Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
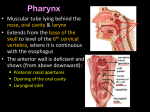
Pharynx Dr. Basil Saeed, Professor of otorhinolaryngology. Lecture 1 Anatomy The pharynx is a funnel-shaped fibromuscular tube lined with epithelium and is 10-12 cm in length in adults. It extends from the base of the skull superiorly to the level of C6 where it becomes continuous with the esophagus. The pharyngeal wall consists of 4 layers: 1. Mucous membrane. It is stratified squamous type, except in the nasopharynxnasopharynx where columnar ciliated epithelium is found. 2. Pharyngobasilar fascia. It is the middle fibrous tissue layer. 3. Muscle layer. It consists of three constrictor muscles- superior, middle and inferior- which overlap from below upwards. 4. Buccopharyngeal fascia. The pharynx is divided anatomically into 3 parts: 1- Nasopharynx: This extends from the base of the skull to the hard palate. It communicates anteriorly with the nasal cavities through the posterior nares (choanae). At the junction of the roof and posterior wall lies a small mass of lymphoid tissue called adenoids (nasopharyngeal tonsil). On the lateral wall, there are the openings of the Eustachian tubes. These tube connect the nasopharynx with the middle ear cavities, and are lined with ciliated columnar epithelium. Behind which are hollows called the fossa of Rosenmuller, which is the site of nasopharyngeal malignancy. 2- Oropharynx: This extends from the level of hard palate to the level of hyoid bone and opens anteriorly into the oral cavity. The palatine tonsils are situated in it's lateral wall. The free edge of the soft palate forms the palatine arch which separates the oral cavity from the pharynx. 3- Hypopharyx: This extends from the level of hyoid bone to the upper end of oesophagus and communicates anteriorly with the larynx and below with the oesophagus. It’s divided into 3 parts: a. Pyriform fossae: are two potential spaces on each side of the pharynx forming a lateral food channel during the act of swallowing. b. Postcricoid area: lies behind the cricoid cartilage and encircled by the cricopharyngeus muscle which forms the upper oesophageal sphincter. c. Posterior pharyngeal wall: extends from the hyoid bone to the oesophageal inlet. Mucous Membrane The lining epithelium is stratified squamous except in the nasopharynx, where columnar epithelium is found. Pharyngobasilar Fascia This fascia is strengthened posteriorly by a strong band called the median raphae. This raphae is attached above to the base of the skull and gives insertion to the constrictor muscles. Muscular Layer I- Circular (outer): which consist of 3 constrictor muscles overlapping one another from below upwards. 1 Superior constrictor: it arises from the medial pterygoid plate, pterygoid hamulus and pterygomandibular ligament. 2 Middle constrictor: it arises from the hyoid bone and stylohyoid ligament. It gives stability to the hypopharynx 3 Inferior constrictor: has 2 parts: a Thyropharyngeus (oblique) arises from the oblique line of thyroid cartilage. b Cricopharyngeus (transverse): arises from the cricoid cartilage and passes transversely backwards forming the upper oesophageal sphincter. All the constrictor muscles are inserted posteriorly into the median pharyngeal raphae. Functions: The constrictor muscles propel the bolus of food down into the esophagus. The cricopharygeus (lower fibers of the inferior constrictor) act as a sphincter, preventing the entry of air into the esophagus between the acts of swallowing Killian dehiscence: this is a potential gap between the fibers of the thyropharyngeus and cricopharyngeus. The mucous membrane may bulge between these two muscles when there is incoordination of the pharyngeal peristaltic waves and thus forming the pharyngeal pouch. II- Longitudinal (internal): these muscles elevate the larynx and shorten the pharynx during deglutition: Stylopharyngeus. ,Salpingopharyngeus and Palatopharyngeus. Buccopharyngeal Fascia This fascia is loosely attached posteriorly to the prevertebral fascia and laterally it's connected to the styloid process and to the carotid sheath. Subepithelial lymphoid tissue of the pharynx (Waldeyer's ring) Is a collection of sub-epithelial lymphoid tissue around the entrance of the respiratory and alimentary tracts. Waldeyer's ring is formed by: 1. Nasopharyngeal tonsil (adenoid): Lies between the roof and posterior wall of the nasopharynx. The free surface exhibits about 5 vertical fissures. 2. Tubal tonsils: lie behind the openings of the Eustachian tubes. 3. Palatine tonsils: are two masses of lymphoid tissue situated on each side of the oropharynx. 4. Lingual tonsils: which is embedded in the posterior 1/3 of the tongue. 5. Lateral pharyngeal bands behind the posterior tonsillar pillar. 6. Lymphoid nodules scattered on the posterior pharyngeal wall. Hypertrophy of the lymphoid tissue of Waldeyer's ring occurs in the earlier years of childhood, probably in response to upper respiratory tract infection. Maximum bulk is obtained at the age of 3-6 years, thereafter, some regression in size is to be expected, and in old age it atrophies. Waldeyer's ring is characterized by: 1. Lack a definite capsule. 2. They have efferent lymph vessels, but no afferent vessels. 3. Function as one unit: when a member of it is removed, the others parts undergo compensatory hypertrophy. 4. It has an immunological function like the formation of lymphocytes, and secretion of antibodies mainly lgA. Palatine Tonsils Are two masses of lymphoid tissue situated on each side of the oropharynx. The medial surface is exposed in the pharynx and is pitted by a number( dozen) of crypts which passes extend into the substance of tonsillar lymphoid tissue. The tonsil has an upper pole, body and a lower pole which extends into the dorsum of the tongue forming the lingual tonsil. The tonsil is related anteriorly and posteriorly to the palatoglossus and palatopharyngeus muscles respectively. Laterally the tonsil is enclosed by a dense fibrous capsule separating the tonsil from the superior constrictor muscle (tonsillar bed). This capsule provides a convenient plane of separation of the tonsil during tonsillectomy. * Blood supply of the tonsil: 1. The main supply is the tonsillar branch of the facial artery. 2. Lingual artery. 3. Ascending pharyngeal artery. 4. Descending palatine artery. The venous drainage is to the paratonsillar vein which drains to the pharyngeal plexus and into the internal jugular vein. * Lymphatic drainage: Deep cervical chain of lymph nodes. Nerve Supply of the Pharynx Sensory Nerve Supply Nasopharynx: Maxillary nerve( trigeminal). Oropharynx: Glossopharyngeal nerve, and trigeminal. Laryngopharynx: Internal laryngeal branch of the vagus nerve, and glossopharyngeal. Motor Nerve Supply All the muscles of pharynx, except the stylopharyngeus, are supplied by the pharyngeal plexus. The plexus is formed by the pharyngeal branches of the IX and X nerves together with the sympathetic fibers from the superior cervical ganglion. The stylopharyngeus is supplied by the glossopharyngeal nerve Retropharyngeal Space (Space of Gillette) This space lies behind the pharynx and extends from the base of the skull to the superior mediastinum. The anterior wall is formed by the posterior pharyngeal wall and it's covering buccopharyngeal fascia. The posterior wall is formed by the cervical vertebrae and their covering muscles and fascia. Contents: retropharyngeal lymph nodes of Rouviere. They usually disappear spontaneously during the 3rd or 4th year of life. Parapharyngeal Space This potential space lies lateral to the pharynx and connects posteriorly with the retropharyngeal space. It extends from the base of the skull to the hyoid bone. It is bounded medially by the superior constrictor muscle. Laterally lies the medial pterygoid muscle, the mandible and the parotid gland. It's posterior wall is the prevertebral muscles and fascia. Contents 1. Deep cervical lymph nodes. 2. The last 4 cranial nerves and the cervical sympathetic trunk. 3. Great vessels of the neck: carotid and internal jugular vein. Physiology of the pharynx The pharynx is the inlet for the air and food passages. Swallowing is divided into 3 stages : the oral stage, pharyngeal stage and the esophageal stage. Vocal resonance and articulation are important for speech production. It also has a protective function of the the lymphoid tissue of Waldeyer's ring . Symptoms of Pharyngeal Diseases 1- Sore throat (pain) a Inflammatory: Aphthus, tonsillitis and pharyngitits. b Neoplastic: Malignancy of oropharynx or hypopharynx. c Neurological: IX neuralgia. d Blood dyscrasia: Agranulocytosis and leukaemia. 2- Dysphagia: True dysphagia is the real difficulty in swallowing food, resulting in food coming back into the mouth, slow eating and loss of weight. It means the presence of cancerin the pharynxor esophagus until proved otherwise and is usually progressive. The second form is a feelimg of a lump in the throat and is usually due to cricopharyngeus spasm secondary to stress, reflux esophagitis, pharyngeal pouch, or pressure from a big thyroid or cervical osteophytes. It can be the earliest sign of cancer. The other form is painful swallowing (odynophagia), which can be due to tonsillar infection or pyriform sinus tumour. 3- Difficulty in breathing: Any pharyngeal infection is likely to impede the airway leading to stridor e.g. retropharyngeal abscess and Ludwig's angina. 4- Speech problems: Paralysis of the soft palate can lead to abnormal speech called rhinolalia aperta (hypernasalily). This is in contrary to rhinolalia clausa when there is nasal obstruction by anything like common cold or nasal polyps. Muffled voice can be seen on oropharyngeal and hypopharyngeal tumours of some size. 5- Neck mass, due to lymphadenpopathy: May be infective or malignant. 6- Other symptoms include regurgitation of recently eaten food in cases of pharyngeal pouch, and nasal symptoms such as epistaxis and nasal block in nasopharyngeal tumours. Such tumours can result in neurological symptoms resulting from cranial nerve involvement like diplopia and hoarseness. Examination 1- Nasopharynx: This can be done with postnasal mirror and tongue depressor (posterior rhinoscopy), and it can be thoroughly examined by rigid and flexible endoscopes. 2- Oropharynx: It is simple with tongue depressor; palpation may be needed for the tongue. 3- Hypopharynx: It can be done with the use of laryngeal mirror to examine the larynx too. It can be done thoroughly with the use of endoscope. 4- Neck examination: for cervical lymphadenopathy. 5- Other areas : ears are examined for secretory otitis media in cases of nasopharyngeal tumours. Investigations of pharyngeal diseases: 1- Radiography: Plain films like lateral X-Ray of the skull, is needed in nasopharyngeal mass like adenoids, and can demonstrate bone erosion in cases of nasopharyngeal cancer. Contrast films: barium swallow is needed in the diagnosis of pharyngeal pouch, esophageal web and hypopharyngeal mass. CT scan MRI scan. 2- Laboratory investigations: CBC, ESR, serum iron and iron binding capacity, monospot test, serology for toxoplasma, brucella, CMV and HIV. 3- Biopsy for suspected lesions in the pharynx may be needed.