Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
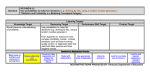
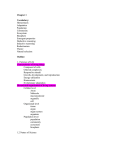
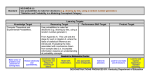
9/3/2014 Story.. • Take home message—clinical reasoning is the glue in OMPT learning Shaping Clinical Reasoning: A Collaborative Approach Using Varied Case Reports and Vignettes for Entry-level and Fellowship Students. Carina D Lowry and Carol A Courtney Objectives Clinical Reasoning • By the end of this presentation, the learner will: • Describe metacognition and explain techniques that the student can use to develop metacognition. • Explain several ways to incorporate clinical reasoning case reports into entry level and fellowship curricula. • Describe how videotape and interactive learning platforms can be utilized to give feedback on clinical reasoning processes. • Recognize the role of clinical instructor, clinical faculty, and small group facilitators in guiding clinical reasoning. • Identify pitfalls and errors in student reasoning and what to do to ensure a helpful learning environment. • Clinical Reasoning: thinking and decision making associated with clinical practice that enables therapists to take the best-judged action for individual patients • Hypothetico-deductive: Hypothesis testing for diagnosis/management • Pattern recognition: Associate current problem with pattern for management • Narrative: Collaborative reasoning between patient and clinician for management Jones and Rivett, 2004 Metacognition Clinical Reasoning Novice “Expert” • Requires more cues from patient and environment. • Broad base of questions • Many hypotheses to be tested • Difficulty with pattern generation and recognition • Single hypothesis reasoning • Able to pick up cues more quickly from patient and environment. • Narrows focus for questions • Explores fewer hypotheses more thoroughly/deeply • Recognizes patterns easily in their domain • Able to reason in different hypotheses simultaneously “Being aware of one’s cognitive processes and exerting control over these processes” (Higgs and Jones, 2000) The ability to think about one’s clinical reasoning, and being able to modify one’s behavior based upon this awareness. Often seen as a progression toward mastery level and indicates that the student is able to use a hypothetico-deductive model reasoning process (Rushton, 2009) Jones and Rivett, 2004 1 9/3/2014 However, today we want to: • Explore how to improve clinical reasoning and metacognition through pattern recognition and the “lowly” case report • Show that pattern recognition really is more of a mastery level skill when you reason in different hypotheses categories simultaneously • Outline how to integrate case reports into Physical Therapy education—at entry level, residency, and fellowship level. Hierarchy of Evidence—Why the Case Report? 1. Case reports allow for individual patient considerations whereas they may be excluded from an RCT. 2. Case reports can give more detail to examination and treatments. 3. Case reports can explore more of the “why did I pick this specific diagnostic test, treatment procedure, etc.” to fit the patient case. 4. Case reports can “tell the patient’s story”. http://myhome.spu.edu/cfry/ebp.htm How does your student learn? Narrative Reasoning • The patient’s interpretation of his/her unique story • “Construction of Meaning” • Choice of what is expressed, what is emphasized, and what is not expressed • Gains insight into the patient’s experiences of disability, pain, beliefs, feelings, health behaviors. • Affects patient’s ability to learn and their learning styles • Affects treatment choice • Validated by consensus between patient and therapist. Howard Gardner’s Theory of Multiple Intelligences, 1983 Edwards, Physical Therapy, 2004 Another story….. 3 Broad Categories • Determining irritability is a skill that develops with clinical reasoning and experience. • Three categories of mental representation 1. Basic science 2. Formal knowledge of disease probabilities, scripts, and schemas 3. Experiential knowledge: exemplars aka pattern recognition. • Conclusion: “the more important finding is that focusing instruction on one processing strategy or another may be less important than engaging students with many problems, which are carefully sequenced to optimize learning and transfer.” Norman, Medical Education, 2005 2 9/3/2014 Entry Level DPT Years 1-3 “Paper” patients • Didactic Learning through “paper” or virtual patients • Designed case based upon a real patient or a well known clinical pattern or common diagnosis. • Use of Learning Platform like D2L, Blackboard • “Learn as you go” format • Reproducible and low cost • Limited visual unless videos are incorporated into the case • Pattern Recognition Notebooks • Based on didactic material/textbooks/Clinical guidelines • Additional Pattern Generation during clinical rotations • Selection of Case Report patient during clinical rotations • Guided by clinical instructor • Written case report 2nd year • Oral defense case report 3rd year • Use of 2nd year students to simulate paper patients for 1st year • Refines interview skills with practice • Transfers to clinical practice with real patients • Second year students then have more in depth discussions for examination and management, home setting, etc. • Meet with expert clinician and peers to discuss case as it progresses. • Can be interdisciplinary peers Patient Initiating the session Doctor Initial Rapport Virtual Patients in Primary Care • Swedish Qualitative Study of 3rd year medical school students • Interactive case study on a virtual learning platform • Videos of standardized patient and primary care MD embedded in case • 5 sections (see next slide) • Reflections in each section • Generally positive learning experience reported • Intermediate activity between didactic theory and real patients Gathering information The student’s strategy, history taking Clinical Reasoning Pattern Recognition Physical Examination Hypothesis Generation Patient’s ideas, concerns and expectations, The patient’s unique experience of illness Doctor’s ideas, concerns and expectations. The doctor’s agenda Preliminary diagnosis Collaboration during the physical exam Explanation and planning Shared understanding and involvement in decision making Closing the session Follow up and farewell (Salminen, 2014) (Adapted from Salminen, 2014) Virtual Patients Key Points cont. Pattern Recognition Notebooks 1. 2. 3. 4. 5. 6. • Use of clinical reasoning forms for visualizing pain referral patterns, reasoning in different hypothesis categories, and management • Common diagnoses and patterns at first didactic • Clinical patients when student goes on rotation reflection on action • Allows organization of patterns Preformulated comments based on EBP presented as text for case Text and video used for learning and collaboration Hyperlinks embedded in case Open ended questions allow free text answers by student Reflective thought guided by a virtual “tutor”. Student able to visualize and read communication (both verbal and nonverbal) between patient and health care provider 7. Reflection-in-action emphasized throughout culminating in reflection-on-action • Visual learners and mathematical/logical learners (Salminen, 2014) 3 9/3/2014 Clinical Pattern Subjective Form Clinical Pattern Disorder Name Common Pain Referral Pattern Subjective Characteristics Behavior of Symptoms • Aggravating • Ease • 24 hour • Precautions/Contraindications • History of Condition • Contributing/Predisposing Factors • • • • Physical Exam • Observation • Functional tasks • Active ROM • Passive ROM • Palpation/Joint Play • Prognosis • Impairments • Functional Limitations • Disabilities • Pathobiological Mechanism • Management/Treatment • Goals • Supporting Evidence Used with permission – Mark Jones The clinical reasoning form can be a way of forcing the student to analyze the patient presentation Another Story….. • Identifying motivation for the patient and psychological factors may be more important than the impairment itself. • Draw a “pie chart” on the diagram that reflects the proportional involvement of the pain mechanisms apparent after completing the subjective examination. Hypotheses Categories Case Report • Activity and Participation Capabilities/Restrictions • Patient’s perspectives and beliefs/psychosocial factors • Physical Impairments and associated structure/tissue sources • Pathobiological Mechanisms • Contributing factors • Precautions and Contraindications • Management and Treatment • Prognosis • Actual writing of case report • Can fulfill CAPTE requirements (entry level) and also demonstrate clinical reasoning in clinical setting • Merging of didactic and clinical education • Case report selection is critical • Promote professionalism • May need to assist student by finishing case and/or data collection Jones and Rivett, 2004 4 9/3/2014 Selection of Case Report (cont.) Writing Case Reports • What can you do as a clinical educator to ensure student success with case report selection? • Break into sections • • • • • • • Unique diagnosis or presentation or treatment approach As complete course of care as possible Use an outcome measure Take good notes/records while maintaining HIPAA Guide selection of tests and treatments with evidence if possible This is where we shape clinical reasoning “What makes this case interesting? What is my angle to discuss?” • • • • • • Lit Review Case Description, Outcome Measures, Examination, Intervention Clinical Impression(s) Background and Purpose Outcomes, Discussion, and Conclusion Abstract when case is final/complete • Mixed media to introduce writing technique/material • Meet to review with peers and/or faculty facilitator • Weekly, Biweekly, Monthly • Writing on a Timetable Case Defense • Oral defense of case that is based upon written report • Case report selection during clinical rotations • Displays oral communication skills in entry level, residency, and fellowship trained students • Presented to peers, clinical faculty, and clinical educators • Can be poster presentation at conference Errors in clinical reasoning in entry level and beyond • Faulty perception or elicitation of cues • Deficiency in basic clinical skills • Incomplete factual knowledge about a disease process or clinical condition • Deficiency in content knowledge • Misapplication of known facts to a specific problem • Incorrect use of heuristics • ie. Mechanical Diagnosis and Therapy applied to all patients with low back pain. A final story Entry Level to Residency to Fellowship • Second year student with a patient with low back pain. • Should demonstrate a progressively deeper body of knowledge • More ability to reason in different hypothesis categories • More ability to reason using dual processing • More ability to treat patient with different theories • More ability to explain and defend reasoning using different theories • “I really thought I should extend him. But it worsened his pain and it stayed worse.” • “We were taught McKenzie theory as our low back pain framework. It blew my mind that he would get worse if I extended him.” • Can use vignettes, clinical patterns, written case report, and case defense in all three levels of Physical Therapy education 5 9/3/2014 Errors in Clinical Reasoning Norman 2009, Mamede 2014 (Not a complete list) • Availability • Tendency to judge diagnoses as more likely if they are more easily retrievable from memory Processing Strategies • Base rate neglect • Tendency to ignore the true rate of disease, and pursue rare but more exotic diagnoses Errors in Clinical Reasoning • Confirmation Bias Carol A Courtney • Premature closure • Tendency to seek data to confirm, not refute the hypothesis. • Tendency to stop too soon without appropriate consideration of alternative possibilities • ‘Salient distracting features’ Diagnostic error (medical) Graber et al. 2005 Dual processing • Analyzed 100 diagnostic errors • Found an average of 5.9 cognitive errors per case • Found 4 categories: • • • • Faulty Knowledge (11 occasions) Faulty Data Gathering (45) Faulty Information Processing (159) Faulty Verification (106) • Intuitive (fast): • earlier in evolutionary development, and is rapid, contextual, holistic, and unavailable to introspection • Automatic formation of memories • Analytical (slow): • abstract and inductive Dual Processing System 1 (Intuitive) • experience-based and automatic • consistent with memories of individual experiences • access based on similarity between the present situation and prior experience Intuitive Processing – Implicit Learning System 2 (Analytical) • conscious, logical, and without context • places heavy loads on working memory, and is energy-intensive 1. Pattern recognition 2. Common-sense understanding: • Identification of subtle trends; 3. Similarity recognition: • ability to recognize subtle likenesses to cues found in past episodes 4. Sense of salience: • Identifying key pieces of information • Determining relevance versus irrelevance; 5.Deliberative rationality: • Selective attention to certain aspects or events 6. Skilled know-how: • Experiential knowledge, where the tools of a practical situation become an extension of one’s self. Ken Randall Dissertation 2009 6 9/3/2014 Analytical Processing 1. 2. 3. 4. Which is better? Intuitive or Analytical? Hypothesis generation Application of clinical prediction rules Application of evidence based practice Reflection Analytical Processing: Reflection in/on Action Intuitive Processing • “inherently flawed” • Solution: slow down • Valuable in the early stages of learning • Reflection strategies explicitly mobilize analytical knowledge Kahneman 2011 • Promotes greater ‘accessibility’ to knowledge base • Medical decision making may be different • Dependent on both systems • diagnoses are not reasoned so much as they are recognized Monteiro and Norman 2013 What happens when intuition fails us? Utilizing both Intuitive and Analytical Thinking • When signs and symptoms of a diagnosis do not fit: • Response not triggered • With recognition failure, System 2 (Analytical) will engage • Alternatively: • clinician may act against better judgment and behave irrationally • Clinician rejects System 2, and defaults to System 1 (Intuitive) • Good decision makers consciously blend their processing styles • Although System 1 (intuition) operates at an unconscious level, its output, once seen, can be consciously modulated by adding a System 2 (analytical) approach • Engagement of System 2 may occur when it “catches” an error in System 1 Croskerry and Norman 2008 Risen and Gilovich 2007 7 9/3/2014 Overconfidence Questions to ponder… • Not always a bad thing? • Leads to definitive action • However, • intuitive thinking may be associated with strong emotions such as excitement and enthusiasm. Such positive feelings, in turn, have been linked with an enhanced level of confidence in the decision maker's own judgment Tiedens and Linton 2001 • A specific number of practice hours are the standard requirement before undertaking OMPT Fellowship training, meaning: • Can lead to: • Better to gain intuitive knowledge before encouraging a analytical monitoring of intuitive processing? confirmation bias References • Daniel Kahneman (2011). Thinking, Fast and Slow. Farrar, Straus and Giroux, New York. • Edwards, I, Jones, M, Carr, J, Braunack-Mayer, A, Jensen, G. (2004). Clinical Reasoning strategies in physical therapy. Physical Therapy. 84(4):312-330. • Gardner, Howard (1983). Frames of Mind: The Theory of Multiple Intelligences, Basic Books, ISBN 0133306143 • Jones, M. and Rivett, D. (2005). Clinical Reasoning for Manual Therapists. Philadelphia: Elsevier. • McEwen, I. (Ed) (2009). Writing Case Reports: A How-To Manual for Clinicians. Washington D.C.: American Physical Therapy Association. • Miller, P, Rivett,D, Isles, R. (2009). Pattern recognition is a clinical reasoning process in musculoskeletal physiotherapy. ANZAME09 Handbook, Launceston, NSW. • Monteiro S and Norman G. (2013). Diagnostic Reasoning: Where We’ve Been, Where We’re Going. Teaching and Learning in Medicine, 25(S1), S26–S32 • Norman, G (2005). Research in clinical reasoning: past history and current trends. Med. Educ. 39:418-427. • Norman G (2009). Dual processing and diagnostic errors. Adv in Health Sci Educ 14:37–49. • Rushton, A, Lindsay, G. (2010). Defining the construct of masters level clinical practice in manipulative physiotherapy. Manual Therapy. 15:93-99. • Salminen, H. et al. (2014). Virtual patients in primary care: developing a reusable model that fosters reflective practice and clinical reasoning. J Med Int Research. 16 (1):1438-8871. 8