Survey
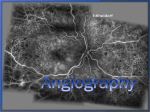
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Reference Section Magnetic Resonance Angiography Using the Intravascular Contrast Agent Vasovist ® a report by Mathias Goyen University Medical Centre Hamburg Atherosclerosis is a generalised disease and contributes to cardiac death, stroke, limb loss and a range of other illnesses. Disease in the major arteries, including the infra-renal abdominal aorta, internal iliac arteries, renal arteries and peripheral vasculature, remains a major cause of morbidity and mortality. For example, the prevalence of disease in the infrarenal abdominal aorta ranges from less than 3% in 60year-old patients to 20% in 75-year-old patients,1,2 and the incidence increases with increasing age. Other forms of vascular disease such as renal artery stenosis present additional manifestations, including hypertension and renal failure. As the average age of the population increases, the burden of vascular disease is anticipated to increase. Until recently, X-ray angiography (XRA) requiring arterial catheterisation and the use of substantial volumes of iodinated contrast agent was the clinical standard practice when a detailed image of the vasculature was required. However, less invasive imaging techniques using X-ray computed tomography (CT) or magnetic resonance imaging (MRI) have been developed. These imaging methods, either without exogenous contrast agents (MRI only) or with exogenous contrast agents (both CT and MRI) have become increasingly popular over the past few years as data have suggested that their accuracy, in some clinical settings, might approach that of the accepted standard diagnostic method, catheter XRA using iodinated dye.3–5 MRI is a safe, non-invasive and widely available imaging technique that has experienced rapid growth over the past decade. Enhancement of MR images with exogenous contrast agents such as chelates of gadolinium or iron has become standard clinical practice in many settings. Such contrast agents provide technical benefits, including improved image quality, and clinical benefits, such as improved sensitivity and specificity for disease. Magnetic resonance angiography (MRA), a more recent development in MRI, uses tailored acquisition sequences to highlight blood flow and is widely used to assist in the management of patients with vascular diseases, especially in the brain. In many vascular EUROPEAN CARDIOVASCULAR DISEASE 2006 beds like peripheral vessels, however, non-contrast MRA is not used routinely in clinical practice due to shortcomings of unenhanced MRA and/or the limitations of currently available MR contrast agents. What is Vasovist®? MS-325 is the product development code for the drug product containing trisodium gadolinium (international non-proprietary name: gadofosveset) as the active substance. Vasovist® injection is composed of an aqueous solution (244mg/ml, 0.25mmol/litre) of drug substance, gadofosveset trisodium, and a small amount of ligand excipient, fosveset, to ensure minimal free gadolinium in solution. The drug substance consists of a stable gadolinium diethylenetriaminepentaacetic acid (Gd-DTPA) chelate substituted with a diphenylcyclohexylphosphate group. Vasovist ® injection is a clear, colourless to slightly yellow solution in which the pH has been adjusted from 6.5 to 8.0. The density is 1.12g/ml and the osmolality ranges from 700–950mOsm/Kg at 37ºC. The viscosity of Vasovist® injection ranges from 2.7 to 3.3cps at 20ºC. The molecular formula is C33H40GdN3Na3O15P and the molecular weight for the anhydrous form is 957.86. Mathias Goyen is Chief Communication Officer (CCO) at the University Medical Center in Hamburg, Germany. He was previously Assistant Professor of Radiology at the Department of Diagnostic and Interventional Radiology at the University Hospital Essen, Germany. Dr Goyen has edited four books and authored many peer-reviewed articles in the field of magnetic resonance angiography. He completed his medical studies in Bochum, Germany and Basel, Switzerland and his residency training in radiology at the University Hospital Essen, Germany Vasovist® is administered either by a hand or power injector to deliver a dose of 0.03mmol/kg in 25–30 seconds. Overview of the Clinical Development Programme Prior to approval in the EU, Vasovist® underwent extensive evaluation of the safety and efficacy of the drug. The clinical development programme for efficacy included two phase II studies and four phase III studies. In phase II studies, approximately 300 patients were evaluated to define optimal dose for MRA. The optimal dose for MRA was found to be 0.03mmol/kg. The clinical effectiveness of Vasovist® was demonstrated through analysis of efficacy data of 672 patients who were included in four adequate and well-controlled phase III studies. Vascular beds 1 Reference Section Figure 1: Vasovist ®-enhanced f-p 3D-CE-MRA of the Carotid and Calf Arteries with 1mm 3 Isotropic Voxel Sizes intravenous bolus injection. The overall rate and experience of adverse events was comparable with placebo and was similar to that reported in clinical trials for other Gd chelates. Clinical Applications of Vasovist®-enhanced MR Angiography Due to the use of parallel acquisition techniques with an acceleration factor of three, scan time is only 12 seconds for the carotids. Due to the high relaxivity of the contrast agents, high vessel-to-background contrast is achieved despite the small contrast media volume of less than 8ml and the reduction of signal-to-noise ratio by PAT acceleration. Source: Stefan O Schoenberg, Department of Clinical Radiology, University Hospitals – Grosshadern, Munich, Germany. representative of areas of turbulent blood flow (aortoiliac occlusive disease) to an organ (renal artery disease) and slow flow (pedal arterial disease) were studied. In all of these studies, the fundamental methodology was the same. Summary of Efficacy Results of Four Phase III Studies Vasovist® reduced the rate of uninterpretability significantly and improved the diagnostic confidence. Fewer than 2.3% were uninterpretable for Vasovist®enhanced MR angiography, versus approximately 16% for two-dimensional time of flight. For comparison, 2.8% of the vessels were deemed uninterpretable on XRA. For all readers in all studies, the vascular surgeon readers agreed with XRA more often when using Vasovist®-enhanced MRA than when using pre-contrast MRA (range of improvements: 1–36%). For six of the eight readers, the improvement was substantial (>15%) and statistically significant (p<0.001). Safety Data for Vasovist® Safety data in 767 patients (505 males and 262 females) receiving 0.03mmol/kg bw dose are reported. There were no clinically significant trends found in adverse events, laboratory assays, vital signs, ECG, or oxygen saturation. Vasovist® has a good safety profile and can be safely administered as an 2 Diagnostic accuracy of 3-D contrast-enhanced MR angiography (3D-CE-MRA) is a result of temporal and spatial resolution, anatomic coverage and acquisition time. For first-pass 3D-CE-MRA (f-p 3D-CE-MRA) with standard extracellular Gdchelates this relationship is in conflict with the transit time of the contrast agent and the breath hold capacity of the patient. Representative clinical examples are the assessment of carotid, renal and peripheral arteries. In all three vessel territories maximum spatial resolution is required for exact detection and grading of atherosclerotic stenoses. For the carotid arteries, the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria require accurate definition of a 70% stenosis as a threshold for surgical endatherectomy. With regard to the renal arteries, a large multicentre study has shown relatively moderate results for stenosis grading if voxel sizes greater than 3mm3 were used for f-p 3D-CE-MRA while a recent study has shown good correlation to digital subtraction angiography using isotropic voxel sizes of less than 1mm3 and non-intravascular Gdchelates.8,9 The same study could also demonstrate that cross-sectional measurements of area stenosis are feasible if sufficient spatial resolution is used.9 On the other hand, high temporal resolution is also desirable for f-p 3D-CE-MRA for a number of reasons – in the carotid artery, delayed inflow and collateral flow can be visualised in the case of a haemodynamically significant stenosis, whereas retrograde flow can be appreciated in subclavian steal syndrome. For the renal arteries, disturbing overlay of enhancing renal parenchyma on small intrarenal branches can be effectively avoided allowing better visualisation of diseases involving the distal renal arteries, such as in fibromuscular dysplasia.10 For the peripheral arteries, critical ischaemia with inflammatory changes often results in substantial venous overlay prior to sufficient arterial enhancement. Here, the so-called hybrid approach often represents the only way to overcome this diagnostic limitation.11 This includes either a selective high-resolution f-p 3D-CE-MRA of the calves after a test-bolus measurement or a timeresolved f-p 3D-CE-MRA preceding the moving table-MRA of the pelvis and thighs.11 Any technical development overcoming this limitation of multiple measurements with different demands for temporal and spatial resolution would EUROPEAN CARDIOVASCULAR DISEASE 2006 Magnetic Resonance Angiography Using the Intravascular Contrast Agent Vasovist ® Figure 2: High-resolution Pulmonary MR Angiogram Acquired in the Steady-state Phase after Application of Vasovist ® a reasonable scan time of approximately 5 minutes.12 Due to the absence of motion artefacts in the peripheral arteries, exquisite image quality can be achieved allowing for visual artery–vein separation despite the close proximity of theses vessels. Artery–vein separation can be further enhanced by the use of semi-automated software, which is currently under preparation by different vendors. The add-on of the high-resolution s-s 3D-CE-MRA represents a valuable problem-solving tool in combination with the imaging during first pass. While the acquisition scheme of f-p 3D-CE-MRA can be adapted to meet the requirements for fast time-resolved imaging, the target area of interest is revisited during the s-s 3D-CE-MRA and imaged with maximum resolution. Other Potential Indications – Off-label Use be desirable. Intravascular contrast agents such as Vasovist® that are both bolus-applicable and remain in the vessels in the steady state have the potential to integrate these different diagnostic requirements within one single comprehensive scan. A recent study has shown that high-resolution f-p 3D-CEMRA with Vasovist® allows data sets to be acquired with an isotropic spatial resolution of 1mm3 in the carotid arteries with acquisition times of only 12 seconds.12 These acquisitions were accelerated by the use of parallel acquisition techniques (PAT) with acceleration factors of up to three. While PAT allow for higher spatial resolution at no increase in scan time, they decrease the signal-to-noise ratio at least by the square root of the acceleration factor. Thus, MR contrast agents with high relaxivity are required. Due to the strong protein binding, the relaxivity of Vasovist® is relatively high resulting in good image quality for f-p 3D-CE-MRA even for small total volumes, despite higher acceleration of acquisition by PAT. Figure 1 shows an example of f-p 3D-CEMRA of the carotid and calf arteries. In addition to the use of this combined firstpass/steady-state approach for the labelled indications, one can envision further applications beyond one single field of view. With the introduction of whole-body MRI scanners with multiple independent rf-channels and inbuilt coil systems for large anatomic coverage this approach becomes attractive for assessment of the entire vasculature by a combination of multi-station f-p 3D-CE-MRA and s-s 3D-CE-MRA. This shifts the focus of MRA away from solely displaying vascular anatomy to a more disease-specific imaging approach. One example includes the systemic assessment of atherosclerotic disease, which has been shown as an arising application for screening of cardiovascular risk factors in preliminary studies.13,14 This systemic angiographic assessment is also of high interest for patients with vasculitis such as Takayasu arteritis that manifests in multiple different locations. Here, the combination of f-p 3D-CE-MRA of the carotid and renal arteries in combination with high-resolution assessment of the inflammatory stenoses could improve the overall diagnostic work-up of the patients and replace a more time-intensive multistep multi-modality approach. After acquisition of MRA images in the first pass, any of the three vessel territories can easily be revisited for high-resolution 3D-CE-MRA in the steady-state phase (s-s 3D-CE-MRA). Initially, there were concerns with regard to the presence of venous overlay on the s-s 3D-CE-MRA data sets, particularly for arteries with small vessel calibre and close-by coursing veins such as in the distal calves. However, with today’s optimised surface coils and the use of PAT, isotropic voxel sizes of less than 100µm3 can now be acquired in Lastly, intravascular contrast agents enable the combined systemic assessment of arteries and veins, which is of particular interest for detection of lowerleg venous thrombosis complicated by pulmonary embolism.15 Figure 2 shows a high-resolution s-s 3DCE-MRA of the pulmonary vascular bed, acquired in one breath hold of approximately 35 seconds at a spatial resolution of 1mm3 using a PAT acceleration factor of three. In the steady state, it also would be feasible to use two sagittally-oriented 3-D slabs, each An acceleration factor of three was used for parallel imaging resulting in an overall scan time of 35 seconds for the entire data set with 1mm3 isotropic spatial resolution. Source: Stefan O Schoenberg, Department of Clinical Radiology, University Hospitals – Grosshadern, Munich, Germany. EUROPEAN CARDIOVASCULAR DISEASE 2006 3 Reference Section covering one lung separately, for further reduction of scan time without sacrificing spatial resolution.16 Conclusion Vasovist®-enhanced MRA is safe and well-tolerated in patients with vascular disease, effective for the detection of vascular stenosis and aneurysms, significantly more accurate – both more sensitive and specific – than non-contrast MRA for the diagnosis of vascular stenoses and similar to conventional angiography for the overall characterisation of vascular disease, without the need for catheterisation. ■ References 1. Criqui M H et al., “The prevalence of peripheral arterial disease in a defined population”, Circulation (1985);71: pp. 510–515. 2. Vogt M T et al., “Lower extremity arterial disease and the aging process: a review”, J Clin Epidemiol (1992);45: pp. 529–542. 3. Rieker O et al., “CT angiography versus intraarterial digital subtraction angiography for assessment of aortoiliac occlusive disease”, AJR Am J Roentgenol (1997);169: pp. 1,133–1,138. 4. Tan K T et al., “Magnetic resonance angiography for the diagnosis of renal artery stenosis: a meta-analysis”, Clin Radiol (2002);57: pp. 617–624. 5. Grist T, “MRA of the abdominal aorta and lower extremities”, J Magn Reson Imaging (2000);11: pp. 32–43. 6. Rapp J H, Wolff S D, Quinn S F et al., “Aortoiliac occlusive disease in patients with known or suspected peripheral vascular disease: safety and efficacy of gadofosveset-enhanced MR angiography—multicenter comparative phase III study”, Radiology (2005);236: pp. 71–78. 7. Goyen M, Edelman M, Perreault P et al., “ MR angiography of aortoiliac occlusive disease: a phase III study of the safety and effectiveness of the blood-pool contrast agent MS-325”, Radiology (2005);236: pp. 825–833. 8. Vasbinder G B et al., “Accuracy of computed tomographic angiography and magnetic resonance angiography for diagnosing renal artery stenosis”, Ann Intern Med (2004);141: pp. 674–682. 9. Schoenberg S O, Rieger J R, Weber C H et al., “High-spatial-resolution MR-angiography of renal arteries with integrated parallel acquisitions: comparison with digital subtraction angiography and US”, Radiology (2005);236: pp. 687–698. 10. Schoenberg S O et al., “Renal arteries: optimization of three-dimensional gadolinium-enhanced MR angiography with bolus-timing-independent fast multiphase acquisition in a single breath hold”, Radiology (1999);211: pp. 667–679. 11. Meissner O A, Rieger J, Weber C et al., “Critical limb ischaemia: hybrid-MR angiography compared with DSA”, Radiology (2005);235: pp. 308–318. 12. Nikolaou K, Schoenberg S O, Hartmann M, Chamberlin P, Reiser M F, “Ultra-high-resolution whole-body MRA using parallel imaging on a 32-channel MR system and intravascular contrast agents: protocol optimization for clinical applications”, Eur Radiol (2005); (Suppl): p. 340. 13. Herborn C U et al., “Peripheral vasculature: whole-body MR angiography with midfemoral venous compression—initial experience”, Radiology (2004);230: pp. 872–878. 14. Kramer H, Schoenberg S O, Nikolaou K et al., “Cardiovascular screening with parallel imaging techniques and a wholebody MR imager”, Radiology (2005);236: pp. 300–310. 15. Ruehm SG et al., “Pelvic and lower extremity veins: contrast-enhanced three-dimensional MR venography with a dedicated vascular coil-initial experience”, Radiology (2000);215: pp. 421–427. 16. Oudkerk M et al., “Comparison of contrast-enhanced magnetic resonance angiography and conventional pulmonary angiography for the diagnosis of pulmonary embolism: a prospective study”, Lancet (2002);359: pp. 1,643–1,647. 4 EUROPEAN CARDIOVASCULAR DISEASE 2006