocardial ischemia were performed in each patient. Patients who always refer anginal symptoms were enrolled in group P; patients who do not complain of anginal pain were enrolled in group A. Only male patients were studied. Patients with intercurrent inflammatory conditions, and patients who were on nonsteroidal anti-inflammatory drugs and steroids, were excluded. Pharmacologic washout was performed. Calcium channel antagonists and nitrates were halted 48 h before the test. Beta-blockers were gradually reduced and stopped 1 week before the examination. No patients were receiving digoxin. Informed written consent for all tests was obtained from the studied subjects. The Ethical Committee of our hospital approved the study. Exercise stress testing. All patients carried out a multistage bicycle ergometric stress test. The initial workload was 25 W and the subsequent stepwise increments were 25 W every 2 min at a pedalling frequency of 60 rpm. Standard 12-lead electrocardiogram (ECG) and blood pressure were recorded in basal conditions with the patient lying in a supine position for 10 min and subsequently just before the test, at the end of each stage, at the appearance of ECG JACC Vol. 38, No. 7, 2001 December 2001:1895–901 signs of ischemia and/or of anginal pain, at peak exercise and every 3 min during recovery. Three ECG leads (D3, V5, V6) were continuously monitored and displayed on an oscilloscope throughout the test. During the test the patients were repeatedly asked about the onset of angina or other symptoms. A positive ECG response was defined as the occurrence of at least 1-mm ST-segment depression, as compared with the baseline tracing. The ischemic threshold was defined as the appearance of a 1-mm flat or downsloping ST depression 0.08 s after the J point; the angina threshold was defined as the time of the first report of chest pain during the test. The multistage bicycle ergometric stress test was stopped when moderate-to-severe angina, dyspnea, muscle fatigue, ST-segment depression ⬎3 mm or major arrhythmia occurred. The rate-pressure product (heart rate ⫻ systolic blood pressure) was calculated in basal conditions, at the ischemic threshold and at peak exercise. Coronary arteriography. All patients underwent cardiac ventriculography and sones selective coronary arteriography within 7 ⫾ 5 days after the exercise stress test. Left ventriculography was performed before coronary arteriography in the 30° right anterior oblique projection; ventricular volumes and left ejection fraction were calculated by the standard area-length method. Significant CAD was defined as narrowing of 50% or more of the lumen of at least one of the three main arteries or their major branches. Flow cytometry analysis. Cell-surface receptors were detected by direct immunofluorescence signal evaluated by using flow cytometry (11,21). Blood samples were taken from forearm vein at 8:00 AM before exercise stress test. The samples were immediately processed in whole blood so as to avoid any in vitro manipulation that might activate phagocytes. The following monoclonal antibodies (MAbs) were tested: anti-CD11b/CD18; LFA-1 as anti-CD11a/CD18, and anti-mouse control FITC— obtained from Becton Dickinson (Milan, Italy). Analysis was performed by flow cytometry using fluorescence-activated cell sorter (Becton Dickinson). The fluorescence signal arising from the MAbs specifically bound to receptors was converted to molecules of equivalent soluble fluorescein (MESF) and quantified by using standardized fluorescein microbeads (quantum 26 FITC 7.3-m diameter hydrophobic microspheres, FACS, Research Triangle Park, North Carolina, obtained by Becton Dickinson, Milan, Italy). Cytokine assay. Quantitative measurement of IL-1, IL-4, IL-6, IL-10, TNF-␣ and IFN-␥ was performed using a solid-phase sandwich ELISA test with microtiter plate precoated with the specific MAb (Biosource, Celbio, Milan, Italy). Quantitative measurement of TGF-1 was performed using a solid-phase enzyme amplified sensitivity immunoassay with microtiter plate precoated with the specific MAb (Biosource; Celbio, Milan, Italy). Tests were performed according to the supplier’s instructions. Patient sample and cytokines standard samples were assayed simultaneously, in duplicate. The standard curve for the IL-1 assay ranged from 0.31 to 20 pg/ml; for IL-4 it was 0.39 to JACC Vol. 38, No. 7, 2001 December 2001:1895–901 Mazzone et al. Silent Myocardial Ischemia and Inflammatory Cytokines 1897 Table 1. Clinical, Angiographic and Ergometric Data in Symptomatic (Group P) and Asymptomatic Patients (Group A) With Coronary Artery Disease Clinical features Mean age (yrs ⫾ SD) Arterial hypertension Hyperlipidemia Diabetes mellitus Smoking Coronary angiography One-vessel disease Multivessel disease Ejection fraction (%) ⫾ SD LVEDV (ml) ⫾ SD LVEDP (mm Hg) ⫾ SD Exercise stress test Baseline RPP (beats/min ⫻ mm Hg) ⫾ SD Peak RPP (beats/min ⫻ mm Hg) ⫾ SD Peak ST depression (mm) ⫾ SD Group P (n ⴝ 34) Group A (n ⴝ 44) p Value 60.7 ⫾ 8.6 4 10 3 9 64.9 ⫾ 9.4 6 14 4 12 NS NS NS NS NS 10 14 58.1 ⫾ 10.2 115 ⫾ 26 16.4 ⫾ 8.1 7 26 60.1 ⫾ 9.4 124 ⫾ 21 14.6 ⫾ 3.9 NS NS NS NS NS 9.243 ⫾ 2.232 21.043 ⫾ 4.585 1.92 ⫾ 1.51 9.623 ⫾ 2.056 22.347 ⫾ 6.573 2.24 ⫾ 1.82 NS NS NS LVEDV ⫽ left ventricular end-diastolic volume; LVEDP ⫽ left ventricular end-diastolic pressure; RPP ⫽ rate-pressure product. 12.5 pg/ml; for IL-6 it was 0.16 to 5.0 pg/ml; for IL-10 it was 0.78 to 25 pg/ml; for TNF-␣ it was 0.5 to 16 pg/ml; for IFN-␥ it was 15.6 to 500 pg/ml, and for TGF-1 it was 16 to 2,000 pg/ml. The sensitivity of assays were: 0.19 pg/ml for IL-1; 0.27 pg/ml for IL-4; 0.10 pg/ml for IL-6; 0.21 pg/ml for IL-10; 0.1 pg/ml for TNF-␣; 4 pg/ml for IFN-␥; and 2 pg/ml for TGF-1. Plasma samples were appropriately diluted with a phosphate-buffered solution to enter calibration curve ranges. Assay performance was tested using two concentrations of cytokines in plasma throughout the procedure. Mean intra- and interassay coefficients of variation were always ⬍6%. Statistical analysis. Results are expressed as mean ⫾ SD. The Mann-Whitney nonparametric analysis was used to investigate differences between the two different groups. The StatView program for Apple Computers was utilized, and p values ⬍0.05 were considered statistically significant. RESULTS Seventy-eight patients (mean age 62.5 ⫾ 8.6 years) were included in the study. Group P consisted of 34 anginal patients: 19 patients with effort angina, 4 patients with angina at rest and 11 patients with mixed angina. Silent ischemia was documented during exercise stress test in 44 patients (group A); 27 patients with silent ischemic episodes during daily life activities and documented by Holter recording were also included within group A. Clinical data are reported in Table 1. There were no statistically significant differences in age, ECG-documented severity of angina, hypertension, hyperlipidemia, diabetes and smoking. Coronary angiography results were similar within the two groups. All patients in group P complained of angina during exercise test; moderate to severe dyspnea was experienced during exercise stress test in group A patients. The entity of ST-segment depression at peak exercise was similar in the two groups. No difference was found in the CD11a/CD18 expression on monocytes. The CD11b/CD18 expression was lower in asymptomatic patients both on granulocytes and monocytes (p ⬍ 0.01) (Fig. 1). In symptomatic patients, MESF values (⫻ 103/cells) were 68.1 ⫾ 7 for granulocytes and 80.8 ⫾ 6 for monocytes; in asymptomatic patients, MESF values (⫻ 103/cells) were 56.4 ⫾ 7 for granulocytes and 48.4 ⫾ 8 for monocytes. In asymptomatic patients, anti-inflammatory cytokine levels were significantly higher: IL-4, 0.634 ⫾ 0.062 ng/ml vs. 1.790 ⫾ 0.195 ng/ml, p ⬍ 0.005; IL-10, 5.804 ⫾ 0.364 ng/ml vs. 15.350 ⫾ 1.129 ng/ml, p ⬍ 0.001; TGF-, 2.511 ⫾ 0.232 ng/ml vs. 9.671 ⫾ 0.533 ng/ml, p ⬍ 0.001 (Fig. 2A). Proinflammatory cytokine concentrations were similar in the two groups: IL-1, 0.376 ⫾ 0.027 ng/ml vs. 0.412 ⫾ 0.025 ng/ml, p ⫽ NS; IL-6, 2.581 ⫾ 0.534 ng/ml vs. 2.805 ⫾ 0.426 ng/ml, p ⫽ NS; TNF-␣, 5.746 ⫾ 0.401 ng/ml vs. 5.733 ⫾ 0.322 ng/ml, p ⫽ NS; IFN-␥, 26.362 ⫾ 2.193 pg/ml vs. 24.860 ⫾ 3.406 pg/ml, p ⫽ NS (Fig. 2B). DISCUSSION Our data show that, patients with asymptomatic ischemia, there is higher production of anti-inflammatory cytokines with lower expression of CD11b/CD18 adhesion molecule on phagocytes. These observations may indicate that the clinical feature of silent myocardial ischemia might correlate with a particular biochemical pattern of inflammatory system activation. Inflammation opioid system and peripheral benzodiazepine receptors. Inflammation is involved in the pathogenesis of atherosclerotic process, in plaque instability and rupture and in tissue injury during MI. In this regard, several studies showed that unstable and complicated atherosclerotic plaque might result from recruitment of neutrophils and monocytes within the plaque owing to local 1898 Mazzone et al. Silent Myocardial Ischemia and Inflammatory Cytokines JACC Vol. 38, No. 7, 2001 December 2001:1895–901 Figure 1. CD11b/CD18 adhesion molecule expression in asymptomatic patients (group A) and in patients complaining of angina pain (group P). Asymptomatic patients express lower level of adhesion molecule both on neutrophils and on monocytes. Open bars ⫽ silent ischemia; solid bars ⫽ symptomatic ischemia. MESF ⫽ molecules of equivalent soluble fluorescein. production of inflammatory metabolites and cytokines (9 – 12). The local inflammatory reaction further mediates tissue damage and may be responsible for the modulation of the pain transmission pathways (1,2,10,13,15). Immunocytes locally release inflammatory cytokines as well as betaendorphins, thus interfering with the endogenous opioidmediating system (3,4,8,20,21–27). The resulting inflammatory microenvironmental production may alter the threshold for activation of peripheral nerve endings (1,2,10,13,15). Higher threshold of pain transmission pathway activation has been demonstrated during strenuous exercise and after physical training due to increased plasma levels of endogenous opioids (see beta-endorphins), as part of physiological stress response (4,8). During myocardial ischemia, the endogenous opioids, which derive from local immune cells, interact with specific receptors on sensory nerves, leading to strong and clinically measurable analgesia (5,21,22,24 –27). It has also to be stressed that morphine, which is the best pain-relieving drug currently available for cardiac patients, is able to decrease leukocyte activation and to exert anti-inflammatory properties (3,22,24 –29). In this regard, our previous studies showed that morphine and other opioid peptides downregulate the expression of CD11b/CD18 receptor on phagocytes, decreasing phagocyte– endothelial cell interactions (23). We would also like to focus briefly on peripheral benzodiazepine receptors (PBRs), which are expressed on leukocyte surfaces. Higher PBR expression correlates with higher threshold for pain transmission pathway activation and with acute systemic stress response. Moreover, in a dose-related manner, PBR interferes with inflammatory response and cytokine release (30,31) and may modulate the perception of pain (32). Our previous work showed that PBRs are strongly expressed on the leukocytes of patients with silent myocardial ischemia (21). Inflammatory cytokines and pain. The T-lymphocyte and monocyte infiltrates within atherosclerotic lesions may be responsible for plaque instability and acute coronary events (1,13,33–35). The T-lymphocyte responses can be categorized as proinflammatory (Th1 type) or anti-inflammatory (Th2 type) (34,35). The Th1 type activation leads to proinflammatory cytokine release (TNF-␣, IL-1, IL-6, and IL-8), whereas Th2 lymphocyte activation leads to endorphin and anti-inflammatory cytokine (IL-4 and IL10) release. The proinflammatory pattern activation seems to intensify nociception, whereas Th2 lymphocyte production (36) seems to reduce the pain perception. Several observations suggest that inflammatory cytokines orchestrate nociception and also suggest the role of proinflammatory and anti-inflammatory cytokines in the perception of pain. Particularly, proinflammatory cytokines are known to induce the release of pain mediators, such as bradykinin and calcitonin gene-related peptide (CGRP) and to activate vagal afferents (37). The IL-1 is a proinflammatory cytokine able to induce hyperalgesia. Central administration of IL-1 enhances the nociceptive neuronal response (38 – 40) and, in monoarthritic rat, dosedependently enhances the spinal-cord– evoked release of substance P (SP) and CGRP (41). By contrast, the IL-1 receptor antagonist attenuated the IL-1–induced hyperal- JACC Vol. 38, No. 7, 2001 December 2001:1895–901 Figure 2. Cytokine plasma levels in asymptomatic patients (group A) and in patients complaining of angina (group P); A, anti-inflammatory cytokines; B, proinflammatory cytokines. Open bars ⫽ silent ischemia; solid bars ⫽ symptomatic ischemia. IFN-␥ ⫽ interferon-gamma; IL ⫽ interleukin; TGFbeta ⫽ transforming growth factor-beta; TNF-alpha ⫽ tumor necrosis factor-alpha. gesia (40,42). The TNF-␣ induces pain and hyperalgesia after injection; the effects are mediated by direct sensitization of primary afferent nociceptors and by upregulation of other proinflammatory proteins. Both subcutaneous (43) and intraplantar (44) TNF-␣ injections contribute to hyperalgesia and inflammation; this evokes ongoing activity in type C nociceptors, causes significant and dose-related increases in skin vascular permeability (43), induces proinflammatory cytokine production (IL-1, IL-6, IL-8), and triggers the cyclooxygenase-dependent pathways to synthesize prostaglandins (43). In experimental inflammation, pentoxifylline was demonstrated to inhibit TNF-␣ release, with consequent decrease of pain-related behavior (44). By contrast, anti-inflammatory cytokine IL-10 administration was demonstrated to reverse the dynorphin-induced allodynia, which is a model of neuropathic pain in the mouse, thus suggesting that allodynia might be modulated by the inflammatory cytokine system (45). The IL-10 inhibits the positive inflammatory feed-forward loop by Mazzone et al. Silent Myocardial Ischemia and Inflammatory Cytokines 1899 inhibiting the initial induction and the subsequent amplification of proinflammatory cytokines (46). A single peripheral administration of IL-10 was demonstrated to decrease the nerve injury-induced thermal hyperalgesia (46,47) and the intradermal endotoxin-induced hyperalgesia (48). Our data show that IL-10 levels increase significantly in asymptomatic patients. Transforming growth factor- stimulates connective tissue growth and collagen formation, and it can virtually and strongly inhibit all the immune and hematopoietic functions, especially if present before cell activation (49,50). It also has a role in mediating inflammation and cytotoxic reactions (49 –51): TGF- blocks the IFN-␥– induced cell activation, thus increasing the production of ROS, prostaglandins and nitric oxide; IL-4 has similar effects to that of TGF- in limiting the inflammatory hyperalgesia (51,52). Role of the transcription factor nuclear factor-B. Cytokine production is primarily regulated at the transcriptional level (53,54) by specific transcriptional factors linking the receptor-driven cytoplasmic signaling events with changes in gene expression. The nuclear factor-B (NF-B) activation induces nociceptive protein production such as proinflammatory cytokines, inducible nitric oxide synthase (S), cyclo-oxygenase (COX-2) and pre-prodynorphin. Several stimuli, such as proinflammatory cytokines, oxidative stress, nerve growth factor, and protein kinase C, can activate NF-B (53–56). The relevance of NF-B to nociception is supported by the observation that hyperalgesic doses of nerve growth factor in vivo activate NF-B in dorsal root ganglia (56). Moreover, capsaicin-induced hyperalgesia associates with enhanced expression of NF-B (56). Anti-inflammatory cytokine administration (such as IL-10) correlates with NF-B reduced activity and with decreased intensity of pain perception (47). Our data may suggest that alterations of anti-inflammatory cytokine production might exert an inhibitory effect on NF-B, which is crucial for nociception, leading to an ischemic angina episode. Study limitations. Our results showed that an antiinflammatory pattern of cytokine production is activated in patients with silent myocardial ischemia. The data suggest that silent ischemia might result from a particular microenvironmental pattern of inflammatory system activation leading to higher threshold for the stimulation of peripheral nerve endings. The findings should be interpreted cautiously. Cytokines have a very short half-life in the bloodstream, and their biologic effects seem to be more related to the length of cytokine exposure than to their absolute circulating concentrations; in addition, cytokine levels were detected only once in the study, and our observational study did not include any follow-up controls. Sequential measurement of circulating cytokines and clinical correlation with patients’ symptoms and illness stages are necessary to further confirm our data. Moreover, we lack a biologic model describing stimuli able to cause Th1 or Th2 activation in cardiovascular patients, and we did not investigate whether 1900 Mazzone et al. Silent Myocardial Ischemia and Inflammatory Cytokines a particular pattern of cytokines might correlate with clinical outcome. In addition, we also cannot exclude the idea that inflammatory cell activation and cytokine release are epiphenomena occurring during myocardial ischemia, without any pathogenetic implication with the basic illness. Moreover, pain perception might only depend on individual pain threshold and/or other unknown mechanisms. Nevertheless, the positive association described between silent myocardial ischemia and anti-inflammatory cytokine production cannot be excluded. Conclusions. The significant increase of levels of antiinflammatory cytokines together with the decrease of leukocyte adhesion molecule expression might identify one of the mechanisms for silent ischemia. In patients with silent ischemia it might be possible that the Th2 activation will induce higher production of anti-inflammatory cytokines together with endogenous opioid production and higher expression of PBRs. The anti-inflammatory cytokines might be able to block the pain transmission pathway activation by increasing the threshold for nerve activation. In addition, the anti-inflammatory cytokines will exert a prolonged inhibitory effect on transcription factor NF-B, leading to reduction and/or elimination of pain-mediating substances. Further studies are needed to explain the effects of these cytokines on clinical progression and prognosis and on the atherosclerotic process. These findings might also indicate that immune system cytokine production can modulate nociception, thus providing us with data on widespread clinical implications. Acknowledgment We thank Elizabeth De Jung for the final English language version of this article. JACC Vol. 38, No. 7, 2001 December 2001:1895–901 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. Reprint requests and correspondence: Dr. Antonino Mazzone, Chief of Internal Medicine and Oncology, Hospital of Legnano, Via Candiani 2, 20025 Legnano, Milano, Italy. E-mail: medicina 2legnano@ao-legnano. REFERENCES 1. Ross R. Mechanisms of disease: atherosclerosis and inflammatory disease. N Engl J Med 1999;340:115–26. 2. Shah PK. New insights into the pathogenesis and prevention of acute coronary syndromes. Am J Cardiol 1997;79:17–23. 3. Drost C. Influence of opiate system in pain transmission during angina pectoris. Z Kardiol 1990;79S:31–3. 4. Falcone C, Specchia G, Rondanelli R, et al. Correlation between beta-endorphin plasma levels and anginal symptoms in patients with coronary artery disease. J Am Coll Cardiol 1998;11:719 –23. 5. Meller ST, Gebhart GF. Silent ischemia: a hypothetical mechanism. Neurosci Biobehav Rev 1993;17:229 –36. 6. Falcone C, Sconocchia R, Guasti L, et al. Dental pain threshold and angina pectoris in patients with coronary artery disease. J Am Coll Cardiol 1998;12:348 –52. 7. Glazier JJ, Chierchia S, Brown MJ, et al. The importance of generalized defective perception of painful stimuli as a cause of silent myocardial ischemia in chronic stable angina pectoris. Am J Cardiol 1986;58:667–72. 8. Falcone C, Guasti L, Ochan M, et al. Beta-endorphins during 26. 27. 28. 29. 30. 31. 32. 33. 34. coronary angioplasty in patients with silent or symptomatic myocardial ischemia. J Am Coll Cardiol 1993;22:1614 –20. Mazzone A, De Servi S, Ricevuti G, et al. Increased expression of neutrophil and monocyte adhesion molecules in unstable coronary artery disease. Circulation 1993;88:358 – 63. De Servi S, Mazzone A, Ricevuti G, et al. Clinical and angiographic correlates of leukocyte activation in unstable angina. J Am Coll Cardiol 1995;26:1146 –50. Mazzone A, De Servi S, Mazzucchelli I, et al. Increased expression of CD11b/CD18 on phagocytes in ischaemic disease: a bridge between inflammation and coagulation. Eur J Clin Invest 1997;27:648 –52. Folcik VA, Aamir R, Cathcart MK, et al. Cytokine modulation of LDL oxidation by activated human monocytes. Arterioscler Thromb Vasc Biol 1997;17:1954 – 61. Sinisalo J, Paronen J, Mattila KJ, et al. Relation of inflammation to vascular function in patients with coronary heart disease. Atherosclerosis 2000;149:403–11. Ridker PM, Rifai N, Stampfer MJ, et al. Plasma concentration of IL6 and the risk of future myocardial infarction among apparently healthy men. Circulation 2000;101:1767–72. Prediman K, Shah PK. Circulating markers of inflammation for vascular risk prediction. Circulation 2000;101:1758–9. Teplyakov AI, Pryshepova EV, Kruchinsky NG, et al. Cytokine and soluble adesion molecules. Possible manifestation of atherosclerotic response in atherosclerosis. Ann N Y Acad Sci 2000;902:320 –2. Mazzone A, Ricevuti G. Leukocyte CD11/CD18 integrins: biological and clinical relevance. Haematologica 1995;80:161–75. Woolf CJ, Allchorne A, Safieh-Garabedian B, et al. Cytokines, nerve growth factor and inflammatory hyperalgesia: the contribution of tumor necrosis factor-alpha. Br J Pharmacol 1997;121:417–24. Watkins LR, Wiertelak BP, Goehier LB, et al. Characterization of cytokine-induced hyperalgesia. Brain Res 1994;654:15–26. Porreca F, Lai J, Malan TP. Can inflammation relieve pain? Nat Med 1998;4:1359 – 60. Mazzone A, Mazzucchelli I, Vezzoli M, et al. Increased expression of peripheral benzodiazepine receptors on leukocytes in silent myocardial ischemia. J Am Coll Cardiol 2000;36:746 –50. Mazzone A, Ricevuti G, Pasotti D, et al. Peptide opioids and morphine effects on inflammatory process. Inflammation 1990;14: 717–26. Mazzone A, Ricevuti G. Interaction between morphine and granulocyte aggregation in myocardial ischemia. Cardiovasc Drugs Ther 1990;4:303– 4. Stefano GB, Scharrer B, Smith EM, et al. Opioid and opiate immunoregulatory processes. Clin Rev Immunol 1996;16:109 – 44. Stein C. Mechanism of disease. The control of pain in peripheral tissue by opioids. N Engl J Med 1995;332:1685–90. Stefano GB, Salzet B, Fricchione GL, et al. Enkelytin and opioid peptide association in invertebrates and vertebrates: immune activation and pain. Immunol Today 1998;19:265– 8. Machelsa H, Stein C. Pain control by immune-derived opioids. Clin Exp Pharmacol Physiol 2000;27:533– 6. Roy S, Charboneau RG, Barke RA. Morphine synergizes with lipopolysaccharide in a chronic endotoxemia model. J Neuroimmunol 1999;95:107–14. Rattan AK, Tejwani GA. Sodium ions modulate differentially the effect of a benzodiazepine agonist on rat spinal , ␦ and opioid receptors. Pharmacology 1994;48:30 – 40. Torres SRR, Nardi GM, Ferrara P, et al. Potential role of peripheral benzodiazepine receptors in inflammatory responses. Eur J Pharmacol 1999;385:R1–2. Taupin V, Gogusev J, Descamps-Latscha B, et al. Modulation of tumor necrosis factor-␣, interleukin-1, interleukin-6, interleukin-8, and granulocyte/macrophage colony-stimulating factor expression in human monocytes by an endogenous anxiogenic benzodiazepine ligand, triakontatetraneuropeptide: evidence for a role of prostaglandins. Mol Pharmacol 1993;43:64 –9. Gavish M, Bachman I, Shoukrun R, et al. Enigma of peripheral benzodiazepine receptor. Pharmacol Rev 1999;51:629 –50. Biasucci LM, Liuzzo G, Angiolillo DJ, et al. Inflammation and acute coronary syndrome. Herz 2000;25:108 –12. Liuzzo G, Goronzi JJ, Yang H, Hopecky SL, et al. Monoclonal T-cell activation and plaque instability in acute coronary syndromes. Circulation 2000;101:2883– 8. JACC Vol. 38, No. 7, 2001 December 2001:1895–901 Mazzone et al. Silent Myocardial Ischemia and Inflammatory Cytokines 35. Mazzone A, De Servi S, Vezzoli M, et al. Plasma level of interleukin-2, 6, 10 and phenotypic characterization of circulating T lymphocytes in ischemic heart disease. Atherosclerosis 1999;15:369 – 74. 36. Panerai AE, Sacerdote P. Beta-endorphin in the immune system: a role at last? Immunol Today 1997;18:317–9. 37. Opree A, Kress M. Involvement of the inflammatory cytokines TNF-␣ IL-1-beta and IL-6 but not IL-8 in the developement of heat hyperalgesia: effects of heat-evoked CGRP release from rat skin. J Neurosci 2000;20:6289 –93. 38. Oka T, Aou S, Hori H. Intracerebrovascular injection of interleukin1-beta enhances nociceptive neuronal responses of the trigeminal nucleus caudalis in rats. Brain Res 1994;656:236 – 44. 39. Yabuchi K, Nishiyori AM, Satoh M, et al. Biphasic effects of intracerebroventricular IL-1-beta on mechanical nociception in the rat. Eur J Pharmacol 1996;300:59 – 65. 40. Oka T, Aou S, Hori T. Intracerebrovascular injection of IL-1-beta induces hyperalgesia in rats: Brain Res 1993;624:61– 8. 41. Malcangio M, Bowery NG. Spinal cord SP release and hyperalgesia in monoarthritic rats: involvement of the GABA-B receptors system Br J Pharmacol 1994;113:1561– 6. 42. Cunha JM, Cunha FQ, Poole S, et al. Cytokine-mediated inflammatory hyperalgesia limited by IL 1 receptor antagonist. Br J Pharmacol 2000;130:1418 –24. 43. Junger H, Sorkin LS. Nociceptive and inflammatory effects of subcutaneous TNF-␣. Pain 2000;85:145–51. 44. Wordliczeck J, Szczepanik AM, Banach M, et al. The effect of pentoxifiline on post-injury hyperalgesia in rats and postoperative pain in patients. Life Sci 2000;66:1155– 64. 45. Laughlin TM, Bethea JR, Yezierski RP, et al. Cytokine involvement in dynorphin-induced allodynia. Pain 2000;84:159 – 67. 46. Wagner R, Janjigian M, Myers RR. Anti-inflammatory interleukin-10 therapy in CCI neuropathy decreases thermal hyperalgesia, macrophage recruitment, and endoneural TNF-alpha expression. Pain 1998; 74:35– 42. 47. Poole S, Cunha FQ, Selkirk S, et al. Cytokine-mediated inflammatory hyperalgesia limited by interleukin-10. Br J Pharmacol 1995;115: 684 – 8. 48. Kanaan SA, Poole S, Saade NE, et al. IL-10 reduces the endotoxininduced hyperalgesia in mice. J Neuroimmunol 1988;86:142–50. 49. Fontana A, Constam DB, Frei K, et al. Modulation of the immune response by TGF-beta. Int Arch Allergy Immunol 1992;99:1–7. 50. Clark DA, Coker R. Transforming growth factor-beta (TGF-beta). Int J Biochem Cell Biol 1998;30:293– 8. 51. Letterio JJ Roberts AB. Regulation of the immune responses by TGF-beta. Annu Rev Immunol 1998;16:137– 61. 52. Cunha FQ, Poole S, Lorenzetti BB, et al. Cytokine-mediated inflammatory hyperalgesia limited by IL4. Br J Pharmacol 1999;126:45–50. 53. O’Neill LA, Kaltschmidt C. NF-kappa B: a crucial transcription factor for glial and neuronal cell function. Trends Neurosci 1997;20:252– 8. 54. Baeurle PA, Henkel T. Function and activation of NF-kappa B in the immune system. Annu Rev Immunol 1994;12:141–79. 55. Welters ID, Fimiani C, Bilfinger TV, et al. NF-B, nitric oxide and opiate signaling. Med Hypotheses 2000;54:263– 8. 56. Wood JN. Regulation of NF-kappa B activity in rat dorsal root ganglia and PC12 cells by tumor necrosis factor and nerve growth factor. Neurosci Lett 1995;192:41– 4. 1901