Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
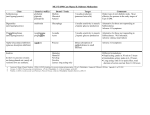
• • Diabetes mellitus: a chronic disease associated with abnormally high levels of the sugar glucose in the blood. • Diabetes is caused by one of two mechanisms: • • 1. Inadequate production of insulin • • 2. Inadequate sensitivity of cells to the action of insulin. Hyperglycemia is an abnormally high blood glucose (blood sugar) level. Hyperglycemia is a hallmark sign of diabetes (both type 1 diabetes and type 2 diabetes) and prediabetes. Diabetes is the most common cause of hyperglycemia. Symptoms and Signs • • • • • • • • • • ◾Polyuria ◾Polyipsia ◾Polyphagia ◾Weight loss ◾Muscle weakness ◾Always tired ◾Poor healing ◾Vaginal infection ◾Sexual problems ◾Sensory changes Complication of Diabetes • ◾Retinopathy • ◾Neuropathy • ◾Nephropathy • ◾Cardiovascular disease • ◾Amputations • ◾Other complication How to Control diabetes • • • • • • • • • • • ◾Change lifestyle. ◾Eating healthier. ◾Exercise (physical activity). ◾Taking care of your body. ◾Taking care of your teeth . ◾taking oral antidiabetic agents. ◾No smoking. ◾ Control blood pressure. ◾Check blood sugar levels daily. ◾Check feet to make sure there is no nerve damage . ◾Check in with you're doctor at least once a month . Diabetes and Dental problems • • People with uncontrolled diabetes are at greater risk for dental problems. They're more likely to have infections of their gums and the bones that hold their teeth in place, because diabetes can reduce the blood supply to the gums. High blood sugar may also cause dry mouth and make gum disease. • Note : • the patients with diabetes are higher risk for gum problems . Complications of Diabetes in Oral cavity • ◾Tooth decay • ◾ Periodontal disease • ◾Bleeding gums • ◾Tooth sensitivity • ◾Recession of gums • ◾Bad breath • ◾Salivary gland dysfunction Medical Management of DM Treatment of Type 2 Diabetes •Monotherapy with oral agent •Combination therapy with oral agents •Insulin +/- oral agent •insulin required in 20-30% of patients With duration of the disease, more intensive therapy is required to maintain glycemic goals MAJOR TARGETED SITES OF DRUG CLASSES Pancreas Beta-cell dysfunction Sulfonylureas Liver Hepatic glucose overproduction Biguanides •Thiazolidinediones •DPP-4 inhibitors •GLP1 analogue •Insulin Meglitinides Muscle & fat DPP-4 inhibitor ↓Glucose level Gut Insulin resistance Thiazolidinediones Biguanides Reduced glucose absorption α-glucosidase inhibitors Insulin Oral Hypoglycemics • Drugs That Increase Insulin Supply: • Sulfanylureas - enhance secretion of insulin from pancreas (requires functional β cells) • First Generation: • • • • Tolbutamide (Orinase) Acetohexamide (Dymelor) Tolazamide (Tolinase) Chlorpropamide (Diabenase) • Second Generation: • Glimipride (Amaryl) • Glyburide (DiaBeta; Micronase) • Glipizide (Glucotrol) • Other Secretagogues • Nateglinide (Starlix) • Repaglinide (Prandin) 25 Mechanism of Insulin Release in the Pancreas Oral Hypoglycemics • Drugs That Decrease Insulin Resistance or Improve Insulin Effectiveness: • Biguanides - decrease glucose secretion by liver and enhance the uptake of glucose in cells • Metformin (Glucophage) • Alpha-Glucosidase Inhibitors - slows uptake of CHO from gut • Acarbose (Precose) • Miglitol (Glyset) • Thiazolidinediones - increases cellular responsiveness to insulin • Pioglitazone (Actos) • Rosiglitazone (Avandia) 27 Mechanism of Insulin Action • Insulin binds to specific high affinity membrane receptors with tyrosine kinase activity • Phosphorylation cascade results in translocation of Glut-4 (and some Glut-1) transport proteins into the plasma membrane. • It induces the transcription of several genes resulting in increased glucose catabolism and inhibits the transcription of genes involved in gluconeogenesis. • Insulin promotes the uptake of K+into cells. Insulin Sensitizers Thiazolidinediones (Glitazones) • These agents are insulin sensitizers, they do not promote insulin secretion from β-cells but insulin is necessary for them to be effective. Pioglitazone and rosigglitazone are the two agents of this group. Oral Drug Therapy for Type 2 DM • Sulfonylureas • Repaglinide Nateglinide • Biguanides • Thiazolidinediones • Acarbose Miglitol } } } Insulin secretagogues Insulin sensitizers Inhibitors of CHO absorption Sulfonylureas: Mechanism of Action •Improved insulin sensitivity from improved glucose control •Chronic treatment with sulfonylureas improved FPG and OGT •These agents stimulate insulin release from the pancreatic islets. •Normalization of glycemia results in increased sensitivity to insulin •Improved glucose control results in increased ß cell responsiveness Sulfonylureas: • Tolbutamide: • Has shorter duration of action. • More safe. Second Generation Sulfonylureas • Glyburide • Oxidized to weakly active metabolites • Half-life - 6 hours • Duration of action24 hours • Potency - High (1.25 to 20 mg/d) Sulfonylureas: Metabolism & Excretion Metabolized in the liver Hepatic dysfunction will alter pharmacokinetics Excretion Second generation: significant fecal excretion Glyburide -50% Glimeperide - 40% Clinical Uses of Sulfonylureas Hypoglycemic agents for treatment of Type 2 diabetes mellitus Act by increasing endogenous insulin secretion \ not indicated for Type 1 Most effective when ß cell function has not been severely compromised Increased insulin secretion favors lipogenesis Most appropriate in non- or mildly obese Up to 160 % of ideal body weight Adverse Effects of Sulfonylureas • Severe hypoglycemia • Overdose • Early in treatment • Most common with glyburide • Weight gain • Erythema, skin reactions • Blood dyscrasias (abnormal cellular elements) • Hepatic dysfunction and other GI disturbances Contraindications for Sulfonylureas Pregnancy Surgery Severe infections Severe stress or trauma Severe hepatic or renal failure Insulin therapy should be used in all of these Biguanides Galega officinalis French lilac Goatsrue Active ingredient: NH guanidine H2N NH2 Biguanides First Generation- Phenformin Phenethylbiguanide Adverse Effects Lactic acidosis Risk of cardiovascular disorder Biguanides • Second Generation- Metformin 1,1-Dimethylbiguanide CH2H2C N H Rarely produces lactic acidosis except under predisposing conditions NH2 NH2 C C N H NH2 Biguanides Mechanism of action: • antihyperglycemic • Correct elevated hepatic glucose output Inhibit gluconeogenesis Inhibit glucose-6-phosphatase activity glycogen sparing • insulin resistance • Mediated by activation of 5’AMP-activated protein kinase (AMPK) in hepatocytes and muscle • Do not increase insulin secretion • Not hypoglycemic, even at high doses Second Generation Biguanides • Do not produce hypoglycemia • Secondary beneficial effects on lipids • • • • Reduced triglycerides Reduced total cholesterol Reduced LDL Increased HDL Second Generation Biguanides • Insulin levels unchanged or reduced • Weight loss, some reduction of blood pressure • Appropriate for obese Type 2 diabetics Metformin • Excreted unchanged in the urine • Half-life - approximately 2 hours • Does not bind to plasma proteins Metformin • Should not be used with renal or hepatic dysfunction • Also approved for prevention of Type 2 diabetes in high risk individuals • Use also for polycystic ovary syndrome: insulin resistance with ovarian hyperandrogenism a glucosidase inhibitors CH2OH Acarbose •Mechanism of action: OH H3C •: competitive and O reversible inhibitors of HN a glucosidase in the small CH2intestine OH OH O and •Delay carbohydrateO digestion HO CH2OH absorption OH O O OH •Smaller HO OHrise in postprandial glucose HO HO OH HO N OH Miglitol HO HO a glucosidase inhibitors Clinical use For mild to moderate fasting hyperglycemia with significant postprandial hyperglycemia Taken with the first bite of a meal Do not produce hypoglycemia, lactic acidosis, or significant weight gain Effective regardless of age, genetic factors, body weight, duration or severity of disease Dental Management • Important to get a complete health history • Ask the undiagnosed diabetic about signs and symptoms, family history, and determine if they are at risk • Ask the known diabetic about their glucose levels, how they control their glucose, their last doctor’s visit, and if they are displaying any symptoms of diabetes now Oral signs and symptoms • Xerostomia, increased caries • Dry atrophic cracked oral mucosa, angular chellitis • Mucositis, ulcers, and desquamative gingivitis, burning mouth syndrome • Difficulty swallowing • Opportunistic bacteria, fungal, viral infection Oral Signs and Symptoms • Poor Wound Healing • Periodontal Disease-usually in poorly controlled or undiagnosed diabetics • Incidence of Perio Disease increases among patients with diabetes as they age • Diabetics with advanced systemic conditions have periodontal disease more frequently and severe. Diagnosing the Diabetic • Symptoms of Diabetes and non-fasting plasma glucose concentration is 200mg/ml or greater • Fasting glucose is 126mg/dl • Lowered oral glucose tolerance test (after 75g glucose load) blood glucose is 200mg/dl or greater Diagnosing the Diabetic • Glycosylated Hemoglobin Hb1Ac • Glycohemoglobin increases in presence of hyperglycemia • Levels help monitor progress of disease and level of patient control • Reflects glucose levels in blood over 6-8 weeks preceding the test