Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
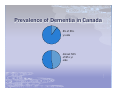
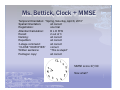
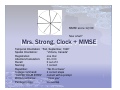
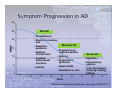
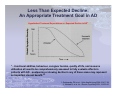
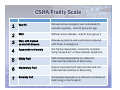
Cognitive Screening in Primary Care Marilyn Malone, MHSc, MD, FRCPC Geriatric Medicine March 18, 2015 Objectives Know how to define and differentiate mild cognitive impairment from dementia syndromes. Better understand the use of and interpretation of common cognitive screening tools Cognitive Screening in Primary Care What is dementia? What is mild cognitive impairment (MCI)? Who is at risk? Tool kit Mini-Cog Clock drawing MoCA MMSE Case examples What is Dementia? Demonstrable impairment of memory (DSM-4) Other impairment in at least one of: Language (naming) Judgment / executive function Construction / visuospatial function Abstraction Personality Impairment interferes with function and ADL Insidious, and > 6 months (ICD-10) What is Dementia? DSM 5: neurocognitive disorder Mild Moderate Severe Dementia IS NOT a test score Collateral history is crucial … Prevalence of Dementia in Canada 8% of 65+ yr olds Almost 50% of 85+ yr olds Who is at risk? Age Family Hx Risk doubles every 5 yrs Risk doubles for each 1st degree relative Cardiovascular disease Risk doubles for each vascular risk factor Risk ≥ 15% justifies cognitive assessment. AGE % <65 1 65 2 70 4 75 8 80 16 85 32 Case #1: Mr. A. Phib You have known Mr. A. Phib, age 65, for about 3 years. He missed his last 2 routine appointments, and you have concerns since it has been more difficult to titrate his INR. You wonder if he stopped taking his warfarin as prescribed. He has never complained about memory, and has no family. You wonder if he should have his memory checked. He comes in for a 15 minute appointment. What next? Mr. Phib, age 65, 1 vascular risk factor AGE % <65 1 65 2 70 4 75 8 80 16 85 32 Dementia risk is 2 x 2 = 4% Due to low calculated risk, a full cognitive assessment isn’t usually indicated. Therefore, you decide to do a “Mini-Cog” rather than an MMSE. Mr. Phib, Mini-Cog Scenario 1: Step 1: Register 3 words Step 2: Draw a clock Step 3: Word recall Step 4: Score Remembers 1 of 3 words Normal clock, 1/3 words = negative screen for dementia Mr. Phib, Mini-Cog Scenario 2: Step 1: Register 3 words Step 2: Draw a clock Step 3: Word recall Remembers 2 of 3 words Step 4: Score Abnormal clock, 2/3 words = positive screen for dementia Collateral history is crucial … Case #2: Ms. Diane Bettick Ms. Diane Bettick, age 60, is well known to you, and has been your patient for 20 years. She used to be a hospital administrator and has been enjoying “the good life” since retiring 4 years ago. She is an avid golfer and sometimes you see her forcing her clubs into the tiny trunk of her convertible after finishing a round. She has Type 2 DM with HbA1C of 6.8%, controlled HTN with BP 124/80, stable ischemic heart disease, lipids well controlled on atorvastatin. You have never worried about her cognition, but her husband says she is having difficulty managing money. Also, he thought she seemed confused and overwhelmed at the Heathrow airport when they went to visit relatives over Christmas. She comes in for a 15 minute appointment without her husband. What next? Ms. Bettick, age 60, 4 vascular risk factors AGE % <65 1 65 2 70 4 75 8 80 16 85 32 Dementia risk is 1 x 2 x 2 x 2 x 2 = 16% Due to high calculated risk, you decide to do a full screening test. What test do you do? Ms. Bettick, Mini-Cog: Step 1: Register 3 words Step 2: Draw a clock Step 3: Word recall Remembers 2 of 3 words Step 4: Score Abnormal clock, 2/3 words = positive screen for dementia Ms. Bettick MoCA score 18/30 Now what? Does she have a dementia or not? Ms. Bettick, Clock + MMSE Temporal Orientation: “Spring, Saturday, April 8, 2010” Spatial Orientation: all correct Registration: one trial Attention/Calculation: DLORW Recall: 2 out of 3 Naming: all correct Repetition: all correct 3-stage command: all correct “CLOSE YOUR EYES” correct Written sentence: “This is stupid” Pentagon copy: all correct MMSE score 27/30 Now what? Ms. Bettick, next steps She failed the Mini-Cog, MMSE 27/30, MoCA 18/30 Collateral information from husband suggests there is functional impairment (finances, travelling) You correctly conclude that she has an early dementia What about driving? What about more investigations? What about treatment? Case #3: Miss Ida Frett Miss Ida Frett is a new patient to you. She is a retired school librarian, lives alone, and takes the bus to church on Sundays. She takes various vitamins and herbal remedies but no other medications. She is terribly worried that she has early Alzheimer’s disease and wants to get “checked out.” Both parents had Alzheimer’s in their late 80’s, and she just turned 84. What next? Miss Frett, age 84, no vascular risk factors, both parents had AD AGE % <65 1 65 2 70 4 75 8 80 16 85 32 Dementia risk is 16 x 2 x 2 = 64% Due to high calculated risk, you decide to do a full screening test. What test do you do? Miss Frett, Clock + MMSE Temporal Orientation: “Spring, Saturday, April 10, 2010” Spatial Orientation: all correct Registration: one trial Attention/Calculation: DLROW Recall: 3 out of 3 Naming: all correct Repetition: all correct 3-stage command: all correct Written sentence: “You are the best doctor in the world” Pentagon copy: all correct MMSE score 30/30 Now what? Miss Frett MoCA score 25/30 Now what? Does she have a dementia or not? Miss Frett You correctly determine that she has MCI Her specific risk for dementia is: 12% per year 50% at 5 years At 5 years, she has a 30% chance of being the same, and a 20% chance of improvement without intervention You ask your nurse to recheck the MoCA in 6 months. Case #4: Mrs. Ima Strong Mrs. Strong is an 86 year old lady with known dementia and frequent falls. Her 90 year old husband brought her in for an annual checkup – you hear Ima yelling at him in the waiting room. Last year she scored 23/30 on an MMSE, and you recommended home supports that she promptly fired. She doesn’t take any medications except Ativan for sleep. Both Ima and her husband Ernest look exhausted. Ima looks thin and disheveled, and Ernie is trying not to cry. What next? MMSE score 12/30 Now what? Mrs. Strong, Clock + MMSE Temporal Orientation: “Fall, September, 1929” Spatial Orientation: “Victoria, Canada” Registration: one trial Attention/Calculation: DLOD Recall: 0 out of 3 Naming: 1 correct Repetition: “No ifs or buss” 3-stage command: 2 correct steps “CLOSE YOUR EYES” correct with a prompt Written sentence: “I love you” Pentagon copy: no overlap Mrs. Strong You are very worried about Ernie’s health and Ima’s outbursts of rage You identify verbal aggression as a key target symptom for treatment. You realize Ativan is a problem, but you also know that atypical antipsychotics such as risperidone can double mortality in demented patients You refer Ima for specialist assessment Symptom Progression in AD 30 25 Mild AD Forgetfulness 20 Short-term memory loss Moderate AD MMSE Repetitive 15 questions Progression of cognitive deficits Hobbies, interests lost 10 Impaired Agitation Dysexecutive instrumental functions 5 Severe AD Aphasia Altered sleep patterns syndrome Impaired Anomia ADL Transitions Total in care 0 1 2 3 4 5 Years 6 7 dependence: dressing, feeding, bathing 8 9 Adapted from Feldman & Woodward. Neurology. 2005;65:S10-7. Management of Patients with Dementia 1. Define specific target symptoms A. B. C. 2. 3. 4. ADL/IADL: e.g. household chores BEHAVIOUR: agitation/aggression/apathy COGNITION: memory, language, executive function Consider rational pharmacologic treatment Ensure non-pharmacologic management Caregiver support, family education Less Than Expected Decline: An Appropriate Treatment Goal in AD Hypothetical Treatment Expectations vs. Expected Decline in AD1 “…functional abilities, behaviour, caregiver burden, quality of life, and resource utilisation all need to be comprehensively assessed to fully evaluate effects in patients with AD…postponing or slowing decline in any of these areas may represent an important clinical benefit.”2 1. Geldmacher DS, et al. J Nutr Health Aging 2006;10:417-29; 2. Winblad B, et al. Int J Geriatr Psychiatry 2001;16:653-66. Dementia IS NOT a test score Key Points Dementia: IS loss of function due to cognitive loss IS NOT a test score Screen those at risk: 2 x 2 rule Identify target symptoms: A, B, C Consider non-pharmacologic and pharmacologic treatments First Link Medical Management of Patients with Dementia: avoid Pitfalls Recommended Guidelines for Treatment of a chronic disease may no longer apply. 1. Diabetes Hypertension Simplify medications as much as possible 2. 3. 4. Specialized diets Avoid multiple doses, anticholinergics, benzodiazepines Consider frailty and its impact on medical/surgical management and prognosis What is important to the patient? CSHA Frailty Scale 1 Very fit Robust/active/energetic/well motivated/fitexercise regularly - most fit group for age 2 3 Well Without active disease - less fit than group 1 Well, with treated co-morbid disease Disease symptoms well controlled compared with those in category 4 4 Apparently vulnerable Not frankly dependent, commonly complain being “slowed up” or have disease symptoms 5 Mildly Frail With limited dependence on others for instrumental activities of daily living 6 Moderately Frail Help is need with both instrumental and noninstrumental activities of daily living 7 Severely frail Completely dependent on others for activities of daily living, or terminally ill