Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
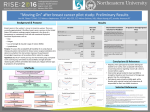
AnMed Health Cancer Care Major Site Report Breast Cancer Major Site Report – Breast Cancer Lumpectomy vs Mastectomy for Early Stage Invasive Breast Cancer For women with a choice in early breast cancer treatment, lumpectomy plus radiation therapy (lumpectomy + RT) is considered as effective as mastectomy. What are the differences between lumpectomy and mastectomy? Type of surgery Lumpectomy is the surgical removal of the tumor and some of the normal tissue surrounding it (not the entire breast). This surgery removes less tissue than mastectomy and can leave the breast looking as close as possible to the way it did before surgery. Most often, the shape of the breast and the nipple area are preserved. After a lumpectomy, a pathologist checks the tumor margins (the normal tissue surrounding the tumor) to make sure all the cancer has been removed. When the margins contain no cancer cells (negative margins), the lumpectomy is successful. However, if the margins contain cancer cells, more surgery must be done. In these cases, a lumpectomy may no longer be an option and a mastectomy may be needed. Mastectomy is the surgical removal of the entire breast. In a total (simple) mastectomy, the surgeon removes the breast, but no other tissue or lymph nodes. In a modified radical mastectomy, the surgeon removes the breast, the lining of the chest muscles and some of the lymph nodes in the armpit. Breast reconstruction may be done at the same time as the mastectomy or at a later date. Radiation therapy (RT) Radiation therapy to the breast is standard after a lumpectomy. It gets rid of any cancer cells that may remain after surgery. This lowers the chances of the cancer returning. In contrast, most women do not need radiation therapy after a mastectomy. Chemotherapy and hormone therapy Having lumpectomy + RT or mastectomy does not affect whether or not a woman’s treatment will also include chemotherapy or hormone therapy. These choices are related to the characteristics of the tumor rather than the type of surgery. Risk of lymphedema Lymphedema is a condition where lymph fluid collects in the arm, hand, finger or chest causing swelling. The risk of lymphedema is the same whether a woman chooses lumpectomy + RT or mastectomy. Women who have a large number of lymph nodes in the armpit removed during either type of breast surgery or who have radiation to these lymph nodes are more likely to develop lymphedema.1 When is lumpectomy + RT an option? Not all women are candidates for lumpectomy + RT. In some cases, the location or size of the tumor make mastectomy a better option than lumpectomy. These include:2 • • • • • Two or more tumors in different areas of the breast (multi-centric tumors) A large tumor, relative to breast size (for some women neoadjuvant therapy may reduce the size of the tumor enough so that lumpectomy is possible) A tumor spread throughout the breast (diffuse tumor) Attempts at lumpectomy cannot get negative margins Inflammatory breast cancer Women treated with lumpectomy must have radiation therapy. Therefore, those who cannot have radiation therapy due to certain health conditions may need to have a mastectomy instead. These conditions include:2 • • • Scleroderma or systemic lupus Past radiation therapy to the same breast Pregnancy (radiation therapy is not given during pregnancy, but women can have a lumpectomy during pregnancy and have radiation therapy after delivery) Lumpectomy + RT versus mastectomy in treating early breast cancer Overall survival Findings from randomized controlled trials, meta-analyses and pooled analyses show there is no difference in overall survival between women with early breast cancer treated with lumpectomy + RT and those treated with mastectomy.3-9 Details of these studies are presented in Table 37 in the research section. Local and distant recurrence The chance of the cancer returning in the breast (called local recurrence) is slightly higher with lumpectomy + RT than mastectomy.4,6,8,9 However, the risk of cancer spreading to other organs (called distant recurrence or metastasis and the main cause of breast cancer death), is the same for lumpectomy + RT and mastectomy.3,4,6 Summary of risks and benefits: lumpectomy + RT versus mastectomy There are risks and benefits to consider when choosing between lumpectomy + RT and mastectomy. The main benefit of lumpectomy + RT is that the breast is preserved as much as possible. The main benefit of mastectomy is that radiation therapy may not be needed. This can be an important factor for women who live far from a radiation treatment center. And, although lumpectomy + RT and mastectomy are equally effective in treating early breast cancer, for some women, mastectomy offers more peace of mind. Mastectomy Amount of tissue removed Extent of surgery Hospital stay Radiation therapy Chance of local recurrence Entire breast Major surgery with general anesthesia Overnight hospital stay may be needed Longer recovery time than with lumpectomy + RT Sometimes done Low Lumpectomy + RT Part of breast (preserves the look of the breast as much as possible) Less extensive surgery with general anesthesia Often go home on same day as surgery Routinely done Low (but slightly higher than with mastectomy) According to Dr. Terry Mamounas, Professor of Surgery, Northeastern Ohio Universities College of Medicine and Medical Director, Aultman Cancer Center, Canton, OH, “Currently most women with early-stage breast cancer are candidates for lumpectomy and radiation therapy. This approach preserves the breast and provides the same overall survival to that achieved with total mastectomy. Advances in imaging and surgical techniques, radiation therapy and adjuvant systemic therapy have resulted in significant reduction in the rates of local recurrence after lumpectomy, making this procedure the preferred method of surgical management for the majority of patients with early-stage breast cancer.” References 1. McLaughlin SA, Cohen S, Van Zee KJ. Chapter 45: Lymphedema, in Harris JR, Lippman ME, Morrow M, Osborne CK. Diseases of the Breast, 4th edition. Lippincott Williams and Wilkins, 2010. 2. Kaufmann M, Morrow M, von Minckwitz G, Harris JR; Biedenkopf Expert Panel Members. Locoregional treatment of primary breast cancer: consensus recommendations from an International Expert Panel. Cancer. 116(5):1184-91, 2010. 3. Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, Jeong JH, Wolmark N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 347(16):123341, 2002. 4. van Dongen JA, Voogd AC, Fentiman IS, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst. 92(14):1143-50, 2000. 5. Blichert-Toft M, Nielsen M, Düring M, et al. Long-term results of breast conserving surgery vs. mastectomy for early stage invasive breast cancer: 20-year follow-up of the Danish randomized DBCG-82TM protocol. Acta Oncol. 47(4):672-81, 2008. 6. Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 347(16):1227-32, 2002. 7. Early Breast Cancer Trialists' Collaborative Group. Effects of Radiotherapy and Surgery in Early Breast Cancer. An Overview of the Randomized Trials. N Engl J Med. 333:1444-55, 1995. 8. Jatoi I, Proschan MA. Randomized trials of breast-conserving therapy versus mastectomy for primary breast cancer: A pooled analysis of updated results. Am J Clin Oncol. 28(3):289-94, 2005. 9. van der Hage JA, Putter H, Bonnema J, et al. on behalf of the EORTC Breast Cancer Group. Impact of locoregional treatment on the early-stage breast cancer patients: a retrospective analysis. Eur J Cancer. 39(15):2192-9, 2003. 10. Morrow M, Jagsi R, Alderman AK, et al. Surgeon recommendations and receipt of mastectomy for treatment of breast cancer. JAMA. 302(14):1551-6, 2009. 11. Habermann EB, Abbott A, Parsons HM, Virnig BA, Al-Refaie WB, Tuttle TM. Are mastectomy rates really increasing in the United States? J Clin Oncol. 28(21):3437-41, 2010. 12. Alderman AK, Bynum J, Sutherland J, Birkmeyer N, Collins ED, Birkmeyer J. Surgical treatment of breast cancer among the elderly in the United States. Cancer. 2010 Sep 30. [Epub ahead of print]. Rhonda Ballew, RN Coordinator Oncology Research/ CC Data Management Mastectomy versus Lumpectomy plus Radiation and Overall Survival in Early Stage Breast Cancer This summary table contains detailed information about research studies. Summary tables offer an informative look at the science behind many breast cancer guidelines and recommendations. Introduction: For women who have the option, lumpectomy (also called breast conserving surgery) plus radiation therapy is just as effective as mastectomy for treating early breast cancer. The randomized controlled trials, pooled analyses and meta-analyses in the table below show there is no difference in overall survival between women treated with either method. Study selection criteria: Randomized clinical trials with at least 150 participants and at least 10 years of followup, pooled analyses and meta-analyses. Study Study Population (number of participants) Stage of Follow-up Breast (years) Cancer Overall Survival (for length of follow-up) Mastectomy Lumpectomy plus Radiation Randomized clinical trials NSABP B06 [1] 1,851 Stage I-II 21 47% 46%NS EORTC [2] 868 Stage I-II 22 45% 39%NS Danish Breast Cancer Cooperative Group [3] 731 Stage I-III 20 58% 51%NS Milan [4] 701 Stage I 20 58% 59%NS National Cancer Institute [5] 237 Stage I-II 26 44% 38%NS Arriagada [6] 179 Stage I 22 52% 60%*NS Pooled and meta-analyses 71%NS EBCTCG [7] 4,891 Stage I-II 10 Jatoi et al. [8] 4,061 Stage I-II 15 NS NS van der Hage et al. [9] 3,648 Stage III/III 11 68% 72% 71% NS = No statistically significant difference between the two groups References 1. Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, Jeong JH, Wolmark N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 347(16):123341, 2002. 2. Litière S, Werutsky G, Fentiman IS, et al. Breast conserving therapy versus mastectomy for stage III breast cancer: 20 year follow-up of the EORTC 10801 phase 3 randomised trial. Lancet Oncol. 13(4):412-9, 2012. 3. Blichert-Toft M, Nielsen M, Düring M, et al. Long-term results of breast conserving surgery vs. mastectomy for early stage invasive breast cancer: 20-year follow-up of the Danish randomized DBCG-82TM protocol. Acta Oncol. 47(4):672-81, 2008. 4. Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 347(16):1227-32, 2002. 5. Simone NL, Dan T, Shih J, et al. Twenty-five year results of the national cancer institute randomized breast conservation trial. Breast Cancer Res Treat. 132(1):197-203, 2012. 6. Arriagada R, Le MG, Guinebretiere JM, Dunant A, Rochard F, Tursz T. Late local recurrences in a randomised trial comparing conservative treatment with total mastectomy in early breast cancer patients. Ann Oncol. 14(11):1617-22, 2003. 7. Early Breast Cancer Trialists' Collaborative Group. Effects of Radiotherapy and Surgery in Early Breast Cancer. An Overview of the Randomized Trials. N Engl J Med. 333:1444-55, 1995. 8. Jatoi I, Proschan MA. Randomized trials of breast-conserving therapy versus mastectomy for primary breast cancer: A pooled analysis of updated results. Am J Clin Oncol. 28(3):289-94, 2005. 9. van der Hage JA, Putter H, Bonnema J, et al. on behalf of the EORTC Breast Cancer Group. Impact of locoregional treatment on the early-stage breast cancer patients: a retrospective analysis. Eur J Cancer. 39(15):2192-9, 2003. Rhonda Ballew, RN Coordinator Oncology Research/ CC Data Management Lumpectomy vs Mastectomy Study - Stage 0, I, II Breast Cancer Patients (2012) Patient Sampling - Ananlytic Cases 205 - 188 Cases Identified for Review Patients had Lumpectomy Patients with lumpectomy who went on to mastectomy Patients having Mastectomy only *Patients who had surgery elsewhere or no surgery 105 12 71 188 17 205 *Surgery elsewhere - 13 patients *No surgery - 4 A) One patient presented with three primaries, patient expired prior to surgical treatment. B) One refused surgery C) Two were aged 84/87 with multiple comorbidities Results: NAPBC guidelines state at least 50% of women diagnosed with early stage (0-II) breast cancer should be treated with breast conservation therapy (lumpectomy + radiation therapy). Based on 2012 analytic data AnMed Health has a 56% lumpectomy rate, well above the NAPBC recommendations. Rhonda Ballew RN 21-Oct-13 By % Lumpectomy vs Mastectomy Rate - Dx/Tx at AnMed vs Tx Elswhr 2012 Analytic Total Breast Cases Stage 0-2 205 Page #s 1 2 3 4 5 6 7 8 9 10 11 12 13 Lumpectomy 8 7 9 8 5 10 8 8 13 8 10 10 1 *Mastectomy 1 1 0 2 2 0 0 2 0 1 3 0 0 Total 105 51.2% 12 5.9% Total Surgeries Lumpectomies Lumpectomy Rate Mastecomies Mastectomy Rate Mastectomy Only 5 6 8 5 6 6 7 3 6 8 5 6 0 Surgery Elswhere 0 1 1 2 1 1 1 3 0 2 0 1 0 No Surgery 0 0 0 0 1 1 1 1 0 0 0 0 0 Number of Patients 14 15 18 17 15 18 17 17 19 19 18 17 1 71 34.6% 13 6.3% 4 2.0% 205 100% % Lump to Mastec 11.4% 188 105 56% 83 44% *Mastectomy: Lumpectomy first, then went on to have Mastectomy ** NAPBC recommends 50% lumpectomy or better Source: CC Data Mmgnt 10, 2013 Page 1 CROSS-TABULATION OF SITE CODE BY CANCER DIRECTED SURGERY HERE FOR 10-LUMP-VS-MASTEC-DX-TX-RHONDA-B SITE COD LUMPECTOMY NBR (%) BREAST 105 MASTECTOMY NBR (%) 51.2 83 ALL OTHERS NBR (%) 40.5 17 DEPENDANT VARIABLES LUMPECTOMY is CANCER DIRECTED SURGERY HERE 20-24 MASTECTOMY is CANCER DIRECTED SURGERY HERE 30-80 TOTAL VALUES NBR (%) 8.3 205 100 Evaluation and Treatment Planning Study – 2014 Breast Cancer Diagnostic Evaluation per NCCN Guidelines: First course of treatment concordant with NCCN recommendations Physician Review – CoC Standard 4.6 A sample selection of 20 analytic invasive breast cancer cases were identified by the registry department and provided for review. Each case was evaluated for the following items according to current NCCN guidelines; • • • • • Family history documented Appropriate lab evaluation (CBC, platelet, LFT’s) Bilateral diagnostic mammogram Determination of ER, PR & HER2/neu for invasion First course of treatment After careful review the following findings were observed and documented for physician review; • • • • • 100% of the cases reviewed had family history documented 100% of the cases reviewed had the recommended lab evaluations performed and documented 19 of 20 cases reviewed (95%) had ER, PR, HER2/neu determination performed. The lone case for which this was not done had insufficient material at biopsy to perform the test and no residual neoplasia in the surgical specimen. 100% of eligible cases had the testing performed. 100% of the cases reviewed has first course of therapy concordant with NCCN guidelines based on the results of the diagnostic workup. 25% of the patients underwent bilateral diagnostic mammogram as recommended by NCCN guidelines. (In lieu of this finding, after physician review and presentation to the QI committee, it was felt further investigation was needed to determine the reasoning behind the difference in diagnostic workup here and the recommended evaluation by NCCN). Post review findings: Upon diagnosis of invasive breast cancer AnMed Health patients undergo a unilateral diagnostic mammogram and ultrasound then proceed straight to MRI for preoperative staging and surgical planning. The NCCN guidelines lists in its most recent literature that “MRI is optional and may be used for staging evaluation to define extent of cancer or presence of multifocal or multicentric cancer in the ipsilateral breast, or as screening of the contralateral breast at time of diagnosis”. It was felt by the radiologists that preoperative MRI was more effective for staging the extent of the disease and helped provide useful information in determining suitability for breast conservative surgery vs mastectomy. Rhonda Ballew, RN October 2014 MRI IN THE PREOPERATIVE EVALUATION: THE DEBATE Numerous reports have shown that MRI can detect additional foci of breast cancer in a substantial number of women with a new diagnosis of breast cancer. While some argue that detecting these additional lesions should improve outcomes after the first operation and, hopefully, lead to lower rates of recurrence, the long-term consequences of MRI-directed changes in treatment have not been fully studied. Below is a summary of the arguments both against and for the use of breast MRI in staging. • The argument against preoperative MRI Mastectomy was the routine treatment for breast cancer into the 1980s. The arrival of breast conservation surgery combined with radiation therapy offered major advantages with similarly low recurrence rates. Based on the results of controlled clinical trials with mortality as the end point, breast conservation therapy and mastectomy confer equivalent risk to the patient. Any increase in the rate of mastectomy prompted by MRI findings would represent a setback in the standard of care. And since radiation therapy is presumed to eradicate or delay progression of residual disease in most women who undergo conservation therapy, preoperative MRI would have little or no impact on rates of recurrence or death. Thus, MRI should not be used routinely in the workup of new breast cancers. • The argument for preoperative MRI The upper threshold amount of residual disease that can be eradicated by radiation therapy is not yet well established. There are as yet no MRI criteria for assessing the likelihood of standard treatment failure in individual patients with multifocal or multicentric disease, or with occult cancer in the contralateral breast. Although the rate of recurrence after breast conservation is low, it is not zero, and each patient should be offered the best possible chance for successful treatment. Detecting widespread disease can obviate inappropriate attempts at conservation, in which both lumpectomy with positive margins and re-excision with positive margins are carried out before the full extent of the disease burden is understood. Knowledge of the extent of disease at presentation will help the patient to make a more informed decision when presented with treatment options. A staging MRI examination showing only a single cancer lesion may permit the patient to choose conservation therapy with a high degree of confidence that no macroscopic disease will be missed at surgery. • Challenges for future clinical trials These issues will not be easy to resolve. Definitive answers can only come from controlled clinical trials with mortality as the end point, but for the data from these trials to be useful, the trials must use standardized MRI technique and interpretation criteria. Such standardization has yet to be accomplished. In the absence of such guidance, it seems reasonable to use MRI for staging within the known limitations of the technique and with secure histologic confirmation whenever widespread disease is suspected from the MRI findings. In this way, the patient and her surgeon can select a treatment plan based on the most realistic assessment of disease burden. References1.Comstock CE, Eby PR: 2nd Annual Great Debate: The Role of Breast MRI in Preoperative Staging. American Roentgen Ray Society Annual Meeting.Presented May 4, 2014. 2. Medscape Education Radiology:Breast Cancer Imaging: MRI’s Role in Current Practice: Gillian Newstead, MD 11/27/2012 Utility of Magnetic Resonance Imaging in the Management of Breast Cancer: Evidence for Improved Preoperative Staging 1. Laura Esserman, 2. Nola Hylton, 3. Leila Yassa, 4. John Barclay, 5. Steven Frankel and 6. Edward Sickles From the Departments of Surgery, Radiology, and Epidemiology and Biostatistics, University of California, San Francisco, San Francisco, CA 94143. Abstract PURPOSE: The staging and treatment for breast cancer are changing; there is an increase in the incidence of ductal carcinoma-in-situ, the use of fine-needle aspiration and stereotactic biopsy for diagnosis, and the use of neoadjuvant chemotherapy. Thus, there is a need for a tool to assess more precisely the extent of cancer in the breast before surgery. To better plan surgical and chemotherapeutic interventions, we evaluated high-resolution magnetic resonance imaging (MRI) as such a tool. PATIENTS AND METHODS: Fifty-seven patients with 58 cases of breast cancer were evaluated preoperatively with MRI using a technique called the triple-acquisition rapid gradient echo technique to maximize anatomic detail. Imaging results were compared with mammography and subsequent pathology results. RESULTS: Magnetic resonance imaging correctly identified residual or primary cancer in 55 of 58 cases and accurately predicted the extent of the cancer in 54 of 58 cases. The anatomic extent was more accurately defined with MRI compared with mammography (98% v 55%). Magnetic resonance imaging added the greatest value in cases of multifocal disease. CONCLUSION: By applying MRI selectively to patients with a known diagnosis of cancer and focusing on defining the extent of malignant lesions, we were able to obtain clear and accurate anatomic information. Our results suggest that MRI could provide very valuable information for preoperative planning and single-stage resection in breast cancer. Based on preliminary data from our series, MRI would be valuable as a staging tool in the preoperative setting even if the cost is in the range of $1,300 to $2,000. It is already significantly less than the target cost, so it is reasonable to refine this technique for clinical use to help plan the most appropriate surgical intervention and possibly reduce costs as well. A careful prospective study is warranted to validate our findings. Received March 19, 1997.Accepted September 1, 1998. In Summary: MRI FOR BREAST CANCER STAGING MRI is effective for staging the extent of disease following a biopsy diagnosis of cancer. In numerous studies, MRI has been shown to be superior to mammography and ultrasound for estimating tumor size when compared with histopathology. In a comparison of mammography, ultrasound and MRI using concordance with histopathology as the end point, Essermanet al32 found that MRI showed the greatest improvement over mammography and ultrasound for staging disease extent when multifocal disease or ductal carcinoma-in-situ (DCIS) was present. Information about the extent of disease is useful in determining suitability for breast conservative surgery and can be used to help guide breast conservation. However, in practice, it is difficult to translate the anatomic boundaries of the enhancing lesion seen on MRI to surgical coordinates with enough precision to ensure adequate margins while minimizing the amount of tissue excised. A criticism of MRI is that it is likely to result in more aggressive surgical approaches without necessarily improving outcomes. Occult multifocality suggested by MRI should be verified by biopsy before recommending substantial alteration to the surgical plan. Boetes C, Mus RD, Holland R, et al: Breast tumors: Comparative accuracy of MR imaging relative to mammography and US for demonstrating extent. Radiology 197:743-747, 1995 Soderstrom CE, Harms SE, Copit DS, et al: Three-dimensional RODEO breast MR imaging of lesions containing ductal carcinoma in situ. Radiology 201:427-432, 1996 Esserman L, Hylton N, Yassa L, et al: Utility of magnetic resonance imaging in the management of breast cancer: Evidence for improved preoperative staging. J ClinOncol 17:110-119, 1999