Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
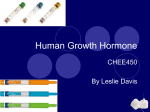
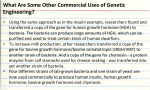
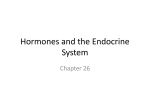
Review Article Ann Clin Biochem 1990; 27: 542-550 Prolactin and growth hormone: molecular heterogeneity and measurement in serum Caroline R Smith * and M R Norman From the Department of Clinical Biochemistry, King's College School of Medicine, Denmark Hil/, London SE5, UK SUMMARY. The pituitary hormones prolactin and growth hormone are related single-chain polypeptides. Both hormones exist in the circulation in several molecular forms, and this heterogeneity may account for some of the complex and sometimes contradictory actions, in vivo and in vitro, of both hormones. It may also lead to problems with quantitation by immunoassays and discrepancies between the results given by assays using different antibodies. Modified forms of the hormones may have markedly different activity in bioassays from that of the parent hormone, but the clinical significance of this is unclear. In this review we summarize what is known about the molecular heterogeneity of the hormones and briefly discuss the implications for clinical biochemists. Additional key phrases: somatotropin; somatomammotropin Over the last 10 years there have been major developments in understanding the relationship between the structure and function of the pituitary peptide hormones. The glycoprotein hormones follitropin (FSH) and lutropin (LH), for example, are now known to exist in the circulation in a number of different forms depending on the composition of their carbohydrate units."? Activity in immunoassays may be determined primarily by the peptide chain and thus be unrepresentative of the biological activity of the hormone, which is modified by the carbohydrate group.Y TABLE 1. The importance of molecular heterogeneity in the physiology of human prolactin (hPRL) and human growth hormone (hGH) has only recently been appreciated. Major sources of molecular heterogeneity of both hormones are summarized in Tables 1 and 2. mE JipRL AND hGH GENE FAMILY The hGH and hPRL are believed to have evolved as a result of duplications of a common ancestral gene. Studies of other animal growth hormones have shown, however, that hGH differs consider- Major forms of hGH in serum Approx. MW Variant (kD) Gene/Chromosome Comments Monomeric pituitary hGH hGH 20kD 'Big' hGH 'Big-big' hGH 22 20 40-50 >60 hGH-N/17 hGH-N/l7 hGH-N/l7 hGH-N/17 Fragments <20 hGH-N/17 Placental hGH 22 24,26 hGH-V/17 hGH-V/17 Approx. 75% of total immunoactive hGH Approx. 16% total immunoactive hGH Dimers (a) Aggregates (b) hGH binding-protein complex Present in serum in basal state ?Formed in tissues Secreted by placenta Glycosylated forms of placental hGH ·Present address: Department of Rheumatology, The Whittington Hospital, Highgate Hill, London N19, UK. Correspondence: Dr M R Norman. 542 Prolactin and growth hormone TABLE 2. 543 Major forms of hPRL in serum Approx. MW Variant (kD) Gene/Chromosome Comments Main component of hPRL reference preparations but only 30% serum hPRL in basal state Major component of serum hPRL in basal state Reduced in hyper-prolactinaemic states Predominently dimers < 20% serum hPRL Aggregates < 5% serum hPRL Found in serum, ?formed in tissues Monomeric pituitary hPRL 23 hPRL/6 Glycosylated hPRL (G-hPRL) 25 hPRL/6 'Big' hPRL 50-60 hPRL/6 'Big big' hPRL Fragments > !OO 16,8, etc. hPRL/6 hPRL!6 ably from any of the non-primate GHs in both amino-acid sequence and biological activity, with hGH the only GH with substantial lactogenic activity. Although hPRL is less different from most non-primate PRLs, rat PRL differs considerably in amino-acid sequence from other mammalian PRLs. 5 The hPRL gene appears to be present 'as a single copy and is located on chromosome 6.6 The hGH gene cluster is found on chromosome 17,7 and probably consists of the normal human pituitary hGH gene (hGH-N), three human placental lactogen (hPL) genes, one of which may be non-functional, and the hGH-variant (hGH-V) gene. 8•9 All these genes have in common a five-exon structure and each encodes a protein product of 22-26 kD molecular weight. The expression of the hGH-N gene is restricted to the somatotrophs of the anterior pituitary; expression of the hPL genes is restricted to the syncytiotrophoblast cells of the placenta. The hGH-V gene has recently been shown to be expressed in the placenta." The hPRL gene is expressed in the pituitary lactotrophs, the decidua of the placenta and in luteal phase endometrium. 2). There is considerable (42%) homology between the coding sequences of the hPRL and hGH genes. The structures of both hormones are stabilized by intra-chain disulphide bonds. The three-dimensional structure of a genetically-engineered variant of porcine GH was determined recently:" a large proportion of the molecule was found to consist of four IXhelices folded to form a compact globular structure. In view of the similarities in amino-acid sequence, it is likely that hGH and hPRL assume a similar shape. Elegant studies by Cunningham et al. 15•16 of the effects on binding characteristics of mutations introduced at various points have allowed the mapping of receptor and monoclonal antibody binding sites on the hGH molecule. The receptor binding-site consists of three sequences, MOLECULAR STRUCfURE OF hPRL AND hGH hPRL is a single-chain polypeptide with an approximate molecular weight (MW) of 23 kD (Fig. 1). Amino-acid sequencing of hPRL derived from a pool of normal pituitaries suggested a 198 amino-acid sequence. I I More recently, sequencing of hPRL cDNA from pituitary adenoma tissue has revealed an almost identical 199 amino-acid sequence. 12 hGH is also a singlechain protein, with the major circulating form having 191 residues and a MW of 22 kD 1J (Fig. COOH FIGURE 1. Monomeric hPRL. A polypeptide of 199 amino acids with three disulphide bridges. 544 Smith and Norman arnino-acids.v" It is likely that the recentlydescribed hGH-like peptide found in maternal serum in the third trimester" represents the product of the hGH-V gene expressed in the placenta. It has recently been reported that, as for the product of the hGH-N gene, alternative splicing of the hGH-V gene primary transcript can result in the production of two distinct proteins (designated hGH-V and hGH_V2).18.19 There is no evidence for more than one hPRL gene and variant forms of hPRL appear to be post-translational modifications of the product of a single gene. FIGURE 2. Monomeric hGH. A polypeptide of 191 amino acids with two disulphide bridges. remote in the linear sequence, which are contiguous when the molecule is folded (Fig. 3). VARIANT FORMS DERIVED FROM DIFFERENT GENES The hGH-N gene directs the synthesis of the 22 kD polypeptide, pituitary hGH, and a posttranscriptionally modified form, hGH 2okD , which is described below and constitutes approximately 10% of pituitary hGH. The hGH-V gene codes for an hGH-like hormone which differs from pituitary hGH in 13 3. Three-dimensional structure of hGH showing the receptor binding site. The structure is based on that determined for porcine growth hormone," with ex helices represented by cylinders. Sites ofmutations which increase ( "") or decrease (.) binding to receptor were determined by Cunningham and weus." Reproduced by kind permission ofthe Authors and the Editor of Science. hGH20kD Translation ofmRNAs derived from the hGH-N gene results in synthesis of two distinct polypeptides, hGH m D and hGH 2okD • It is now clear that the smaller peptide is formed as a result of the use of an alternative splice-acceptor site within exon 3 of the hGH-N gene,18.20 resulting in an internal deletion of bases coding for 15 amino acids" (Fig. 4). The regulation of gene processing by the two routes is not understood. A third mRNA variant lacking the entire third exon has also been detected in pituitary tumour tissue," but the predicted 17·5 kD protein product has not yet been definitively identified. There is no evidence for the existence of analogous hPRL variant forms. FIGURE FIGURE 4. The 20 kD variant ofhGH. The sequence of 15 amino acids deleted in this variant is represented by a dashed line. Pro/actin and growth hormone POST-TRANSLATIONAL MODIFICATIONS Glycosylation A glycosylated form of hPRL (G-hPRL) is consistently found in human pituitaries and sera." An oligosaccharide side-chain is attached at Asn., , resulting in a molecule of apparent MW 25 kD determined by sodium dodecyl sulphate (SDS) electrophoresis. Recent work shows that G-hPRL is a major circulating form in normal sera." We have found that G-hPRL constituted approximately 70% of total monomeric hPRL in a study of 42 normal subjects. The proportion of G-hPRL falls with increasing levels of serum hPRL, and some patients with extremely high hPRL levels may have no detectable G-hPRL in their serum." Very recent work suggests that there may be more than one form of G-hPRL. 26 G-hPRL is also found in amniotic fluid and is a secretory product of luteal phase endometrium" and also of placenta." The Asn-Gln/Leu-Ser sequence at which Nlinked glycosylation occurs does not occur in pituitary hGH but is present in the placental variant. Work by Ray et al. 29 suggests that hGHV is modified by N-linked glycosylation in a fibroblast cell-line, and there is some evidence that the placental product is glycosylated in man." Charge variants Charge variants of both hormones, such as acetylated and deamidated forms, have been described in serum; it is not clear whether these represent artefacts or secreted forms." Aggregates and oligomers Fractionation of serum by gel filtration consistently reveals three major species of hGH: MW approximately 20-22 kD (monomeric or little hGH), 40-50 kD (big hGH) and> 60 kD (big big hGH).32 Similarly, three species of hPRL are found in serum with MW 23 kD (monomeric or little hPRL), 50-60 kD (big hPRL), and > lOOkD (big big hPRL).33-3s 'Big big' forms of both hormones are mainly non-covalently bound aggregates.l":" and in the case of hPRL may be glycosylated." The complex formed by hGH and its serum binding protein (see below) probably accounts for most 'big big' hGH. 37 'Big' forms of both hormones are predominantly dimers,32.38 some disulphidelinked, which appear to be secretory products. High molecular weight forms of hGH normally represent approximately 15-50% of total im- 545 munoactive hGH in serum.V The proportion of 'little' hGH has been shown in one study to be higher in acromegalic patients." Less than 20% of serum hPRL is present in high MW forms in sera from both normal subjects and some patients with hyperprolactinaernia,":" although higher proportions of high MW forms of hPRL are found in some patients with pituitary tumours.":" Some women with hyperprolactinaemia and normal ovarian function have been shown to have very high levels of high molecular weight hPRL in their serum.4(}-42 Proteolytically eleaved forms and fragments When circulating hPRL and hGH are subjected to immunoelectrophoresis under reducing conditions several low MW forms are detected. It has been suggested that the intact monomeric form of each hormone may be subjected to sequential attack by specific proteases to generate biologically active fragments with different functions.i':" Modified forms of both hormones have been described in which the large loop is opened; subsequent reduction of the intrachain disulphide bonds generates low molecular weight fragments. Cleaved forms ofhPRL appear to be present in tissues such as pituitary and ovary and have also been demonstrated in serum from pregnant women." It is not certain that low MW fragments are produced in vivo, but this idea has generated considerable interest in view of evidence that the 16kD fragment of rat PRL is biologically active despite reduced immunoactivity and may have important local effects. 43.4S Immunoactive hGH variants of MW 12-30 kD may contribute significantly to the total immunoactivity of hGH in normal sera in the basal state;" their contribution to hGH bioactivity is unknown. However, fragments of hGH generated in vitro have been shown to have enhanced activity in some bioassays" and may act through specific receptors. Their physiological functions are unknown. SERUM BINDING PROTEINS Until recently it was thought that both hormones existed free in the circulation. It has recently become clear however that a specific, high-affinity, low-capacity hGH binding protein (BP) exists in human plasma." Under physiological conditions, about 50% of hGH m D and 30% of hGH 20kD are bound. The rabbit GH BP has the 546 TABLE Smith and Norman 3. Significance of major circulating variants of hGH Variant Analytical importance Physiological importance hGH 20kD Immunoactivity 10-30% that of hGH m D Growth activity = hGH m D ?Insulin-like and receptor-binding activity reduced" Immunoactivity of aggregates usually reduced. Bioactivity considerably reduced in in vitro bioassays Binding to a minor serum BP may reduce RIA activity by 10-15% May have increased or decreased bioactivity t 1/2 in serum may be increased 2 or 3fold compared with hGH m D and in vivo bioactivity norma!'] 'Big' and 'big big' Fragments Placental hGH Not distinguishable from pituitary hGH in routine assays same amino-acid sequence as the amino-terminal end of the GH receptor, suggesting that in this species the BP is the free extra-cellular domain of the receptor." This relationship between the serum binding protein and the hGH receptor has not been confirmed in man. As yet, no convincing evidence for a hPRL serum BP has been obtained. The effect of the hGH BP on the measurement of hGH levels in blood is likely to be dependent on the relative affinities for hGH of the antiserum used in the assay and the BP. Preliminary data from Baumann et a/. 37 suggest that the affinity of antiserum for bound hGH is likely to exceed that of the BP, so hGH will preferentially bind to the antiserum. The complex of hGH with the major BP is in fact fully immunoactive, although a small proportion of hGH bound to a minor BP may be underestimated by RIA. This is unlikely to represent more than 10-15% of total plasma hGH. TABLE 4. Proportion of large forms not altered by pituitary stimulation High serum levels of aggregates may be associated with short stature (rare) Effect of binding to BP on in vivo bioactivity not known ? Produced in vivo by the action of tissue proteases, May have specific actions The major component of hGH in maternal serum in late pregnancy. Physiological significance unknown CLINICAL SIGNIFICANCE OF MOLECULAR HETEROGENEITY The full clinical significance of the variant forms of the hormones is unclear. Tables 3 and 4 summarize what is known about the physiological and analytical significance of variant forms of both hormones in serum. The properties of modified forms of the hormones may help us to understand situations where there appear to be discrepancies between the results of immunoassay measurements of the ho~ones and the clinical picture. The preservation of normal ovarian function, with maintained fertility, in women with very high immunoassayable hPRL levels is one such example/":" Such women have been shown to have high serum levels of high MW hPRL oligomers which may be of reduced bioactivity." Current immunoassay methods do not allow the routine detection of such patients, who may not require treatment, Significance of major circulating variants of hP RL Variant Analytical significance Physiological significance G-hPRL Activity reduced in Nb2 bioassay (by 50%) significantly underestimated in most immunoassays (by 50-70%) Activity reduced in both bioassays and immunoassays Unknown ? Specific function in pregnancy 'Big' and 'big big' hPRL Fragments Bioactivity much increased relative to immunoactivity in some fragments (in the rat, no data in man) Ovulatory hyper-prolactinaemia may be associated with high levels of large forms ? Produced in tissues Specific actions unknown: may have paracrine actions different from parent hormone Prolactin and growth hormone although serial dilution of their sera may show non-parallelism with monomeric hPRL standard." Similarly, immunoactive but bioinactive hGH has been suggested as a cause of short stature. Subnormal ratios of hGH radioreceptor or bioassay activity to immunoactivity have been found in a smalI number of children, who respond weli to treatment with hGH. 48- 1O One such case of growth failure due to bioinactive hOH was shown to be caused by the presence in serum of large amounts ofhOH oligomers which showed decreased binding to the hGH receptor of human IM9 lymphocytes. 51 ANALYTICAL SIGNIFICANCE OF MOLECULAR HETEROGENEITY Immunoassays depend on the binding of one or more antibodies to binding sites on the target hormone; such sites may be distant from the binding sites for physiologicalIy-relevant ligands. Immunoassays may thus detect biologicalIy inactive hormone fragments or aggregates, or fail to detect bioactive fragments where the assay antibody binding site is absent or obscured. Antibodies for use in immunoassays are usualIy raised against the unmodified monomeric form of the hormone, and may not detect modified but bioactive forms. Reference preparations for use in immunoassay also consist of purified monomeric hormone and so may not reflect the composition of the hormone in the serum being assayed. In view of the marked fluctuations in the proportions of hOH and hPRL variants with different MWs and immunoactivities in serum, there is a strong case for continuing to report results of assays for these hormones in international units rather than mass units. The molecular heterogeneity of the hormones raises the question of the significance of possible in vitro interconversions between forms, particularly mass variants. Variable conversion of high to low molecular weight forms of both hormones is known to occur with treatment with reducing agents, or multiple freeze-thaw cycles. Under usual assay conditions this does not appear to cause problems, but there is some evidence that heat treatment of serum, as may be used for HIV positive samples, can significantly alter apparent immunoactivity in at least one RIA. 52 Comparisons between different immunoassays Systematic comparisons between assays using 547 different antisera are carried out as part of the validation of new methods but there are few published reports in the UK literature. In the case of hPRL, some antisera recognize high MW variants less welI than others":" and this may explain the non-paralIelism sometimes found on dilution of samples with very high hPRL concentrations. Immunoradiometric assays (IRMAs) using monoclonal antibodies, usualIy directed at two non-overlapping epitopes to form a 'sandwich', tend to give lower estimates of hPRL levels than do radioimmunoassays (RIAs) or bioassays'v" and may not recognize some forms of the hormone. Comparisons of hOH results by different immunoassays provide evidence of considerable variation; up to three-fold differences in absolute results, both between RIA and IRMA and between different IRMAs have been reported.":" A least one commercial IRMA does not detect hOH 2okD at alI.57 Such data re-emphasize the importance of establishing familiarity with one assay method and appropriate local reference and 'action' ranges. Similar problems have been experienced with IRMAs for gonadotropins. 58 Comparison between immunoassay and bioassay results The recent development of a relatively simple and convenient bioassay for lactogenic hormones has facilitated comparative studies of their biological and immunoactivity. The Nb2 celI assay" uses a celI line derived from a lymphoma which developed in an oestrogen-treated male rat. The celIs proliferate in response to both hOH and hPRL: the assay can be made specific by using monoclonal antibodies or antisera to block one hormone. There are now several studies reporting altered hPRL bioactivity:immunoactivity (B:I) ratios in situations where hPRL molecular heterogeneity is known to be altered. Using the Nb2 cell bioassay, we,bO and others," have found bioactivity to be reduced compared with immunoactivity in some patients with prolactinomas. This may relate to the reduction in the proportion of serum hPRL which is glycosylated in sera from these patients, since glycosylation has significant effects on both the bioactivity and immunoactivity of the molecule.F:" In uraemic or myxoedematous patients we/ 5•M like Rowe et al.,65 have been unable to demonstrate major differences between hPRL activity in the Nb2 assay and in immunoassays, although other workers have reported changes. 66.67 There are fewer studies of B:I ratios ofhOH in 548 Smith and Norman serum. The insensitivity of even the Nb2 assay for hGH makes measurement of unstimulated hGH levels or confirmation of reduced bioactivity difficult in children with short stature, and results are conflicting.v?" Using the Nb2 assay, we and others have found no change in B:I ratios in sera from acromegalic patients after stimulation of the pituitary.":" Discrepancies between studies of B:I ratios may relate to the immunoassay used for comparison with the bioassay, and definitive answers await the isolation of individual variants such as G-hPRL in sufficient amounts for their use as standards and to raise specific antibodies. Since changes in the molecular heterogeneity of the hormone, such as glycosylation, affect both immunological and biological activities, determination of B:l ratios may conceal important changes in the proportions of hormone variants. CONCLUSIONS I. hGH and hPRL do not circulate as single molecular species but as 'families' of related forms. 2. In a few patients, the molecular heterogeneity of the hormones may help to explain clinical paradoxes. 3. The development of new immunoassay methods, including those involving monoclonal antibodies, is leading to recognition of variability between immunoassays; the importance of establishing reference ranges is emphasized. 4. Despite the heterogeneity of hPRL and hGH, immunoassay results generally correlate well with those of bioassays and will remain the standard method of measurement of these hormones in routine practice. In future assays for variants such as G-hPRL may provide additional information of clinical importance. 5. In view of the heterogeneity of the hormones, there is a good case for using international rather than mass units to express immunoassay results. Acknowledgements We thank Mr Barry Pike for his help with the preparation of the figures, and Miss Joan Butler for critical review of the manuscript and helpful comments. During the writing of this review, Caroline Smith was a Wellcome Trust Research Training Fellow. REFERENCES I Pierce JG, Parsons TF. Glycoprotein hormones: structure and function. Ann Rev Biochem 1981; 50: 465-95 2 Dufau ML, Veldhuis JD. Pathophysiological relationships between the biological and immunological activities of luteinizing hormone. In: Burger HG, ed. Reproductive Endocrinology. Bailliere's Clinical Endocrinology and Metabolism, Vol. I (Feb). \987; pp 153-76 3 Hutchinson JSM. The interpretation of pituitary gonadotrophin assays-a continuing challenge. J Endocrinol 1988; 118: 169-7\ 4 Baenziger JU, Green ED. Pituitary glycoprotein hormone oligosaccharides: structure, synthesis and function of the asparagine-linked oligo saccharides on lutropin, follitropin and thyrotropin. Biochim Biophys Acta 1988; 947: 287-306 5 Wallis M. The molecular evolution of pituitary growth hormone, prolactin and placental lactogen: a protein family showing variable rates of evolution. J Mol EI'01198\; 17: 10-8 6 Owerbach D, Rutter WJ, Cooke NE, Martial JA, Shows TB. The prolactin gene is located on chromosome 6 in humans. Science 1981; 212: 8\5-6 7 Ower bach D, Rutter WJ, Martial JA, Baxter JD. Shows TB. Genes for growth hormone, chronic sommatomammotrophin and growth hormone-like gene on chromosome \7 in humans. Science 1980; 209: 289-92 8 Seeburg PH. The human growth hormone gene family: nucleotide sequences show recent divergence and predict a new polypeptide hormone. DNA 1982; 1: 239-9 9 Hirt H, Kime1man J, Birnbaum MJ, et al. The human growth hormone gene locus: structure, evolution and allelic variations. DNA 1987; 6: 59-70 10 Frankenne F, Rentier-Delrue F, Scippo ML, Martial J. Hennen G. Expression of the growth hormone variant gene in human placenta. J Clin Endocrinol Metab 1987; 64: 635-7 1\ Shome B, Parlow AF. Human pituitary prolactin: the entire linear amino acid sequence. J Clin Endocrinol Metab \977; 45: 1112-5 12 Cooke NE, Coit D, Shine J, Baxter JD, Martial JA. Human prolactin: cDNA structural analysis and evolutionary comparisons. J BioI Chem \981; 256: 4007-16 13 Li CH, Dixon JS. Human pituitary growth hormone. The primary structure of the hormone: revision. Arch Biochem Biophys 1971; 146: 233-6 14 Abdel-Meguid SS, Shieh H-S, Smith WW, Dayringer HE, Violand BN, Bentle LA. Three-dimensional structure of a genetically-engineered variant of porcine growth hormone. Proc Natl Acad Sci USA 1987; 84: 6434-7 15 Cunningham BC, Jhurani P, Ng P, Wells JA. Receptor and antibody epitopes in human growth hormone identified by homolog-scanning mutagenesis. Science 1989; 243: \330-6 16 Cunningham BC, Wells JA. High-resolution epitope mapping of hGH-receptor interactions by alanine-scanning mutagenesis. Science 1989; 244: 1081-5 Prolactin and growth hormone 17 Frankenne F, Closset J, Gomez F, Scippo ML, Smal J, Hennen G. The physiology of growth hormones in pregnant women and partial characterization of the placental GH variant. J Clin Endocrinol Metab 1988; 66: 1171-80 18 Cooke NE, Ray J, Watson MA, Estes PA, Kuo BA, Liebhaber SA. Human growth hormone gene and the highly homologous growth hormone variant gene display different splicing patterns. J Clin Invest 1988; 82: 170-5 19 Cooke NE, Ray J, Emery JG, Liebhaber SA. Two distinct species of human growth hormone-variant mRNA in the human placenta predict the expression of novel growth hormone proteins. J Bioi Chem 1988; 263: 9001-6 20 DeNoto FM, Moore DD, Goodman HM. Human growth hormone DNA sequence and mRNA structure: possible alternative splicing. Nucleic Acids Res 1981; 9: 3719-30 21 Lewis UJ, Singh RNP, Tutwiler GF, Sigel MB, VanderLaan EF, VanderLaan WP. Human growth hormone: a complex of proteins. Recent Prog Horm Res 1980; 36: 477-508 22 Lecomte CM, Renard A, Martial J. A new natural hGH variant-17'5kD-produced by alternative splicing. Nucleic Acids Res 1987; 15: 6331-8 23 Lewis UJ, Singh RNP, Sinha YN, VanderLaan WP. Glycosylated human prolactin. Endocrinology 1985; 116: 359-63 24 Markoff E, Lee DW. Glycosylated prolactin is a major circulating variant in human serum. J Clin Endocrinol Metab 1987; 65: 1102-6 25 Hashim lA, Aston R, Butler J, McGregor AM, Smith CR, Norman MR. The proportion of glycosylated prolactin in serum is decreased in hyperprolactinaemic states. J Clin Endocrinol Metab 1990; 71: 111-15 26 Lewis UJ, Singh RNP, Lewis LJ. Two forms of glycosylated human prolactin have different pigeon crop-sac stimulating activities. Endocrinology 1989; 124: 1558-63 27 Heffner LJ, Iddenden DA, Lyttle CR. Electrophoretic analyses of secreted human endometrial proteins: identification and characterisation of luteal-phase prolactin. J Clin Endocrinol Metab 1986; 62: 1288-95 28 Lee DW, Markoff E. Synthesis and release of glycosylated prolactin by human decidua in vitro. J Clin Endocrinol Metab 1986; 62: 990-4 29 Ray J, Jones BK, Liebhaber SA, Cooke NE. Glycosylated human growth hormone variant. Endocrinology 1989; 125: 566-8 30 Hennen G, Frankenne F, Scippo M-L, et al. Hormone de croissance placentaire. Signification par rapport aux hormones de croissance et lactogene. Reprod Nutr Dev 1988; 28:1699-706 31 Baumann G, MacCart JG, Amburn K. The molecular nature of circulating growth hormone in normal and acromegalic man: evidence for a principal and minor monomeric forms. J Clin Endocrinol Metab 1983; 56: 946-52 32 Stolar MW, Amburn K, Baumann G. Plasma 'big' and 'big big' growth hormone in man: an oligomeric series composed of structurally diverse growth 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 549 hormone monomers. J Clin Endocrinol Metab 1984; 59: 212-8 Suh HK, Frantz AG. Size heterogeneity of human prolactin in plasma and pituitary extracts. J Clin Endocrinol Metab 1974; 39: 928-35 Whitaker MD, Klee G, Kao PC, Randall RV, Heser DW. Demonstration of biological activity of prolactin molecular weight variants in serum. J Clin Endocrinol Metab 1984; 58: 826-30 Garnier PE, Aubert ML, Kaplan SL, Grumbach MM. Heterogeneity of pituitary and plasma prolactin in man: decreased affinity of 'big' prolactin in a radioreceptor assay and evidence for its secretion. J Clin Endocrinol Metab 1978; 47: 1273-81 Shoupe D, Montz FJ, Kletzky OA, diZerega GS. Prolactin molecular heterogeneity. Response to thyrotropin-releasing hormone stimulation of concanavalin A bound and unbound immunoassayable prolactin during human pregnancy. Am J Obstet Gynecol 1983; 147: 482-7 Baumann G, Amburn K, Shaw MA. The circulating growth hormone binding-protein complex: a major constituent of plasma GH in man. Endocrinology 1988; 122: 976-84 Benveniste R, Helman JD, Orth DN, McKenna rr, Nicholson WE, Rabinowitz D. Circulating big human prolactin: conversion to small human prolactin by reduction of disulphide bonds. J Clin Endocrinol Metab 1979; 48: 883-6 Gordon P, Lesniak MA, Eastman R, Hendricks CM, Roth J. Evidence for higher proportion of 'little' growth hormone with increased radioreceptor assay activity in acromegalic plasma. J Clin Endocrinol Metab 1976; 43: 364-73 Jackson RD, Wortsman J, Malarkey WB. Characterization of a large molecular weight prolactin in women with idiopathic hyper-prolactinaemia and· normal menses. J Clin Endocrinol Metab 1985; 61: 258-63 Whittaker PG, Wilcox T, Lind T. Maintained fertility in a patient with hyperprolactinaemia due to big, big prolactin. J Clin Endocrinol Metab 1981; 53: 863-6 Andersen AN, Pedersen H, Djursing H, Andersen BN, Friesen HG. Bioactivity of prolactin in a woman with an excess of large molecular size prolactin, persistent hyperprolactinaemia and spontaneous conception. Fertit Steril 1982; 38: 625-8 Mittra I. Somatomedins and proteolytic bioactivation of prolactin and growth hormone. Cell 1984; 38: 347-8 Sinha YN, Gilligan TA, Lee DW, Hollingsworth D, Markoff E. Cleaved prolactin: evidence for its occurrence in human pituitary gland and plasma. J Clin Endocrinol Metab 1985; 60: 239-43 Clapp C, Sears PS, Russell DH, Richards J, LevayYoung BK, Nicoll CS. Biological and immunological characterization of cleaved and 16K forms of rat prolactin. Endocrinology 1988; 122: 2892-8 Baumann G, Stolar MW, Amburn K. Molecular forms of circulating growth hormone during spontaneous secretory episodes and in the basal state. J Clin Endocrinol Metab 1985; 60: 1216-20 Leung DW, Spencer SA, Cachianes G, et al. 550 Smith and Norman Growth hormone receptor and serum binding protein: purification, cloning and expression. Nature 1987; 330: 537--43 48 Rudman D, Kutner MH, Blackston RD, Cushman RA, Bain RP, Patterson JH. Children with normalvariant short stature: treatment with human growth hormone for six months. N Engl J Med 1981, 305: 123-31 49 Kowarski AA, Schneider J, Ben-Galim E, Weldon VV, Daughaday WHo Growth failure with normal serum RIA-GH and low somatomedin activity: somatomedin restoration and growth acceleration after exogenous GH. J Clin Endocrinol Metab 1978; 47: 461--4 50 Frazer TE, Gavin JR, Daughaday WH, Hillman RE, Weldon VV. Growth hormone-dependent growth failure. Pediatr Res 1980; 14: 478 (abstract) 51 Valenta LJ, Siegel MB, Lesniak MA, et al. Pituitary dwarfism in a patient with circulating abnormal growth hormone polymers. N Engl J Med 1985; 312: 214-7 52 Hardy MJ, Ragbeer SS. Effect of heat treatment for inactivation of HTLV III virus on serum immunoreactive prolactin. Ann Clin Biochem 1987; 24: 322--4 53 Jeffcoate SL, Bacon RRA, Beastall GH, Diver MJ, Franks S, Seth J. Assays for prolactin: guidelines for the provision of a clinical biochemistry service. Ann Clin Biochem 1986; 23: 638-51 54 Rose DP, Berke B, Cohen LA. Serum prolactin and growth hormone determined by radioimmunoassay and a two-site immunoradiometric assay: comparison with the Nb2 cell bioassay. Horm Metab Res 1988; 20: 49-53 55 Smith CR, Butler J, Iggo N, Norman MR. Serum prolactin in uraemia: correlations between bioactivity and activity in two immunoassays. Acta Endocrinol (Copenh) 1989; 120: 295-300 56 Reiter EO, Morris AH, MacGillivray MH, Weber D. Variable estimates of serum growth hormone concentrations by different radioassay systems. J Clin Endocrinol Metab 1988; 66: 68-71 57 Celniker AC, Chen AB, Wert RM, Sherman BM. Variability in the quantitation of circulating growth hormone using commercial immunoassays. J Clin Endocrinol Metab 1989; 68: 469-76 58 Wheeler MJ, D'Souza A, Horn AN. Evaluation of test kits for gonadotropins. Lancet 1989; ii: 616-7 59 Tanaka T, Shiu RPC, Gout PW, Beer CT, Noble RL, Friesen HG. A new sensitive and specific bioassay for lactogenic hormones: measurement of prolactin and growth hormone in human serum. J Clin Endocrinol Metab 1980; 51: 1058-63 60 Smith CR, Butler J, Hashin lA, Norman MR. Serum prolactin bioactivity and immunoactivity in hyperprolactinaemic states. Ann Clin Biochem 1990; 27: 3-8 61 Subramanian MG, Spirtos NJ, Moghissi KS, Magyar DM, Hayes MF, Gala R. Correlation and 62 63 64 65 66 67 68 69 70 71 72 73 comparison of NB2 lymphoma cell bioassay with radioimmunoassay for human prolactin. Fertil Steril 1984; 42: 870--4 Markoff E, Sigel MB, Lacour N, Seavey BK, Friesen HG, Lewis UJ. Glycosylation selectively alters the biological activity of prolactin. Endocrinology 1988; 123: 1303-6 Pellegrini I, Gunz G, Ronin C, et al. Polymorphism of prolactin secreted by human prolactinoma cells: immunological, receptor binding and biological properties of the glycosylated and non-glycosylated forms. Endocrinology 1988; 122: 2667-74 Smith CR, Butler J, Norman MR. Biological activity of serum prolactin in patients with primary hypothyroidism. Ann Clin Biochem 1988; 25: 540-5 Rowe RC, Cowden EA, Fairnan C, Friesen HG. Correlation of Nb2 bioassay and radioimmunoassay values for human serum prolactin. J Clin Endocrinol Metab 1983; 57: 942-6 Mooradian AD, Morley JE, Korchik WP, Ma KW, Hartel MA, Parsons JA. Comparison between bioactivity and immunoreactivity of serum prolactin in uraemia. Clin Endocrinol 1985; 22: 241-7 Silverman A Y, Schwartz SL, Steger RW. A quantitative difference between immunologically and biologically active prolactin in hypothyroid patients. J Clin Endocrinol Metab 1982; 55: 272-5 Tokuhiro E, Dean H, Friesen HG, Rudman D. Comparative study of serum human growth hormone measurement with Nb2 lymphoma cell bioassay, IM9 receptor modulation assay and radioimmunoassay in children with disorders of growth. J Clin Endocrinol Metab 1984; 58: 549-54 Sneid D, Jacobs L, Weldon V, Trivedi B, Daughaday W. Radioreceptor-inactive growth hormone associated with stimulated secretion in normal subjects. J Clin Endocrinol Metab 1975; 41: 471--4 Gamier P, Job J-c. Correlative study of radioreceptor assay and radioimmunoassay of serum growth hormone in children: normal children and hGH-treated pituitary dwarfs. Acta Endocrinol ( Copenh ) 1977; 86: 50-9 Baldwin AL, Aston R, Butler J, Buchanan C, Norman MR. Bioactivity and immunoactivity of growth hormone during dynamic testing of patients with acromegaly. Ann Clin Biochem 1988; 119: 32632 Tanaka T, Shishiba Y, Gout P, Beer C, Noble R, Friesen HG. Radioimmunoassay and bioassay of human growth hormone and human prolactin. J Clin Endocrinol Metab 1983; 56: 18-20 Baumann G, Stolar MW, Buchanan TA. Slow metabolic clearance rate of the 20,OOO-Dalton variant of human growth hormone: implications for biological activity. Endocrinology 1985; 117: 1309-13 Accepted for publication 23 May 1990