Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
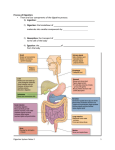
Questions on Digestion and Absorption 1. 2. 3. 4. 5. 6. Digestion of carbohydrates in diet. (3/4) Describe digestion of starch to glucose. (3/4) Describe with the help of a diagram how glucose is absorbed in the intestine. (3) Describe the absorption of glucose (3) Glucose absorption (3/4) Explain the mechanism involved in the absorption of glucose. Describe the causes and features of lactose intolerance. (3/4) 7. Explain how fructose, glucose and ribose are absorbed from the G.I tract. (3) 8. Lactose intolerance (3/4) 9. Write in brief about the digestion and absorption of proteins (3/4) 10. Describe the process of digestion and absorption of dietary proteins. (5) 11. Role of hydrochloric acid in protein digestion. (3) 12. Write in detail about the digestion and absorption of lipids. Write about causes of fatty stools. (5) 13. Give an account of the digestion of a triacylglycerol. (3/4) 14. Write a brief account on absorption of fat from gastrointestinal tract (3) 15. Functions of bile salts. (3) 16. Formation and disposal of chylomicrons. (3/4) 17. What is steatorrhoea? Mention two causes for steatorrhoea. (3) 18. Explain the biochemical basis: a) Oral insulin is not effective in treating diabetes mellitus. b) Steatorrhea is observed in chronic pancreatitis. (3) 19. Explain the biochemical basis: a) Denatured proteins are more easily digested. b) Steatorrhea in biliary obstruction (3) Digestion and Absorption of Food HPKedilaya,GaneshPrasad 2014……………………………………………………………………………... Note: Superscript number denotes ‘Reference for further details’ given in a box usually at the bottom of the page or end of the topic. This is less important for examinations. Contents: Biological Importance Medical Importance Digestion and Absorption – General Aspects Digestion and Absorption of Carbohydrates Digestion and Absorption of Proteins Digestion and Absorption of Fat Biological Importance Digestion is a chemical process wherein large molecules in the food are broken down to smaller molecules so that they can be absorbed. Food consists of large molecules which cannot be absorbed by the body as such and hence need to be digested. Food also consists of small molecules such as vitamins, minerals, monosaccharides and free amino acids which do not need digestion and can be absorbed as such. Absorption is transport of molecules, either digested products or other small molecules which do not require digestion, from the intestinal lumen into blood across the intestinal mucosal cells. 1 Medical Importance Lactose intolerance is a condition where intake of milk causes diarrhea and is due to deficiency of lactase, the enzyme required for digestion of lactose of milk. Hartnup’s disease is due to a genetic defect in the absorption of neutral amino acids, especially tryptophan. Steatorrhea is a condition where excess fat is excreted in feces and is seen in diseases of pancreas, biliary obstruction, etc. Chronic diarrhea can cause malabsorption as seen in celiac disease, Sprue, Crohn’s disease, etc. Digestion and Absorption – General Aspects Digestion The major foodstuffs that require digestion are carbohydrates, proteins and fat (triacylglycerol). During the process of digestion macromolecules are broken down to smaller molecules – polysaccharides to monosaccharides, proteins to amino acids and triacylglycerols (fats and oils) to glycerol and fatty acids. Digestion takes place in the aqueous medium of various digestive juices – Site of Digestion Digestive Juices Mouth Saliva Stomach Gastric juice Small intestinal lumen Pancreatic juice, Bile and Intestinal juice Digestion involves action of enzymes that are present in different digestive juices. All digestive enzymes are hydrolases that hydrolyze the anhydride linkages – glycosidic, peptide and ester linkages of carbohydrates, proteins and fats, respectively. Bile, synthesized in liver and entering into duodenum, neutralizes acidic stomach contents when it enters the duodenum providing optimum pH for enzymes in small intestinal lumen and helps in fat digestion (Bile salts, a constituent of bile, help in both digestion and absorption of fat.) During cooking, hydration of polysaccharides and denaturation of proteins take place. This helps digestion of these molecules. Mastication helps in breaking down of food particles and thus increases solubility and surface area for enzyme action. Peristalsis is also important in breaking down of food particles and mixing them with enzymes. Absorption The small intestine is the main absorptive organ. About 90% of the ingested foodstuffs are absorbed in the course of passage through the small intestine and water is absorbed at the same time. Considerably more water is absorbed after the foodstuff residues pass into the large intestine, so that the contents, which were fluid in the small intestine, gradually become more solid in the colon. 2 Absorption of substances into mucosal cells involves the passage across the plasma membrane either by – simple diffusion or carrier-mediated transports. – Simple diffusion is passive (no energy expenditure) and does not require carrier protein. – Carrier mediated transports may be facilitated transport (passive) or active transport (requiring energy expenditure) There are two pathways for the transport of materials absorbed by the intestine – 1) The hepatic portal system, which takes absorbed water-soluble nutrients directly to the liver 2) The lymphatic vessels, which takes absorbed lipid-soluble nutrients in the form of chylomicrons to the blood stream by way of thoracic duct Digestion and Absorption of Carbohydrates Contents: Introduction Digestion of Starch (and glycogen) Digestion of Disaccharides Absorption of Carbohydrates Clinical Significance Introduction The major carbohydrates in the diet are: Monosaccharides – mainly fructose (present in fruits) Disaccharides – sucrose, lactose and small amounts of maltose (present in malt, beer) Polysaccharides – starch and dietary fibers Starch forms more than 50% of carbohydrates in human food. (Dietary fibers – cellulose, hemicellulose, pectin, lignins, etc. are indigestible. For ‘Dietary fibers’, see Chapters – ‘Chemistry of Carbohydrates’ and ‘Nutrition’) Human food also contains small amounts of pentoses, glucose, trehalose (disaccharide present in mushroom), and glycogen (present in liver in animal foods). All enzymes of carbohydrate digestion cleave glycosidic bonds by hydrolysis. Disaccharides and polysaccharides are digested to their respective constituent monosaccharides units and absorbed in the small intestines along with free monosaccharides present in the food. The absorbed monosaccharides enter the hepatic portal circulation and then to liver cells. Part of the absorbed monosaccharides that is not taken up by hepatic cells enters the systemic circulation. DIGESTION ABSORPTION (in the Small Intestine) Fructose Fructose Sucrose FOOD Starch Glucose 3 Lactose Galactose Digestion of Starch 1, 2 Starch on complete digestion yields glucose. Digestion of starch takes place in mouth, small intestinal lumen and the small intestinal brush border (luminal surface of intestinal mucosal cells). Enzymes required for complete digestion of starch are – amylase (salivary and pancreatic amylase), maltase and isomaltase. Amylase and maltase cleave -1,4 glycosidic linkages and isomaltase cleaves -1,6 glycosidic linkages of starch. (Amylase hydrolyzes internal -1,4 glycosidic linkages.) Starch is mainly digested by pancreatic amylase. Contribution by salivary amylase is very little since the food remains in the mouth for a very short period of time and the enzyme is inactivated by gastric HCl as it enters stomach. Maltase and isomaltase are present on the luminal surface of small intestinal epithelial cells (brush border cells). Starch (amylose and amylopectin) Salivary amylase (in mouth)3 Or Pancreatic amylase (in small intestinal lumen) Limit dextrins4 Small unbranched oligosaccharides (e.g., Maltose, Maltotriose, etc) Isomaltase Maltase Maltase (brush border cells) Glucose Isomaltose Isomaltase (brush border cells) Reference 1. The enzymes and the steps of digestion of glycogen are same as those of amylopectin component of starch as both have similar structure. 2. Cooking hydrates the starch granules making it more susceptible to digestion. 3. Salivary amylase (ptyalin) is present in saliva. Cl- is an activator of this enzyme. 4. Limit dextrins are derived from amylopectin component by the action of amylase and contain eight glucosyl units with one or two branches with α-1,6-glycosidic bonds. 4 Digestion of Disaccharides – – – Major disaccharides present in the human diet are – sucrose and lactose. Small amounts of free maltose (present in malt, beer) and trehalose (disaccharide present in mushroom) may also be present. However, quantitatively maltose is the major disaccharide digested in the gut. Most of the maltose in the gut is derived from digestion of starch. Isomaltose is another disaccharide derived from starch and is digested by isomaltase. (See ‘Digestion of Starch’). Site of digestion of disaccharides is the small intestinal brush border. Maltose, sucrose, lactose and trehalose are digested (hydrolyzed) by disaccharidases – maltase, sucrase (also called invertase), lactase and trehalase respectively. Disaccharidases are attached to the surface of the small intestinal brush border cells. (For ‘digestion of maltose’, see ‘Digestion of Starch’.) – – – – Sucrase Sucrose glucose + fructose Lactase Lactose glucose + galactose Trehalase Trehalose 2 glucose Maltase Maltose 2 glucose Isomaltase Isomaltose 2 glucose Absorption of Monosaccharides The major monosaccharides resulting from carbohydrate digestion are D-glucose, Dgalactose and D-fructose. Absorption is carrier mediated. Pentoses are absorbed by simple diffusion. Monosaccharides are first transported from the lumen to the small intestinal epithelial cells and then into capillaries of portal venous system. Absorption of Glucose Glucose is absorbed from the small intestinal lumen into the intestinal epithelial cells by carrier mediated mechanism involving transporter proteins situated on the luminal surface of the intestinal epithelial cells. Glucose is absorbed mainly by 1) Na+-dependent transporter by secondary active transport and to a less extent by 2) Na+-independent transporter by passive transport. 1) Na+-dependent transporter (SGLT) 5 This carrier protein carries glucose or galactose along with sodium ion from the lumen. The driving force for the Na+-dependent transport is derived from the maintenance of low intracellular levels of Na+ by the action of the Na+-K+ATPase (secondary active transport). 2) Na+-independent transporter Small amounts of glucose, is transported by facilitated transport utilizing glucose transporter-5 (GLUT-5). Transport of glucose from cells to portal venous capillaries: Glucose is transported from the intestinal epithelial cells into portal venous capillaries by glucose transporter-2 (GLUT-2). It is a uniport facilitated transport system, which is sodium independent. Intestinal Lumen Glucose Intestinal Epithelial Cell Na Na+-dependent transporter (SGLT) GLUT-5 Glucose + Na+ K+ ATP ADP + Pi Na+ K+ Na+–K+ ATPase Glucose GLUT-2 Portal Capillary Blood Figure: Absorption of Glucose Absorption of Other Monosaccharides Fructose is absorbed from small intestinal lumen into mucosal cells by facilitated transporter GLUT-5, sharing with glucose. Galactose is absorbed by Na+-dependant trasporter (SGLT) sharing with glucose. Both fructose and galactose are transported from the intestinal epithelial cells into portal venous capillaries by glucose transporter-2 (GLUT-2), sharing with glucose. Any pentose present in food is absorbed by simple diffusion. Clinical Significance Lactose Intolerance 6 This is a common condition with gastrointestinal symptoms like diarrhea, abdominal cramps and flatulence after ingestion of milk or milk-based foods. Cause is due to deficiency of lactase5. Deficiency may be due to genetic (primary/inherited) or acquired (secondary to other causes). The reason for acquired lactose intolerance may be the damage to intestinal epithelial cells due to colitis, gastroenteritis, alcohol consumption or sudden change into a milk-based diet. Biochemical basis of clinical manifestation: Lactase deficiency Accumulation of lactose, organic acids and gases (CO2 and H2) (Produced by action of bacteria on lactose in the gut) Osmotic movement of water from the intestines to the lumen Flatulence and abdominal cramps Diarrhea Treatment involves avoiding milk. Curd is an effective treatment, because the lactobacilli present in curd contains the enzyme lactase. Reference 5. If the lactase enzyme is defective at birth then this constitutes early onset lactose intolerance (inherited lactase deficiency). A significant number of adults exhibit late onset lactase deficiency (primary low lactase activity) especially Asian-, Native- and African-Americans. Digestion and Absorption of Proteins Contents: Digestion of protein – general aspects Reactions of protein digestion Absorption of amino acids Clinical significance Digestion of Proteins – General Aspects Contents: – – – – – – Introduction Sites of protein digestion, GIT juices and proteases Endopeptidases and exopeptidases Specificity of proteases Proteases -zymogen form and activation Role of HCl in protein digestion Introduction 7 Digestion of dietary proteins involves hydrolysis of peptide bonds catalyzed by a group of enzymes called proteases or peptidases in the gastrointestinal tract Complete digestion of proteins yields amino acids. Dietary proteins are denatured on cooking and therefore, cooked proteins are more easily digested1. Sites of Protein Digestion, GIT Juices and Proteases Protein digestion takes place in stomach and intestinal lumen. Enzymes of protein digestion are secreted in gastric juice, pancreatic juice and intestinal juice. GIT Juices Proteases Present Gastric juice Pepsin (chief cells of stomach), Rennin2 Pancreatic Juice Trypsin, Chymotrypsin, Elastase. Carboxypeptidases Intestinal Juice Aminopeptidases, Dipeptidases Endopeptidases and Exopeptidases - Carboxypeptidases and aminopeptidases are exopeptidases – hydrolyze terminal bond releasing one amino acid at a time. Carboxypeptidases act at the carboxy terminal and aminopeptidases at the amino terminal of the protein chain. - Pepsin, trypsin, chymotrypsin, etc are endopeptidases – hydrolyze peptide bonds in the interior of the protein chain to cleave the protein molecule into more than one smaller polypeptides and peptides. Specificity of Proteases Endopeptidases hydrolyze specific peptide bonds in protein molecules. Specificity differs from one protease to another3. Proteases – Zymogen Form and Its Activation Proteolytic enzymes are secreted as inactive zymogens/proenzymes, which are converted to their active form in the intestinal lumen4. Reference 1. During the process of denaturation unfolding of protein molecule takes place and thus peptide bonds become more accessible for the enzyme action. 2. Rennin, a protease, is active in infants and is involved in curdling of milk. Rennin denatures casein of milk to paracasein irreversibly, which then is acted upon by pepsin. Rennin is reported to be absent in the stomach of adults. 3. Enzyme Hydrolysis of petide bonds formed by carboxyl groups of Pepsin Trypsin Chymotrypsin Phe, Tyr, Trp, Met Arg, Lys (basic amino acids) Phe, Tyr, Trp, Val, Leu (Aromatic, uncharged amino 8 Acids) Ala, Gly, Ser (small amino acid residues) Elastase 4. Activation of enzymes involves the cleavage of small peptides so that the active sites are exposed. This would prevent auto-digestion of the secretory acini. Active Enzyme - Inactive Zymogen Pepsin Pepsinogen Trypsin Chymotrypsin Trypsinogen Chymotrypsinogen Elastase Proelastase Carboxypeptidase Procarboxypeptidase Pepsinogen is activated to pepsin in the stomach first by HCl, secreted by parietal cells of stomach and then by pepsin itself (autoactivation). HCl Pepsinogen Pepsin Autoactivation - Trypsinogen is activated to trypsin in the small intestine first by enterokinase (a protease present on the intestinal mucosal membranes) and then by trypsin itself (autoactivation). Enterokinase Trypsinogen - Trypsin Trypsin also catalyses the activation of chymotrypsinogen, proelastase and procarboxypeptidases to chymotrypsin, elastase and carboxypeptidases, respectively. Trypsin Chymotrypsinogen Chymotrypsin Proelastase Elastase Procarboxypeptidase Carboxypeptidase Role of HCl in Protein Digestion The role of HCl, secreted by gastric parietal cells, in protein digestion are - 1) activation of pepsinogen 2) denatures the proteins and 3) providing optimum pH (pH 2 to 3) for the action of pepsin. (HCl also kills microorganisms present in food). 9 Reactions of Protein Digestion (In Stomach and Small Intestinal Lumen) Dietary Proteins In Stomach Pepsin, HCl Gastric Juice Proteoses + Peptones (polypeptides and smaller polypeptides) Trypsin In Small Intestinal Lumen Chymotrypsin Pancreatic Juice Elastase Small Polypeptides + Peptides Carboxypeptidases Pancreatic Juice In Small Intestinal Lumen Aminopeptidases Dipeptidases Intestinal Juice Amino acids Absorption of Amino Acids Amino acids, the end products of protein digestion, are rapidly absorbed from the intestine into the portal blood. Amino acids are transported by a number of carriers many by secondary active transport –Na+-dependent carriers similar to glucose transporter system. Different Na+ -dependent carriers are: - Neutral amino acid carrier - Phenylalanine and methionine carrier - Carrier specific for imino acids (proline and hydroxy proline) There are also Na+-independent carriers specializing in the transport of - Neutral and lipophilic amino acids (e.g. Phe, Leu) - Cationic amino acids (e.g. Lys) Clinical Significance - Allergy to certain food proteins (milk, fish) is believed to result from absorption of partially digested proteins. - Defect in non-tropical sprue is located within the mucosal cells of the intestine and permits the polypeptides (resulting from the peptic and tryptic digestion of gluten, the principal protein of wheat) to be absorbed into the circulation and thus elicit the production of antibodies. - Defect in the intestinal amino acid transport systems are seen in Hartnup’s disease, [defect in intestinal neutral amino acid (Trp) carrier], Iminoglycinuria, cystinuria etc. 10 - Acute pancreatitis (acute inflammation of pancreas), a life threatening disorder, is caused by autodigestion of pancreas by its proteolytic enzymes. Autodigestion is due to unusual conversion of proenzymes into active enzymes by trypsin. Digestion and Absorption of Lipids Contents: – – – – – Introduction Digestion of fat Digestion of other lipids Absorption of lipids Clinical significance Introduction – More than 90% of the dietary lipids are fats and oil (triacylglycerols). The rest is mainly made up of cholesterol and phospholipids. – The main site of digestion and absorption of lipids is the small intestinal lumen. – Bile salts help both in digestion of fat and absorption of digested products of lipids. – Heat of the stomach is important in liquidizing the dietary lipids. Digestion of Fat (Triacylglycerols) – Small intestinal lumen is the main site of digestion of fat. – Digestion of fat involves hydrolysis of ester bonds, produces fatty acids, glycerol and monoacyl glycerols (MAGs) and is catalyzed by lipases. – Pancreatic lipase, present in the pancreas is the main enzyme for digestion of most of the fat. – Colipase, a protein secreted by pancreas, acts as cofactor for pancreatic lipase. – There are also other lipases – lingual lipase, gastric lipase and intestinal lipase – but their contribution is negligible. – Bile salts, present in bile, help fat digestion by emulsifying fat. Role of Bile Salts in Fat Digestion – The bile salts present in the bile lower the surface tension and emulsify fat in the intestine. – Intestinal peristalsis also helps in this. – Emulsification increases the surface area of the fat droplets enabling more enzyme (lipase) molecules to act and thus speeding up digestion. 11 Reactions of Digestion of Fat (Triacylglycerol)1 Triacylglycerol (Fat) Lipase Pancreatic Juice Colipase Fatty Acid Diacylglycerol (DAG) Lipase Colipase Fatty Acid Monoacylglycerol (MAG) Lipase Colipase Fatty Acid Glycerol The major end products of the digestion of fat are – – monoacylglycerols (MAGs), – glycerol and – fatty acids Digestion of Other Lipids – Pancreatic secretion also contains cholesterol esterase and phospholipase A2. – Cholesterol esterase hydrolyzes cholesterol ester to cholesterol and fatty acid. – Phospholipase A2 hydrolyzes phospholipids to form lysophospholipid and a fatty acid. Absorption of Digested Products of Lipids – The water soluble products of lipid digestion – glycerol as well as small- and mediumchain fatty acids (chain length less than 12 carbons) are directly absorbed from the intestinal lumen in to the portal vein and taken to the liver Reference 12 1. Digestion of fat requires another enzyme also an isomerase, which isomerizes 2-MAG into 1-MAG, as lipase cannot hydrolyze 2-MAG. – The more water-insoluble products – monoacylglycerols, long-chain fatty acids, cholesterol and lysophospholipids – are incorporated into bile salt micelles2 to form mixed micelles. – These mixed micelles fuse with the cell membrane of intestinal mucosal cells whereby the products of lipid digestion are internalized into the mucosal cells3. – Triacylglycerols are reconstituted in the intestinal mucosal cells and incorporated into chylomicrons (a lipoprotein) along with apolipoproteins, cholesterol, phospholipids and fat-soluble vitamins absorbed from the intestine. – The chylomicrons are collected by the lymphatic vessels that lead to the blood stream by the way of thoracic duct4. – Normally Over 98% of the dietary lipid is absorbed. . Reference 2. – Bile salt and lecithin (a phospholipid) that are present in bile are amphipathic and hence form micellar aggregation. – The micelles are spherical particles with a hydrophilic exterior and hydrophobic interior core. 3. – The bile salts are left behind which are mostly reabsorbed from the ileum and returned to the liver to be excreted back to the bile (enterohepatic circulation). 4. – The chyle (milky fluid) from the intestinal mucosal cells loaded with chylomicron are transported through the lymphatic lacteals into the thoracic duct and then emptied into systemic circulation. – The serum may appear milky after a high fat meal (post-prandial lipemia) due to the presence of chylomicron in circulation. Normally the lipemia clears within a few hours by the uptake of chylomicron by tissues. 13 Absorption of Digested Products of Lipids Digested Products of Lipids Water-insoluble Monoacylglycerols Long-chain fatty acids Cholesterol Water-soluble Glycerol Short- and Medium-chain fatty acids Micelles Fat-soluble vitamins Mixed micelles SMALL INTESTINAL LUMEN Intestinal Epithelial Cell Monoacylglycerols Long-chain fatty acids Cholesterol Fat-soluble vitamins Triacylglycerol Phospholipids Apolipoproteins Chylomicron Chylomicron LYMPHATIC VESSELS Glycerol PORTAL BLOOD Short- and Medium- chain fatty acids Clinical Significance Steatorrhea - When daily excretion of fat in feces is more than 6g per day, the condition is called steatorrhea. - It may be due to defective digestion or defective absorption of fat. - Defective digestion of fat may be due to absence of or deficiency of pancreatic lipase as in chronic diseases of pancreas or surgical removal of pancreas. - Defective absorption of fat occurs when bile salts do not enter the intestine as in biliary obstruction (e.g. due to biliary stone) - Defective absorption may also be due to malabsorptive diseases e.g. celiac disease, Sprue, Chrohn’s disease, etc or surgical removal of large lengths of the intestine. Chyluria and Chylothorax5 Reference 14 5. Chyluria is an abnormality in which patient excretes milky urine because of the presence of an abnormal connection between the urinary tract and the lymphatic drainage system of the intestine, a so-called chylous fistula. In a similar abnormality – chylothorax, there is an abnormal connection between the pleural space and the lymphatic drainage of the small intestine that results in the accumulation of milky pleural fluid. 15