Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
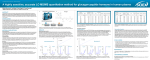
Bioscience Reports, Vol. I0, No. 1, 1990 Glycogenolytic Effect of Pancreastatin in the Rat Victor S a n c h e z , t J u a n R . Calvo I and R a i m u n d o G o b e r n a l'z Received October 13, 1989 Pancreastatin is a novel 49-amino acid peptide with a C-terminal glycine amide. The peptide was isolated from porcine pancreatic extracts and shows a structural similarity to chromogranin A. The effect of synthetic porcine pancreastatin on blood glucose levels and hepatic glycogen content was investigated in rats in vivo. Pancreastatin (300pmol/kg) produced a time-dependent decrease in glycogen content of liver and a slight hyperglycemia. Basal plasma insulin and glucagon levels were not modified by pancreastatin. We suggest that pancreastatin could play a biological role in the glucose metabolism through a glycogenolytic effect. KEY WORDS: glycogen; pancreastatin. INTRODUCTION Pancreastatin, a new 49-amino acid peptide with a C-terminal gylcine amide, was recently isolated from porcine pancreatic extracts by using the amide structure as a marker during the isolation procedure (1). Pancreastatin is widely distributed throughout the central nervous system (2) and in endocrine cells of the gastrointestinal tract, islets and exocrine cells of pig pancreas (3), and possesses a striking sequence homology with a part of bovine chromogranin A, a secretory glycoprotein widely distributed throughout the neuroendocrine system (4). It has been shown that pancreastatin inhibits glucose and arginine induced insulin release, from the isolated perfused pancreas (1, 5, 6). In the mouse, pancreastatin inhibits both glucose and carbachol induced insulin release, stimulates baseline glucagon secretion, and induces a slight hyperglycemia (7). However, the effects of pancreastatin in the rat under in vivo conditions have been very little studied. Thus, Funakoshi et al. have found that an intravenous infusion of pancreastatin inhibited the plasma insulin response to the intragastric infusion of glucose, and increased the plasma glucagon response to the intravenous infusion of arginine, but had not any effect on basal plasma insulin and glucagon concentrations (8). The aim of this study is to investigate, in vivo, the effect of pancreastatin on 1 Department of Medical Biochemistry and Molecular Biology School of Medicine, University of Sevilla, Auda Sanchez Pizjuan 4 41009, Sevilla, Spain. 2 To whom correspondence should be addressed. 87 0144-8463/90/0200-008750600/0~ 1990PlenumPublishingCorporation 88 Sanchez, Calvo and Goberna glucose metabolism. We show that pancreastatin causes hepatic glycogenolysis and hyperglycemia without altering basal plasma insulin and glucagon levels. MATERIALS AND METHODS Animals Male Wistar rats weighing 250-350 g were used. The animals were fed a standard diet ad libitum. The experiments were performed on anaesthetized animals (pentobarbital sodium, 50 mg/kg intraperitoneally) after a short-term fast (4-6 h) in the postabsortive state. Experimental Design Pancreastatin was obtained from Peninsula Laboratories Europe (Merseyside UK); glucagon was from Novo Biolabs (Bagsvaerd, Denmark); bovine serum albumin (BSA) from Sigma Chemical (St Louis, MO, USA). The peptides were dissolved in 0.9% NaCI-I% BSA to prevent adsorption to the syringe. Anaesthetized rats were injected intravenously in the superior mesenteric vein with porcine pancreastatin or porcine glucagon. The doses were 300 pmol/kg and the volume injected was l ml. Control rats were injected with 0.9% NaCI-I% BSA. Pieces of hepatic lobes from the same rat (caudate, left and right main lobes), weighing approximately 0.3 g, were tied off and rapidly excised before, at 10 and 20min after the injection and immediately processed to obtain the glycogen by alcoholic precipitation. Blood samples (0.9 ml) were taken from the jugular vein before, at 5, 10 and 20 min after the injection. The blood obtained was heparinized and 20/,1 were taken to measure blood glucose levels, the remaining blood was immediately centrifuged and plasma separated and stored at -20~ for insulin and glucagon determinations. Determinations ELISA (Enzyme linked immunosorbent assay, kit from Boerhinger Mannhein GmbH, FRG) was employed to measure plasma insulin. Radioimmunoassay (kit from Medgenix, Brussels, Belgium) was employed to measure plasma glucagon. Glycogen was determined by enzymatic conversion (amyloglucosidase from Boehringer Mannhein GmbH, FRG) to glucose which was determined by the glucose oxidase method. Blood glucose levels were also determined by this method. Student's t-test was used to test the degree of significance. RESULTS Effect of Pancreastatin and Glucagon on Hepatic Glycogenolysis The injection in the superior mesenteric vein of 300 pmol/kg of pancreastatin produced a decrease in glycogen content of liver. The basal content of hepatic GlycogenolyticEffectof Pancreastatin 89 '!= I I Fig. 1. Glycogenolysisafter the injection of pancreastatin (300pmol/kg; vertically striped bars), glucagon (300pmol/kg; horizontallystriped bars) or saline-BSA-l% (open bars) in the superior mesenteric vein. Means+ SEM are shown. *p < 0.05, **p <0.001 (n = 7), probabilitylevel of random differencebetween any group and the control group. o 0[ 20 10 Time (rain) glycogen was 51.3 + 5 mg/g liver. The results are expressed as the difference of glycogen concentration between the basal conditions and after the injection of saline-l%-BSA, glucagon or pancreastatin (Fig. 1). The glycogenolysis was significantly enhanced by pancreastatin at 10 min (7.8 4- 1.4 mg/g compared with 2.85: 1.4mg/g in controls, p < 0 . 0 5 ) ; the enhancement was comparable in magnitude to the increase caused by glucagon. At 20 rain the glycogenolysis was enhanced from 3.4 + 1 mg/g in controls to 12.2 + 1.2 mg/g (p < 0.001) in animals injected with pancreastatin. There were no significant differences between this group and the animals injected with glucagon. Effect of Pancreastatin and Glucagon on Baseline Levels of Blood Glucose, Plasma Insulin and Plasma Glucagon Blood glucose levels were significantly increased by pancreastatin (300 pmol/kg), with the peak at 5 min (Fig. 2). Thus, at 5 min after the injection, blood glucose levels were 4 . 3 + 0 . 2 m M in control rats and 5 . 1 + 0 . 2 m M in animals injected with pancreastatin (p <0.01). At 10rain the differences were still significant between controls (4.2 + 0.2 raM) and the animals injected with pancreastatin (4.8 + 0.1, p < 0.05). At 20 min, blood glucose levels did not differ from those in control rats. Blood glucose levels constantly increased after the injection of glucagon. At 5 rain there were no significant differences between this group and that injected with pancreastatin. At 10min the blood glucose levels were 6 . 2 + 0 . 2 m M (p < 0.001) and at 20 min they were 6.7 + 0.3 mM (p < 0.00l). Baseline levels of plasma insulin and glucagon levels were not significantly affected by injection of pancreastatin (Fig. 2). Glucagon slightly elevated basal plasma insulin levels. At 20 rain the increase was significant (34 + 7/~U/ml compared with 16 + 3/~U/ml in the control group, p < 0.05). After glucagon injection, the plasma glucagon levels were 720 + 70 pg/ml at 5 min, 330 + 50 pg/ml at 10 min and 180 + 38 pg/ml at 20 min. Sanchez, Calvo and Goberna 90 7 i i J i.~ I I I I 6 84 o ~, 5 ~.~ 4 ~E O~ 50 .E 40 = so x 20 0_.. 0 800 o, 600 92= E ~'~, 400 E-- 200 t 0... o I I I I 0 5 I0 20 Fig. 2. Blood glucose levels (top), plasma levels of insulin (middle) and glucagon (bottom) before and at various time points after the injectionof pancreastatin (300pmol/kg; e, n = 8), glucagon (300pmol/kg; 9 n =8) or saline-BSA-1% (A, n = 6). Means :I:SEM are shown. *p <0.05, **p <0.0t, ***p<0.001, probability level of random difference between any group and the control group. T i m e (rain) DISCUSSION This paper describes the effect of pancreastatin, in vivo, on the hepatic glycogen in rats. This 49-residue peptide with a C-terminal glycine amide was isolated from porcine extracts by Tatemoto et al. (1). Recently, Eiden (4) and Huttner and Benedum (9) independently drew attention to a striking similarity in amino acid sequence between porcine pancreastatin and a segment of the peptide chain of bovine chromogranin A. This similarity suggests a functional role of chromogranin A as a precursor of pancreastatin or pancreastatin-like peptide. Chromogranin A and its related proteins, chromogranin B and C and secretogranin I and II, are widely distributed throughout the neuroendocrine system and other tissues (10, 11, 12). Thus, the role of pancreastatin may not be limited to the pancreas. The foregoing results demonstrate that, in vivo, pancreastatin (300 pmol/kg) injected via the portal vein stimulates the hepatic glycogenolysis, and this effect could be direct since we have found no effect on basal insulin and glucagon levels. Other authors have studied the effect of pancreastatin (4 nmol/kg) in the mouse in v i v o ; Ahr6n et al. (7) have found that this peptide weakly inhibits insulin secretion and stimulates glucagon secretion. These contradictory results could be explained by the different animal species used, the different doses employed and the different experimental models. On the other hand, Lindskog et al. (13) reported that it slightly elevated basal plasma glucagon levels without altering basal plasma insulin. Recently, Funakoshi et al. (8) have Glycogenolytic Effect of Pancreastatin 91 found no effect of an intravenous infusion of pancreastatin (1 and 10 n m o l / k g / h ) on unstimulated insulin and glucagon release. H o w e v e r , unlike our study, they found no effect on the basal plasma glucose levels. This difference m a y result from the different metabolic situations, since they conducted the experiments after an overnight fasting (18-24 h) when the glycogen stores are almost depleted, and we suggest that the hyperglycemic effect is caused by glycogenolysis. The glycogenolysis caused by pancreastatin was c o m p a r a b l e to that caused by glucagon. The differences in the hyperglycemia caused by pancreastatin and glucagon could be explained by a different effect of pancreastatin on gluconeogenesis and glycolysis (it has not b e e n studied yet), whereas glucagon increases gluconeogensis as much as glycogenolysis (14) and inhibits glycolysis, in large part mediated by changes in the level of fructose-2,6-biphosphate (15). H o w e v e r , further studies are needed to clarify this point. ACKNOWLEDGEMENTS Supported by a G r a n t f r o m Comision Asesora de Investigaci6n Cientifica y T6cnica ( C A I C Y T no. 1106). V. Sanchez Margalet is a doctoral fellow of the University of Sevilla, Spain, sponsored by M o n t e de Piedad Y Caja de A h o r r o s de SeviUa. REFERENCES 1. Tatemoto, K., Efendi6, S., Mutt, V., Makk, G., Feistner, G. J. and Barchas, J. D. (1986) Nature 324: 476-478. 2. Gibson, S. J., Kars, S., Ballesta, J., Steel, J., Bretherton-Watt, D. G., Ghatei, M. A., Valentino, K. L., Tatemoto, K., Bloom, S. R. and Polak, J. M. (1987) Regul. Pept. 18:376 (Abstract). 3. Ravazzola, M., Efendi6, S., Ostenson, C. G., Tatemoto, K., Hutton, J. C. and Orci, L. (1988) Endocrinology 123:227-229. 4. Eiden, L. E. (1987) Nature, 325:325-301. 5. Efendic, S., Tatemoto, K., Mutt, V., Quan, C., Chang, D. and Ostenson, C. G. (1987) Proc. Natl. Acad. Sci. USA 42:1361-1367. 6. Silvestre, R. A., Peir6, E., Miralles, P., Villanueva, M. L. and Marco, J. (1988) Life Sci. 42:1361-1367. 7. Ahr6n, B., Lindskog, S., Tatemoto, K. and Efendic, S. (1988) Diabetes 37:28t-285. 8. Funakoshi, A., Miyasaka, K., Kitani, K. and Tatemoto, K. (1989) Regul. Pept. 24:225-231. 9. Huttner, W. B. and Benedum, U. M. (1987) Nature (London) 325:305. 10. O'Connor, D. T. (1983) Regul. Pept. 6:263-280. 1i. Rindi, G., Buffa, R., Sessa, F., Tortora, O. and Solcia, E. (1986) Histochemistry 85:19-28. 12. Grube, D., Aunis, D., Bader, F., Cetin, Y., J6rns, A. and Yoshie, S. (1986) Histochemtstry 85:19-28. 13. Lindskog, S. and Ahr6n, B. (1988) Hormone Res. 29:237-240. 14. Stevenson, R. W., Steinert, K., Davis, M. A., Hendrick, G. K., Williams, P. E., Lacy, W. W., Brown, L., Donahue, P., Lacy, D. B. and Cherrington, A. D. (1987) Diabetes 36:382-389. 15. EI-Maghrabi, M. R., Claus, T. H., Pilkis, et al. (1982)J. Biol. Chem. 257:7603-7607.