Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
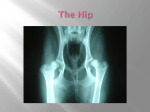
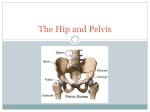
Hip and Pelvis Chapter 19 Hip & Pelvis Strongest articulation in body Most stable articulation Well protected & surrounded by muscle on all sides Muscles of back, abdomen, hamstrings, quadriceps, abductors, adductors, and gluteals attach Freely moveable, ball-and-socket Function of Pelvis Transmit weight from axial skeleton to LE when standing or to ischial tuberosities when sitting Provides attachments for various muscles that insert onto and control LE House parts of digestive and urinary tract Houses reproductive systems Pelvis—Skeletal Structure Ilium Sacrum Ischium Obturator foramen Pubis Iliac crest Greater sciatic notch Iliac fossa Pubic Symphsis Coccyx Pelvis—Skeletal Structure Anterior Superior Iliac Spine (ASIS) Anterior Inferior Iliac Spine (AIIS) Posterior Superior Iliac Spine (PSIS) Ischial Tuberosity Greater Sciatic Notch Obturator Foramen Pelvis—Skeletal Structure Pelvis—Skeletal Structure Pelvis—Skeletal Structure Ischial Tuberosity Ischial Tuberosity Comparison of Male & Female Pelvis Male More dense Muscle attachments more sharply defined Female Smaller Shorter Wider Male versus Female Male Female Hip—Skeletal Structure Hip—Skeletal Structure Hip—Ligaments Iliofemoral Pubofemoral Ischiofemoral Primary Muscles of the Pelvis, Hip & Thigh Gluteal muscles Gluteus medius Gluteus minimus Gluteus maximus Hip flexors Iliopsoas Psoas Major/Minor Sartorius Pectineus Rectus femoris Adductors Adductor longus Adductor brevis Adductor magnus Hamstrings Biceps femoris Semimembranosus semitendinosus Primary Muscles of the Pelvis, Hip & Thigh Gluteal Muscles Hip extension Internal rotation External rotation Abduction Hip Flexor Muscles Hip Flexor Muscles Adductor Muscles Iliotibial Band Thickening of the fascia Runs up outside of thigh Top of hip & crosses knee Holds our leg straight when we stand, giving the larger thigh muscles a chance to rest Tensor Fasciae Latae (TFL) Common Injuries and Conditions Of The Hip and Thigh Bursitis Most frequent location is over lateral hip Greater trochanteric bursitis Tenderness lateral hip Made worse by walking, running, or twisting hip Insufficient stretching or warm-up Treatment: Limit activity Stretching exercises Ice & ice massage NSAIDs Fracture 3 classifications: Femoral neck Intertrochanteric Subtrochanteric Causes: Falling (elderly) Extreme trauma (car accidents) Impact injury (athletics) Signs & Symptoms Leg may appear abnormally rotated Cannot move hip without pain X-ray to confirm Treatment Depends on fracture type and medical condition Fracture Quad & Hip Flexor Strain Common in those sports that require jumping, kicking, or repetitive sprinting Quad: rectus femoris Hip Flexor: rectus femoris and/or iliopsoas Treatment Ice Compression NSAIDs Rehab Progressive Sport specific Hamstring Strain Causes Sudden, explosive starts and stops Chronic overuse Making quick start or stop when leg extended Overtraining (fatigued hamstring muscles) Muscle imbalance (quad muscles overdeveloped) Inflexibility Overstretched Insufficient warm-up, stretching, or conditioning Direct blow while muscles contracted Signs & Symptoms Sharp pain (most common in belly of muscle) Bruising Swelling Loss of strength Feel or hear “pop” Hamstring Strain Treatment RICE Medication Physical therapy/rehab Crutches Massage Rehabilitation Progressive Weight-training Preventative Proper stretching Recovery Time Mild: 2-10 days Moderate: 10 days-6 weeks Severe: 6-10 weeks Adductor Strain MOI: sudden sideways change in direction Skating Soccer Track & field Tennis Adductor longus Treatment: Difficult to treat Risk of re-injury is high Rest, ice, anti-inflammatory meds Stretching & strengthening exercises Iliotibial Band Syndrome Lateral knee pain Pain worse after running Especially after climbing hills/stairs Often not present until midway through run Associated with “snapping hip” Attributed to: Over-training Doubling mileage Increase in hill repeats Running on uneven roads Tight indoor tracks Poor running shoes Treatment Address faulty pelvic mechanics Reduce or stop running Cross-train Ice Stretch Gluteals and TFL Self-massage outside thigh and/or gluteals Address faulty foot mechanics, running shoes, or orthotics Return to running gradually Quadriceps Contusion Direct blow to thigh from helmet or knee Limit motion Affect gait Severity graded by ROM at time of injury Treatment Football, rugby, soccer, basketball Immediate compression, ice, NWB Massage contraindicated Recovery Time: 2 days to 6 months Complication: Myositis Ossificans Myositis Ossificans Ossifying mass (calcium deposit) forms within the muscle Result of recurrent trauma to quad muscle that was not properly protected after mild injury Signs & Symptoms Hard, painful mass in soft tissue Progressive loss of knee flexion X-ray at four weeks Treatment Heat Limit joint motion Rehab exs limit pain Discouraged 6months: Passive stretching Vigorous exercise Calcium reabsorbtion may take 3-6 months Myositis Ossificans Iliac Crest Contusion “hip pointer” Caused by direct blow to hip Common in football due to improperly fitted hip pads Signs & Symptoms: Treatment Extreme tenderness Swelling Ecchymosis Ice, compression Pad injured area RTP: dictated by athlete’s pain level Iliac Crest Contusion Overuse Injuries MOI: cumulative effects of very low levels of stress Chronic muscle strains Stress fractures Tendonitis Repetitive action of running Overuse/overload fatigue within the tendon Snapping hip Iliopsoas tendon snapping over the head of the femur Bursitis CROSS-TRAINING Stress Fractures Pelvis: occur most often in runners & dancers Femur: occur usually in runners Signs/Symptoms: Chronic, ill-defined pain over groin and thigh Initially diagnosed with muscle strain Symptoms do not resolve with rest & rehab Treatment: Rest Non-weight-bearing endurance exercises Stress Fractures Stress Fractures