Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
AMEBICAN JOUBNAL or EPIDEMIOLOGY
Vol. 98, No. 5
Copyright O 1973 by The John* Hopkins University
Printed in U£.A.
RECURRENT OUTBREAKS OF MEASLES,
CHICKENPOX AND MUMPS
I. SEASONAL VARIATION IN CONTACT RATES1
WAYNE P. LONDON-" AND JAMES A. YORKE*
(Received for publication April 19,1973)
chickenpox; communicable diseases; disease outbreaks; epidemiologic
methods; measles; models, theoretical; mumps; varicella
INTRODUCTION
rent outbreaks in large populations (2).
Outbreaks of infectious diseases have The seasonal variation in the reported cases
been studied frequently by mathematical o f measles, for example, has been long
models (1-9). Although useful in describ- recognized (3, 10) but whether or not there
ing single outbreaks of a few months' dura- is seasonal variation in the contact rate has
tion in small populations, deterministic not been investigated,
models have not predicted undamped recurThe contact rate of a disease in a given
...
,
population is the fraction of the suscepti'This research was partially supported under , ,
, ,
. , ,.
...
National Science Foundation Grant GP-313S6X1. ™™ that an average infective successfully
•Mathematical Research Branch, National In- exposes per day. In this paper contact rates
stitute of Arthritis, Metabolism, and Digestive for measles, chickenpox and mumps are
Diseases, Bethesda, Md. 20014.
estimated for each month of a 30- or 35* Institute for Fluid Dynamics and Applied
. . ,
,
,,
,
,
Mathematics, University of Maryland. College Year-period from the monthly reports of
Park. Md. 20740.
cases of the three diseases in New York
453
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
London, W. P. (Mathematical Research Branch, National Institute of
Arthritis, Metabolism, and Digestive Diseases, Bethesda, Md. 20014) and
J. A. Yorke. Recurrent outbreaks of measles, chickenpox and mumps. I.
Seasonal variation in contact rates. Am J Epidemiol 98:453-468, 1973.
—Recurrent outbreaks of measles, chickenpox and mumps in cities are
studied with a mathematical model of ordinary differential delay equations. For each calendar month a mean contact rate (fraction of susceptibles contacted per day by an infective) is estimated from the monthly reported cases over a 30- to 35-year period. For each disease the mean
monthly contact rate is 1.7 to 2 times higher in the winter months than in
the summer months; the seasonal variation is attributed primarily to the
gathering of children in school. Computer simulations that use the
seasonally varying contact rates reproduce the observed pattern of undamped recurrent outbreaks: annual outbreaks of chickenpox and
mumps and biennial outbreaks of measles. T h e two-year period of
measles outbreaks is the signature of an endemic infectious disease that
would exhaust itself and become nonendemic if there were a minor increase in infectivity or a decrease in the length of the incubation period.
For populations in which most members are vaccinated, simulations show
that the persistence of the biennial pattern of measles outbreaks implies
that the vaccine is not being used uniformly throughout the population.
454
LONDON AND YOBKE
implies that the present use of the vaccine
is strongly non-uniform and that in spite of
the reduced numbers of cases, in some
groups in society the disease is as prevalent
as ever.
In a subsequent paper (11) the estimated
contact rates are used to study the spread
of the three infections in society and stochastic effects of populations of different
sizes are analyzed. A general formulation of
the model will appear elsewhere (12).
THE DATA
The monthly number of reported cases of
measles, chickenpox and mumps in New
York City and measles in Baltimore is
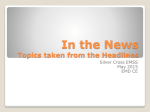
shown in figure 1. In New York City, from
1945 until widespread use of the vaccine in
the early 1960's, outbreaks of measles occurred every other year in the even-numbered years. Prior to 1945 outbreaks
occurred essentially every two years with
extra high years in 1931, 1936, and 1944;
two consecutive low years occurred in 1939
and 1940, followed by an exceedingly high
year in 1941. From 1929 to 1963 the average number of reported annual cases in
New York City was about 18,000. In Baltimore from 1928-1959 outbreaks of measles
occurred essentially even' second or third
year with no apparent pattern to the biennial or triennial recurrences; the average
number of reported annual cases was about
5000. In both New York City and Baltimore the dramatic effect of extensive vaccination is seen after 1966. In both cities the
largest number of cases of measles occurred
in the spring: in the high years in March,
April or May and in the low years in April,
May or June. The minimum number of
cases occurred in August or September.
In New York City outbreaks of chickenpox and mumps that peaked in the spring
months occurred annually. The average annual number of reported cases was about
9800 for chickenpox and about 6500 for
mumps.
The fraction of cases of each disease that
are reported can be estimated from the
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
City and measles in Baltimore. For each
calendar month the 30 or 35 monthly contact rates are averaged to obtain a mean
monthly contact rate for that month. The
year-to-year variation in the contact rate
for any month is small relative to the
seasonal variation: for the three diseases
the mean monthly contact rates are 1.7 to 2
times higher during the autumn and winter
months than during the summer months.
This seasonal variation is apparently caused
by the close contacts made by children,
particularly during the coldest months,
when school is in session. Simulations that
use the seasonally varying contact rates
show the pattern of the outbreaks of measles, chickenpox and mumps: undamped
recurrent outbreaks that peak in the spring
months. The large seasonal variation in the
contact rates appears to be an essential
feature of any realistic model of recurrent
outbreaks of these diseases in cities.
Measles with its biennial pattern of recurrent outbreaks is shown to be in a
narrow border region between "highly efficient" nonendemic diseases and "less efficient" diseases such as chickenpox and
mumps that are endemic with regular oneyear outbreaks. Our simulations reproduce
the annual outbreaks of chickenpox and
mumps and the biennial outbreaks of measles in which the observed ratio of cases in
the high year vs. the low year is 5:1. The
simulations show further that if the incubation period of measles were longer than 12—
13 days or if the infectivity were slightly
lower the outbreaks of measles would occur
annually. If the incubation period were as
short as 10 days or if the infectivity were
slightly higher, the disease would die out, at
least locally, and no regular pattern of
outbreaks would be observed.
Recurrent outbreaks in a population in
which many members are vaccinated are
more difficult to model accurately because
the numbers and social characteristics of
those vaccinated usually are not known.
Simulations show, however, that the continuing biennial pattern of measles outbreaks
455
OUTBREAKS OP MEASLES, CHICKENPOX AND MUMPS. I.
6000-
4000-
2000-
1000
N e w ' i M City
20001-
1000-
2000|-
YEAR
FIGURE 1. Monthly number of reported cases of measles, chickenpox and mumps in New
York City and Mensles in Baltimore.
birth rates (13, 14) if the changes in susceptibles due to immigration and emigration are neglected and if it is assumed that
by age 20 nearly all children acquire measles, 68 per cent acquire chickenpox and 50
per cent acquire mumps (15). On this basis,
the rate of reporting of each disease is 1 in
8 cases of measles in New York City, 1 in 3
to 4 cases of measles in Baltimore and 1 in
10 to 12 cases of chickenpox and mumps in
New York City. (Since at least 25 per cent
of infections of mumps are subclinical, the
reported fraction of infections of mumps
would be correspondingly smaller.)
THE MODEL
A contact or an exposure of a susceptible
by an infective is defined as an encounter in
which the infection is transmitted. The
contact rate is denned as the fraction of
susceptibles in a given population contacted
per infective per day. The contact rate
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
2000-
456
LONDON AXD YORKB
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
reflects the social behavior of the members
Since we are interested in diseases that
of society and the ease with which the can be acquired only once, the rate of
disease is transmitted; both factors may change of susceptibles, dS/dt, equals the
vary during the year. Suppose that, at time constant net rate of entry of susceptibles y
t, E(t) is the number of exposures per day, minus the rate of exposure E(t), that is
S{t) is the number of susceptibles and I{t)
dS/dt = y - E{t)
(2)
is the number of infectives. Then the fraction of susceptibles exposed per day by all This equation implies that after being coninfectives is E(t)/S{t) and the contact rate tacted by an infective a susceptible immefi(t) is given by
diately leaves the susceptible population; it
is shown later that multiple contacts of a
susceptible can be neglected.
The number of exposures per day is given
We assume that all individuals exposed
by
at time t incubate the disease for time Tx,
are infectious for time T% and then cease to
E{t) =
(1) be infectious and remain permanently im(Alternatively if v is the total number of mune to reinfection. The rate of change of
contacts of both susceptibles and immunes infectives dl/dt equals the rate of appearmade by an infective per day and N is the ance of infectives, which is the exposure
total population, then the number of expo- rate time 7\ ago, minus the rate of disapsures per day is given by E(t) = v(S(t)/ pearance of infectives, which is the expoN)I(t) and the contact rate is given by /? sure rate time Ti + T2 ago. Thus
= v/N; if v varies during the year, so does
dl/dl = E(t - Ti) - E(l - T1 - T^.
/S-)
We assume that the net rate of entry of Integration of this equation yields
susceptibles into the population is constant.
This net rate is the sum of the rates of
= /
E(s) ds.
(3)
entry of susceptibles from births and from
immigration minus the rate of loss of sus- This equation states that the number of
ceptibles from emigration and the rate of infectives at any time equals the sum of the
the loss of individuals who do not acquire exposures made in the previous Ti 4- T2 to
the disease by, for example, age 20, and Ti days. (In the more general formulation
hence leave the school-aged susceptible of the problem (12) the definition of I(t)
population. (In 1935-1936, for example, by differs from the definition here by the mulage 20, 5 per cent of an urban population tiplicative factor T->.)
had no history of measles, 32 per cent no
The basic equations 1, 2 and 3 follow
history of chickenpox, and 50 per cent no naturally from the assumptions that the
history of mumps (15).) The assumption of rate of exposure is proportional to both the
a constant input of susceptibles is, of number of susceptibles and the number of
course, an approximation. The birth rate in infectives, that the disease confers permaNew York and Baltimore, for example, nent immunity and that there exists an
decreased by about 30 per cent during the incubation and an infectious period. The
1930's and rose again during the next two same equations appear, for example, in the
decades (13, 14). Significant immigration work of Wilson and Burke (16).
and emigration also occurred in both these
The two delays—T1? the time from expocities, but it is virtually impossible to meas- sure to infectivity and T2, the duration of
ure these migrations or to know the fraction infectivity—require interpretation. We are
of the immigrant or emigrant population interested in the spread of disease in sothat was susceptible.
ciety, and not among siblings in a house-
OUTBREAKS OF MEASLES, CHICKENPOX AND MUMPS. I.
457
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
METHOD
hold (the cases of which are less likely to
affect the spread of disease in society and
The data used to calculate the monthly
less likely to be reported (17)); therefore,
contact rates are the notifications of cases
we assume that an infective ceases to transof each infectious disease received by the
mit the disease when he is confined at home
city health departments (usually by postal
by the severity or the characteristic feacard) during any month. (The monthly
tures of the disease (e.g., the rash). The
notifications are given in the appendix of
infective is assumed to manifest constant
the following paper (11).) Since the delay
infectivity for a period of time equal to T2
from exposure to diagnosis is about two
before being withdrawn from society. 7\ is
weeks and the delay from diagnosis to the
then the time from exposure to the beginreceipt of notification in the health departning of infectivity; although called the
ment is estimated to be about 10 days, the
incubation period, it is perhaps a few days
monthly totals for one month represent
shorter than the usual incubation period,
mainly the exposures from the previous
which is defined as the time from exposure
month. Thirty-five consecutive years of
to the onset of symptoms. The choices of
data (prior to the use of the vaccine) were
the length of the delays, Tx and T2 are
used to calculate the monthly contact rates
based on the epidemiology of the individual
of measles in New York City and Baltimore
diseases (18, 19).
and 30 consecutive years of data for chick For purposes of computation we use a
enpox and mumps in New York City.
fixed time interval A, usually one day, let
We define the disease year of, say 1950,
the nth time interval be tn = nA, and
as the 12 months from September 1, 1949,
approximate equations 1-3 by the difference
through August 31, 1950. For measles, a
delay equations (A — 1),
high year is a disease year in which many
E(tn) = fKQKQSiL)
(4) cases were reported (in New York City,
greater than 21,000; in Baltimore, greater
S(tn+l) = S(tn) ~ E(tn) + y
(5) than 4900 cases) and a low year is a disease
year in which few cases were reported (in
/(WO = E E(k-i + 1)
(6) New York City, less than 13,000; in Balti.-7-!
A distribution of incubatio?i periods and more, less than 3800 cases).
In order to calculate a contact rate for
models without delays. A broad distribution
each
month of the 30 or 35 disease years,
of incubation periods similar to that rethe
number
of susceptibles at the beginning
ported by Sartwell (19) can be incorpoof
each
epidemic
year was estimated. The
rated into the delay equation model by
estimation
of
susceptibles
is independent of
assuming, for example, that 1/8 of the
the
model
or
the
choice
of
parameters
of the
exposed individuals incubate the disease for
model
{T-i,
T
,
y,
or
fi(t)).
A
mean
contact
2
9 days, 1/8 for 10 days, . .. , 1/8 for 16
rate for each calendar month was then
days. Equation 3 is replaced by
estimated from the data of monthly notifi7(0 = (1/8) [
[ /3(u)S(u)T(u)duds. cations. This was done for each choice of
Tj, the duration of the incubation period,
•I i-Tj
J$-n
(A distribution of incubation periods in and r 2 , the duration of the infectious pewhich half the exposed individuals incubate riod. The constant net input of susceptibles,
the infection for 12 days and half for 13 7, was not required in the estimation of the
monthly contact rates. Finally, for each
days is denoted by T± - 12 to 13.)
The incubation and infectious periods can choice of Tx and T2 the corresponding
be also modeled by ordinary differential estimated mean monthly contact rates and
equations without delays (see appendix 1). a constant net input of susceptibles, y, was
458
LONDON AND YOEKE
Second, a slight variation of the result
can be proved for the model. We first
consider a simple model without delays that
assumes no incubation period. (This model
is discussed in appendix 1.) Equation 3 is
replaced by dl/dt = p{t)S{t)I{t) - (1/S)
I(t) where 8 is the mean length of the
infectious period. At tf, the time of the peak
of the outbreak, dl/dt = 0 and S{tp) = Sp
= l/(S/3), where /S is the contact rate at
the time of the peak. For the more realistic
delay equation model that has an incubation period: an infective infects fiS(t) susceptibles per day so that during T2 days of
infectivity fiS(t)T2 susceptibles are infected. At the peak of an outbreak each
infective infects exactly one susceptible and
so (within a minor correction for the delays) pS{tP)T2 = 1 or S(tp) = l/(T2f3).
For Sp to be independent of the time of the
peak these arguments require that /3(£) does
not change much during the months when
the peaks occur.
The values of Sp and the average annual
number of reported cases are given in table
1. These values of Sp for New York City
yield a total susceptible population that is
close to that calculated from census data
(13) and age specific attack rates (15). For
measles in Baltimore, the value of *SP yields
a total susceptible population that agrees
with the findings of Hedrich (20). The
values of Sp for chickenpox and mumps can
be changed by at least 50 per cent without
TABLE 1
Values of Sp and average annual number
of reported canes of measles, chickenpox
and mumps in A'eio York City and
measles in Baltimore
City and disease
New York City
Measles
Chickenpox
Mumps
Baltimore
Measles
sr
Average
annual
reported
casej
70,000
85,000
90,000
18,000
9,800
6,600
13.7
20,000
5,000
4.0
Ratio
3.9
8.8
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
used in a simulation of the recurrent outbreaks.
Estimation of susceptibles for the calculation of contact rates. The number of
susceptibles at the beginning of each of the
30 or 35 disease years was estimated by
assuming that at the peak of each outbreak
the number of susceptibles equals a constant number Sp. Thus, at the beginning of
a particular September the number of susceptibles equals Sp plus the number of
reported cases from that September to the
peak of the outbreak that year. Under this
assumption each observed annual outbreak
of chickenpox is assumed to begin with
essentially the same number of susceptibles
because the number of reported cases from
each September to the peak of each outbreak is roughly the same. The same is true
for the observed annual outbreaks of
mumps. For measles, a high year is assumed to begin with a large number of
susceptibles (Sp plus the large number of
reported cases from that September to the
peak) and each low year is assumed to
begin with a correspondingly smaller number of susceptibles. The more contagious the
disease the more contacts each infective
makes and hence the smaller the number of
susceptibles at the peak. That the number
of susceptibles should equal a constant at
the peak of an outbreak is intuitive since at
the peak the number of exposures per unit
time is neither increasing nor decreasing.
The idea may be justified in two ways.
The result was found empirically by
Hedrich (20), who estimated the number of
susceptibles to measles for each month in
Baltimore from 1900-1930 from census data
and the number of reported cases. From
1900-1914 the average number of susceptibles at the peak of each outbreak was
63,700 with a coefficient of variation
(standard deviation divided by the mean)
of less than 4 per cent; for 1921-1930 the
corresponding figures were 74,000 with a
coefficient of variation of less than 6 per
cent. (The population of Baltimore rose
substantially in 1918 (14).)
OUTBREAKS OF MEASLES, CHICKENPOX AND MUMPS. I.
from year to year. The mean monthly
contact rate for each calendar month is the
average of the 30 (or 35) contact rates for
that month. A mean monthly contact rate
was calculated for each choice of T^_ and T2.
The monthly contact rates calculated by
the above method showed a "see-saw" highlow pattern even after they were averaged
for all years. If the rate for one month was
exceptionally high, the rate for the next
month was unduly low. The raw monthly
contact rates (/3r) were smoothed according
to the formula
/S(t) = 0.26j8,(i - 1)
+ 0.5 j8r(i) + 0.25 0,(i + 1)
where t = 1 , . . . , 12 (if i — 1, use 12 for i —
1, etc.). The statements about the mean
monthly contact rates do not depend on the
smoothing.
Simulations. Equations 4-6 were used to
simulate the recurrent outbreaks. For each
choice of J"i and T^ the corresponding curve
of the 12 mean monthly contact rates estimated from the data of monthly notifications was used. The constant net input of
susceptibles y equalled the average annual
number of reported cases of each disease. In
most simulations it made little difference if
the susceptibles were added equally
throughout the year, or, to mimic the gathering of children in school, added at the
beginning of the disease year. An arbitrary
initial estimate of susceptibles and infectives was needed to begin the iteration of
equations 4-6; after several years of simulated time, a pattern of stable, recurrent,
undamped outbreaks that persist indefinitely was obtained. The estimation of susceptibles that was used in the calculation of
monthly contact rates was not required for
the simulations.
Most simulations were made to determine
under what conditions the equations would
produce biennial outbreaks similar to those
of measles in New York City (figure 1). In
these outbreaks the average number of reported cases was about 30,000 in the high
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
altering the relative shape of the curve of
the mean monthly contact rates or the
results of the simulations. For measles the
choice of Sf is quite critical. If Sp is decreased by about 15 per cent too few susceptibles are available at the end of the
high year and the corresponding contact
rates are systematically high; if Sp is decreased by about 10 per cent the simulations yield biennial outbreaks but the ratio
of cases between the high and low years is
greater than the observed ratio of 5:1. If Sj,
is increased by about 10 per cent the simulations yield a ratio of cases that is less
than the observed ratio; a 20 per cent
increase in Sp yields simulations of annual
outbreaks (ratio of cases of 1:1).
Estimation of the mean monthly contact
rate. A contact rate for each month of a 30or 35-year-period was calculated from the
data of monthly notifications by the use of
equations 4-6 in the following way. The
number of susceptibles at the beginning of
each of the 30 or 35 disease years was
specified by the method described. A contact rate was found for each month, starting with September of the first year, such
that the calculated number of exposures
equalled the reported number of exposures
for that month. (The contact rate was
found by a "shooting" technique: successively smaller contact rates were tried until
the calculated exposures equalled the reported exposures). To start the calculations
the reported exposures for the preceding
August were distributed equally throughout
the month; thereafter, the pattern of exposures calculated for a month was used in
calculating the contact rate for the next
month. The number of susceptibles at the
beginning of a month equalled the number
of susceptibles at the beginning of the
previous month minus the exposures for the
month. (In some calculations new susceptibles were added each day throughout the
year, but, in general, the constant net input
of susceptibles, y, was zero.) Each September the number of susceptibles was specified; susceptibles were not carried over
459
460
LONDON AND YOBKE
RESULTS
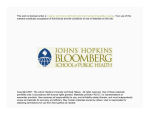
Mean monthly contact rates. The mean
monthly contact rates for measles, chickenpox and mumps in New York City and
measles in Baltimore are shown in figure 2.
In both cities the measles contact rates in
June, July and August are low. The curves
rise sharply from August to October, re-
main high from November until March or
April and then fall steeply from May to
June. The ratio of the peak month to the
lowest month is about 1.7 in New York; in
Baltimore, 1.6. The contact rate for mumps
shows similar features as the curves for
measles. The curve for chickenpox, however, peaks in October and has a sharp
decline from October to December; the
ratio of the peak month to the lowest month
is about 2. In a subsequent paper (11) these
special features of the seasonal variation in
the contact rate for chickenpox are related
to the clustering of susceptibles with infectives and to the spread of chickenpox
through the population.
Figure 2 shows that for any given month
the variation in the monthly contact rates
from year to year for that month is small
compared to the seasonal variation from
month to month. The coefficients of variation (standard deviation divided by the
mean) for measles, chickenpox, and mumps
in New York City are about 10, 7 and 5 per
cent, respectively, and about 18 per cent for
measles in Baltimore. Some months show
systematic differences in the mean monthly
contact rates for all three diseases between
the years with a large number of cases and
years with fewer cases and for chickenpox
between the early and late years of study.
These systematic differences, which contribute to the variation in the monthly contact
rates from year to year, are discussed in a
subsequent paper (11).
The curves of the mean monthly contact
rates are not changed by any of the following alterations: 1) the length of the incubation period is changed by 50 per cent or a
distribution of incubation periods is assumed (for measles as long as 9 to 16
days); 2) the infectious period is changed to
one or three days; 3) the level of susceptibles (Sp) is changed by as much as 50 per
cent (for measles, if Sp is decreased by 15
per cent, not enough susceptibles remain at
the end of a high year and erroneously high
contact rates are calculated for these
months); 4) susceptibles are added each
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
year and about 6000 in the low years, a
ratio of 5:1. For measles the criterion of a
successful simulation was a recurrent outbreak every other year with a ratio of high
year to low year cases of about 5:1.
Multiple contacts of a susceptible. In the
calculation of the mean monthly contact
rates and in the simulations, the difference
equations 4-6 were solved numerically on a
computer. The step size A was selected such
that further reduction had negligible effect
on the results; one iteration per day was
sufficient.
Because the time interval of iteration was
one day or less, and not 14 days (3, 4), the
chance of a susceptible being contacted by
more than one infective is very small. At
the peak of the simulated outbreak of
measles in New York City there are about
560,000 susceptibles and about 2400 exposures per day; the daily probability of
exposure for any susceptible is 2400/560,000 or about .0043. The number of occurrences of a susceptible being contacted by
two infectives in one day is (.0043)2- 560,000 = 10.4, which is negligible with respect
to the 2400 exposures. Thus, the correction
for multiple contacts, which is the distinguishing feature of the Reed-Frost model
(4), changes the exposure rate by at most
0.43 per cent (10.4/2400). The Reed-Frost
correction, usually employed when the iteration step size is 14 days, causes an error
(and corresponding correction) 142 times
larger than the correction here. That similar mean monthly contact rates and similar
simulations are obtained with iteration step
sizes of one day or as small as 1/8 of a day
implies that multiple contacts of a susceptible are not important.
OUTBREAKS OF MEASLES, CHICKENPOX AND MUMPS. I.
1.4
MEASLES
1.2
1.0 -
•1
0.8
CHICKENPOX
1-2 h
<
i-
o
o
day throughout the year; 5) the contact
rates are calculated using models of ordinary differential equations that assume an
incubation period (see appendix 1). Mean
monthly contact rates calculated from data
from individual boroughs in New York City
show the same features as those calculated
for the entire city.
Simulations with a constant contact rate.
The first result from the simulations is that
seasonal variation in the contact rate is
necessary to simulate undamped recurrent
outbreaks that peak in the spring months.
If the contact rate is assumed constant and
susceptibles are added equally throughout
the year, simulations yield damped waves
of outbreaks that approach a constant endemic level of disease. This constant limiting solution is
. 0.8
<
UJ
0.6
MUMPS
1.2
1.0 -
0 8-
0.6
JJASONDJFMAMJJA
FIGURE 2. Mean monthly contact rates for
measles, chickenpox and mumps in New York
City. The contact rates are normalized by #, the
average of the 12 mean monthly contact rates.
The bars show one standard deviation on either
side of the mean. The dashed line in the top panel
is the mean monthly contact rate for measles in
Baltimore. Because of delays due to the incubation period and in reporting, the notifications
from one month correspond to the contact rate of
the previous month. For measles, T\ = 12 to 13
days: in New York City (1929-1963), $ = 7.25 X
lO-«; in Baltimore (1925-1959), 0 = 2.65 X HT8.
where p is the constant contact rate, T2 the
infectious period, and y the constant net
input of susceptibles. If the contact rate
is assumed constant but the susceptibles are
added only at the beginning of the disease
year (to model the gathering of children in
school), the simulations show outbreaks in
which either the cases are distributed evenly
in all months of the year or if a well defined
peak occurs, the peak is not in the spring
months.
Simulations of measles epidemics: allowable incubation periods. The following simulations were done with the seasonally
varying mean monthly contact rates calculated from the data of monthly notifications.
An important factor in simulating biennial outbreaks of measles that have the
observed ratio of high year to low year
cases is the duration of the incubation
period. If the incubation period is assumed
For chickenpox in New York City (1931-19(30),
7\ = 13 days and 0 = 6.07 X 10"«. For mumps in
New York City (1934-1963), 7\ = 16 days and £ =
5.64 X 10"«. For all diseases Tt = 2 days.
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
0.6
461
462
LONDON AND YORKE
MEASLES
6000
4000
1000
MUMPS
1000
SONDJFMAMJJASONDJFMAMJJASONDJFMAMJJASONDJFMAMJJA
MONTH
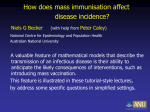
FIGURE 3. Simulations of the recurrent outbreaks of measles, ehickenpox and mumps in
New York City. The mean monthly contact rates and the values of 7\ and T2 from figure 2
were used. The constant net input of susceptibles, y, which equals the average annual number of reported cases, was measles—18,000; ehickenpox—9800; and mumps—6500. The dashed
line is the simulation of the recurrent outbreaks of measles with the modified exposure rate,
pU)SU)I(t) (l-c/(£)), where c = 0.00015.
to be 12 to 13 days, biennial outbreaks are
simulated. For the mean monthly contact
rate from New York City the ratio of high
year to low year cases from the simulated
outbreaks is 5:1 (figure 3); for the mean
monthly contact rate from Baltimore the
ratio from the simulated outbreaks is 6.5:1.
If the incubation period is assumed to be
shorter than 12 days, biennial outbreaks are
not simulated. Too many cases occur when
susceptibles are plentiful and in succeeding
years not enough susceptibles and infectives
are present to sustain the disease. (In the
year following the high year the susceptibles are replenished but the infectives are
now too low to sustain the disease. Introduction of additional infectives prevents the
disease from fading out in that second
year.) If the duration of the incubation
period is 14 days, too few cases occur when
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
2000
OUTBREAKS OF MEASLES, CHICKENPOX AND MUMPS. I.
simulated high year outbreak occurs earlier
(March and April) than the peak of the
simulated outbreak in the low year (April
and May); further, the exposures in the
summer after the low year are about 25 per
cent higher than the exposures in the summer following the high year. These two
qualitative features are not present in the
simulation already mentioned in which the
exposure rate is not modified.
The role of the incubation period and
level of infectiousness in determining epidemic patterns. Once the parameters are
determined, the model allows us to determine the role of the incubation period and
the role of the level of infectiousness in
epidemic patterns. For example, if measles
had a shorter (or longer) incubation period,
would it still be endemic in the New York
City area, and if endemic, would it still
have a biennial pattern of outbreaks with a
ratio of high year cases to low year cases of
about 5:1? Equivalently, we may ask, suppose a virus disease appeared with the same
level of infectiousness as measles, that is,
with the same contact rate, but having a
different incubation period, what would be
the pattern of recurrent outbreaks? Using
the contact rate obtained for measles (calculated using Tt = 12 to 13 and T2 = 2
days), we simulate these situations by assuming incubation periods of different
lengths (T2 always equals two days). If the
incubation period T\ is assumed to be three
days, the peak of the outbreak occurs in
December or January. The disease dies out
after the peak, is no longer endemic, and
the pattern of outbreaks appears similar to
that of influenza (18). If the incubation
period is increased slightly, the ratio of
high year cases to low year cases becomes
smaller. Finally, if Ti is greater than or
equal to 16 days, annual outbreaks (ratio
of cases is 1:1) that peak in the spring are
simulated.
We may similarly ask how the level of
infectivity affects the pattern of measles
outbreaks. If the infectivity is increased by
15 per cent (modeled by a 15 per cent
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
susceptibles are plentiful; biennial outbreaks are simulated but the ratio of high
year to low year cases is about 3:1. For an
assumed incubation period of 16 days the
simulations show annual outbreaks (ratio
of cases of 1:1).
As long as the duration of the incubation
period is 12 to 13 days, assumptions about
the range of the distribution of incubation
periods (19) and the length of period of
infectivity are not critical. For example, the
assumption that half the individuals incubate the disease for 12 days and half for 13
days gives the same simulation as the assumption that 1/8 of the individuals incubate the disease for 9 days, 1/8 for 10 days,
. . . , and 1/8 for 16 days (the mean incubation period being 13 days). It also makes no
difference if the period of infectivity is
assumed to be one, two or three days.
(There is a redundancy in the choice of
difference values for r x and T2. For example, the assumption that half the individuals incubate the infection for 12 days and
half for 13 days and then are infectious for
one day is the same as the assumption that
all individuals incubate the infection for 12
days and then are infectious for two days.)
Simulations of measles outbreaks with a
modified exposure rate. Mean monthly contact rates were also calculated with a modified
exposure rate of the
form
p(t)S(t)I(t) (1 - cl(t)). As discussed in a
subsequent paper (11) the modification eliminates a systematic difference in the mean
monthly contact rates between the high and
low years that occurs in the spring months.
The maximum modification of the exposure
rate is about 7 per cent at the peak of the
outbreak, and the parameter c can be chosen small enough so that the number of
infectives in the low years is so small that
the modification has negligible effect. This
modification produces simulations that
most faithfully reproduce the observations
in New York City. Biennial outbreaks with
the observed ratio of cases of 5:1 are
simulated (figure 3). Like the outbreaks in
New York City (figure 1) the peak of
463
464
LONDON AND YOBKE
DISCUSSION
The mean monthly contact rates for measles, chickenpox and mumps that are estimated from reported monthly cases show
substantial seasonal variation (figure 2).
This cyclic variation is large relative to the
variation from year to year. The shape of
the curve of mean monthly contact rates
does not change significantly when the contact rates are computed from a wide choice
of values for the incubation period, the
infectious period or the level of susceptibles.
The curve of the mean monthly contact
rate for measles in Baltimore is almost
identical to the curve for measles in Xew
York City. The increased contact rate in
the autumn and winter months for measles,
chickenpox and mumps suggests that this is
an essential feature of any realistic model
of recurrent outbreaks of these diseases in
cities. Comparison of the contact rate of
polio (that has a relatively short incubation
period) with the contact rate of infectious
hepatitis (that has a relatively long incubation period) would be useful in understanding the seasonal variation of these diseases.
Because the absolute values of the mean
monthly contact rates are inversely proportional to the level of susceptibles, which is
difficult to determine, the absolute values of
the mean contact rates are not a reliable
measure of the actual number of contacts
made by an infective per day or of the
infectiousness of the three diseases. A valid
measure of infectivity is discussed in a
subsequent paper (11).
The cause of the seasonal variation in the
contact rates. What accounts for the seasonal variation in the contact rate? The
contact rate is affected by two classes of
factors: first, climatic factors that might
enhance the transmission of infectious diseases, such as cold weather, decreased indoor relative humidity, or possibly
decreased resistance to infectious diseases
during colder months, and second, the social
behavior of children aged 4—15, who presumably make more contacts when they are
in school.
The sharp rise and fall in the graph of
the mean monthly contacts for all three
diseases (figure 2) coincide with the opening and closing of school. The mean
monthly contact rate for measles that is
estimated from the reported cases from the
low years (figure 1 in reference 11)) is
approximately constant during the school
year. These features suggest that the increased contacts made by children in school
are the main cause of the seasonal variation
in the monthly contact rates. In addition,
the contact rate is high during the colder
months when, both in school and in the
home, children spend more time indoors
with each other. Data of weekly or biweekly notifications might show drops in
the contact rate due to holiday vacations
from school, but the monthly totals analyzed here did not. For the years and cities
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
increase in the contact rate for all months)
biennial outbreaks are simulated but the
ratio of high year to low year cases is about
8:1; with a 20 per cent increase in inf ectivity too many cases occur when susceptibles
are plentiful and the outbreak is not sustained in succeeding years. If the infectivity is decreased by 10 per cent (modeled by
a 10 per cent decrease in the contact rate for
all months) biennial outbreaks are simulated but the ratio of cases is only 3:1; an
18 per cent decrease in infectivity yields
simulations of annual outbreaks.
Siviulations of outbreak of chickenpox
and mumps. Simulations with mean
monthly contact rates for chickenpox (figure 2) reproduce the pattern of outbreaks in
New York City, annual outbreaks that
peak in February and March (figure 3).
Simulations with the mean monthly contact
rate for mumps (figure 2) show annual
outbreaks that peak in March (figure 3). If
the mean monthly contact rate for mumps
(calculated with Tx = 16) is used in a
simulation with Tx = 12, annual outbreaks
are still simulated; this shows that a shortened incubation period is.not sufficient to
.simulate biennial outbreaks of mumps.
OUTBREAKS OF MEASLES, CHICKENPOX AND MUMPS. I.
ishing susceptibles in the succeeding low
year is not sufficient to explain the biennial
pattern.
Biennial outbreaks. A second question is
why the annual variation in the contact
rate produces annual outbreaks of chickenpox and mumps but biennial outbreaks of
measles. As suggested by the simulations,
biennial outbreaks of measles occur because
the disease is sufficiently contagious and has
a brief enough incubation period that sufficiently many cases occur when susceptibles
are plentiful to deplete substantially the
population of susceptibles. In comparison
with chickenpox and mumps, the relatively
small population of susceptibles to measles
reflects the contagiousness of the disease.
Indeed, an urban resident had almost no
chance of escaping measles by age 20, but
about one chance in three of not contracting
chickenpox and one chance in two of not
contracting mumps (15). In the simulations
of measles outbreaks, the susceptible population is depleted in a high year by 40 per
cent; in a low year by 7 per cent. In
contrast, the population susceptible to
chickenpox and mumps is depleted annually
by less than 10 per cent. If in the calculation of the monthly contact rate the number
of susceptibles at the peak of the outbreak
(Sp) is increased by 20 per cent, the susceptible population is too large, the depletion
during a high year is less and only annual
outbreaks appear in the simulations. Conceivably, a three-year pattern could be
established (and has been observed in Baltimore and elsewhere (25)) in which two
years are needed to replenish the susceptibles; if, however, too many cases occur in a
high year the susceptibles and then the
infectives subsequently become depleted so
that, without the introduction of extra infectives, the disease dies out. Contrary to
findings based on another model (26), that
small changes in infectivity do not affect
periodicity, 5 per cent changes in the infectivity are enough to change substantially
the ratio of cases in the high and low years,
and an 18 per cent decrease in the infectiv-
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
for which we have data, apparently there
were no instances when, except during the
summer, school was closed for more than a
month. In England and Russia, however,
disruption in the usual pattern of school
attendance during World War II, altered
the seasonal and biennial patterns of the
outbreaks of measles (21-23). The Russian
workers (23) present other evidence including different seasonal incidences of measles
between urban and rural populations, to
show that the critical factors are social and
not climatic. Finally, Hope Simpson (24)
measured the infectiousness or contagiousness of measles, chickenpox and mumps in
households during all months of the year.
(In that study the infectiousness was defined as the proportion of exposures of
susceptibles in the home leading to transmission of the disease.) In the home the
infectiousness of the three diseases showed
no seasonal variation. For these reasons, the
seasonal variation in the contact rate is
attributed to social factors, particularly the
gathering of children in school.
The necessity of seasonal variation in the
contact rate. For the delay equation model
studied here, if a simulation is to give
undamped recurrent outbreaks that peak in
the spring, the contact rate £(£) must have
seasonal variation. Computer simulations in
which the contact rate is constant and
susceptibles are added equally throughout
the year show waves of outbreaks of ever
decreasing amplitude and the disease approaches a constant endemic level in society. Simulations in which the contact rate
is constant but susceptibles are added only
at the beginning of the disease year do not
show cyclic outbreaks that peak in the
spring. Although time delays in ordinary
differential equations often introduce oscillatory or even periodic solutions, if the
contact rate is constant, the delays of at
most 20 days are insufficient to produce
cyclic annual or biennial outbreaks. The
idea, for example, that undamped biennial
outbreaks can occur merely by depleting
susceptibles in a high year and then replen-
465
466
LONDON AXD YOHKE
measles but that has an incubation period
of three days show that the peak of the
outbreak occurs in the early winter, after
which the outbreak dies out. The peak of
the outbreaks of influenza, which has an
incubation period of at most three days,
occurs in the late autumn or winter (18).
Non-uniform use of the measles vaccine.
The model can be used to simulate widespread use of, for example, the measles
vaccine, by introducing fewer susceptibles
annually into the population. To model
uniform use of the vaccine, the original
monthly contact rate is used (because the
total population is unchanged); the simulations show annual outbreaks. To model
nonuniform use of the vaccine, that is, a
subpopulation that has not received the
vaccine, the monthly contact rate is increased proportionally (because the total
population is smaller); the simulations
show biennial outbreaks. The persistence of
the biennial pattern of measles outbreaks in
spite of widespread use of the vaccine, at
least in Chicago (27) and New York City
(figure 1) suggests nonuniform use of the
vaccine. The simulations suggest the existence of a subpopulation that is not receiving the vaccine and that is depleted
substantially after an outbreak. Indeed, the
preschool population interacts socially with
itself and represents a larger percentage of
the cases than was previously true (27, 28).
The replacement of the biennial pattern by
annual outbreaks suggests uniform use of
the vaccine. With nonuniform use of the
vaccine, immunes should not be counted in
the total population, and, as noted by others (8), the concept of herd immunity does
not apply to the pockets of susceptibles
within an otherwise totally immune urban
population (29).
REFERENCES
1. Serfling RE: Historical review of epidemic
theory. Hum Biol 24:145-166,1952
2. Bailey NTF: The mathematical theory of
epidemics. New York, Hafner, 1957
3. Soper HE: The interpretation of periodicity in
disease prevalence. J R Stat Soc 92:34-73, 1929
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
ity yields simulations of annual outbreaks.
Although the infectivity of each disease is
difficult to determine, chickenpox is apparently 35-65 per cent and mumps 19-^42 per
cent as infectious as measles in society
(11). Finally, to simulate biennial outbreaks in which the ratio of high year to
low year cases is the observed ratio of 5:1,
the mean duration of the incubation period
must be 12 to 13 days. A longer incubation
period (e.g., 16 days) yields simulations of
annual outbreaks, and with a shorter incubation period too many cases occur when
susceptibles are plentiful and the disease
dies out.
The simulations show, therefore, that
measles is in a narrow border region between "highly efficient" and "less efficient"
infectiou3 diseases. The hypothetical
"highly efficient" diseases are highly infectious, have brief incubation periods (fewer
than 12 days), deplete substantially the
susceptible population during an outbreak
and thus are not endemic in cities. Because
a disease that is not endemic in cities would
probably fail to perpetuate itself, there
appears to be no example of a hypothetical
"highly efficient" disease. An infectious disease that has a brief incubation period but
a low contact rate would not be "highly
efficient" and could be endemic in cities.
The "less efficient" diseases, such as chickenpox and mumps, are less infectious, have
relatively long incubation periods, do not
deplete substantially the susceptible population during an outbreak and are endemic
with a pattern of recurrent annual outbreaks.
Outbreaks that peak in the spring. Incubation periods of at least 12 days also
explain why these outbreaks peak in the
spring months even though the contact rate
rises sharply in the autumn months. With a
"generation time" of about two weeks,
seven or eight months are needed to build
up the level of infectives and then deplete
the susceptibles until the outbreak can no
longer be sustained. Simulations of a disease that has the same contact rate as
467
OUTBREAKS OF MEASLES, CHICKENPOX AND MUMPS. I.
21.
22.
23.
24.
25.
26.
27.
28.
29.
population "susceptible" to measles, 1900-1931,
Baltimore, Md. Am J Hyg 17:613-636, 1933
Gunn W: Measles. Modern Practices in Infectious Fevers. Vol 2. Edited by HS Banks. New
York, PB Hoeber, 1951, pp 499-520
Butler W: Whooping cough and measles, an
epidemiological concurrence and contrast. Proc
R Soc Med 40:384-398, 1947
Guslits SV: Measles. A Course in Epidemiology. Edited by II Elkin. New York, Pergamon
Press, 1961, pp 353-362
Hope Simpson RE: Infectiousness of communicable diseases in the household (measles,
chicken pox, and mumps). Lancet 2:549-554,
1952
Emerson H : Measles and whooping cough. Am
J Public Health (Suppl) 27:1-153, 1937
Bartlett MS: The critical community size for
measles in the United States. J R Stat Soc
Series A 123 :37^4, 1960
Hardy CE, Kassanoff I, Orbach HG, et al:
The failure of a school immunization campaign
to terminate an urban epidemic of measles.
Am J Epidemiol 91:2S6-293, 1970
Landrigan PJ, Conrad JL: Current status of
measles in the United States. J Infect Disease
124:620-622, 1971
Scott H D : The elusiveness of measles eradication: insights gained from three years of
intensive surveillance in Rhode Island. Am J
Epidemiol 94:37-42, 1971
APPENDIX
Models
based on
1
ordinary
differential
equations. The incubation and infectious
periods can also be modeled by ordinary
differential equations that have no delays.
In the following three models the average
duration of the infectious state is 5 days. All
three models implicitly assume that the probability of an infective ceasing to be infectious by time t is independent of the duration
of his infectivity. Likewise, models two and
three assume that the probability of an individual ceasing to incubate the disease by
time t is independent of how long he has
incubated the disease. The first model assumes no incubation period, that is, an exposed individual immediately becomes infectious.
The equations of the first model are
dS/dt = -p(l)S(t)I(f)
+ y
dl/dt = p(t)S(t)I(t) - (l/5)/(0
(la)
(2a)
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
4. Abbey H : An examination of the Reed-Frost
theory of epidemics. Hum Biol 24:201-233,
1952
5. Bnrtlett MS: Deterministic and stochastic
models for recurrent epidemics. Proceedings of
the Third Berkeley Symposium on Mathematical Statistics and Probability. Berkeley and
Los Angeles, University of California Press,
1956, Vol 4, pp Sl-109
6. Wilson LO: AJI epidemic model involving a
threshold. Math Biosci 15:109-121, 1972
7. Ewy W, Ackerman E, Gatewood LC, et al: A
generalized stochastic model for simulation of
epidemics in a heterogeneous population
(model VI). Comput Biol Med 2:45-58, 1972
8. Fox JP, Elveback L, Scott W, et al: Herd
immunity: basic concept and relevance to
public immunization practices. Am J Epidemiol 94:179-189, 1971
9. Hoppensteadt F, Waltman P : A problem in
the theory of epidemics. II. Math Biosci
12:133-146, 1971
10. Bliss CI, Blevins DL: The analysis of seasonal
variation in measles. Am J Hyg 70:328-334,
1959
11. Yorke JA, London WP: Recurrent outbreaks
of measles, chickenpox and mumps. II. Systematic differences in contact rates and stochnstic effects, Am J Epidemiol 98:469-482,
1973
12. Yorke JA, London WP: (in preparation)
13. Summary of Vital Statistics 1968 The City of
New York. Published by the Department of
Health, The City of New York, 1968
14. Baltimore Health News 48:10. Published by
Baltimore City Health Department, 1971
15. Collins SD, Wheeler RE, Shannon RD: The
occurrence of whooping cough, chicken pox,
mumps, measles and German measles in 200,000
surveyed families in 28 large cities. Special
Study Series, No 1, Division of Public Health
Methods, NIH, USPHS, Washington DC, 1942
16. Wilson EB, Burke M: The epidemic curve.
Proc Natl Acad Sci USA 28:361-367, 1942
17. Chope H D : A study of factors that influence
reporting of measles. Virus and Rickettsial
Diseases. A Symposium held at the Harvard
School of Public Health, June 12-June 17,
1939. Cambridge, Harvard University Press,
1940, pp 283-308
18. Debre R, Celers, J (editors): Clinical Virology
(The Evaluation and Management of Human
Viral Infections). Philadelphia, WB Saunders
Company, 1970
19. Sartwell P E : The distribution of incubation
periods of infectious disease. Am J Hyg
51:310-318, 1950
20. Hedrich AW: Monthly estimates of the child
46S
LOXDOX AXD YORKE
Equation la is the same as Equation 2 of
the delay equation model.
The second model assumes an incubation
state W that has mean life of 6 days. The
equations are la and
dW/dt = 0(05(0/(0 ~ O./0)W(t)
(3a)
cll/dl
(4a)
= (1/0)1^(0 - (1/5)7(0
dWJdt = p(l)S(t)I(t) - Wx{t) (5a)
dWi/dt = H',_i(0 - Wi(t)
(6a)
i = 2, . . . r
dl/dt
= WT(t) - (1/8)1 (0
(7a)
For measles, in all three models 5 = 2
days, in model two, 6 = 12 days, and in
model three, r = 12.
The graph of the mean monthly contact
rates for measles that is calculated using
model one is irregular, has large unsystematic
differences between the contact rates calcu-
Downloaded from http://aje.oxfordjournals.org/ at Stanford Medical Center on September 15, 2013
A more complicated approximation to the
delay of the incubation period is to assume
a sequence of incubation states W\, . . . , Wr
each with a mean life of one day. The equations of model three are la and
lated irom the high and low years, and shows
no consistent seasonal variation. The mean
monthly contact rates for measles, calculated using models two and three, are very
similar to the contact rates calculated from
the delay equation model (figure 2). For
models two and three the simulations of the
measles outbreaks that use the seasonally
varying contact rates show biennial outbreaks but the ratio of high year to low year
cases is too low. For model two the ratio is
about 2.5; for model three the ratio is about
3.3.
In comparing the delay equation model
and the ordinary differential equation
models, the model that assumes no incubation state (model one) is too simplistic to
allow the calculation of realistic contact
rates. The models that assume an incubation
state (models two and three) yield realistic
contact rates but the simulations are not
satisfactory. Clearly, ordinary differential
equation models without delays that are
more complicated than model three can
approximate the incubation period, but the
simplest and most satisfactory model is the
delay equation model.