Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
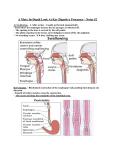
Absorption from different intestinal segments during exercise G. P. LAMBERT, R. T. CHANG, T. XIA, R. W. SUMMERS, AND C. V. GISOLFI Departments of Exercise Science and Internal Medicine, University of Iowa, Iowa City, Iowa 52242-1111 duodenum; jejunum; fluid balance; fluid absorption; solute absorption of fluid homeostasis during prolonged exercise is the ability to absorb ingested fluids (19), which occurs primarily in the proximal small intestine (duodenojejunum). Segmental perfusion is the most accepted technique for study of intestinal absorption of different solutions (47); however, the results only apply to the segment studied. Previous investigations (1, 17, 21–23, 26, 29, 39, 41, 46, 54) have differed in the site of perfusion (e.g., duodenojejunum, jejunum, ileum), which has led to difficulty in comparing results and drawing conclusions regarding the efficacy of various solutions. Furthermore, caution must be exercised in applying the results of direct perfusion studies to what would occur if the same solution were orally ingested. Recently, we developed a technique to simultaneously determine both gastric emptying (GE) and AN IMPORTANT ASPECT 204 intestinal absorption (28). This technique allows determination of intestinal water and solute flux, while also accounting for individual GE rates and alterations made by the stomach to the solution after its oral ingestion. This technique was employed in the present investigation to determine whether different segments of the proximal small intestine absorb water and nutrients at different rates. In humans, the duodenum is defined as the portion of intestine from the pyloric sphincter to the ligament of Treitz and is 20–30 cm in length (10, 33). It is highly permeable and presumably the site of maximal fluid movement between the alimentary canal and the blood. It is often cited as the intestinal segment responsible for bringing chyme from the stomach to isotonicity (51). Most segmental perfusion studies bypass this segment and typically evaluate jejunal function beyond the ligament of Treitz. If the purpose of performing segmental perfusion in the jejunum is to evaluate the efficacy of ingesting the same solution, such an extrapolation may be inaccurate. In contrast to the duodenum, the jejunum consists of a less leaky mucosal epithelium with a significantly greater ability to absorb glucose (24). Results of a pilot study from this laboratory (Fig. 1) indicate significantly greater fluid absorption with ingestion of a water placebo (WP) compared with an isotonic 6% carbohydrate-electrolyte (CHO-E) beverage in the duodenum. This contrasts with previous findings (22, 23) in which primarily the jejunum was studied by the segmental perfusion technique. From these data, we questioned whether segmental differences exist for fluid and solute absorption. Given the large osmotic gradient between water and blood, we hypothesized that absorption of water would be greater in the duodenum (first 25 cm) compared with an isotonic solution. In the jejunum (second and third 25-cm segments), where membrane resistance is greater than in the duodenum but where glucose transport is enhanced (24), we hypothesized an isotonic CHO-E beverage would have an absorptive advantage over deionized water because of CHO absorption and subsequent ‘‘solution drag.’’ To test these hypotheses, we studied water and solute absorption of two different solutions (a deionized WP and an isotonic CHO-E solution) in three consecutive segments of the proximal small intestine (,0–25, 25–50, and 50–75 cm distal to the pyloric sphincter). MATERIALS AND METHODS Six healthy men and one woman [age 26.0 6 9.0 yr; peak oxygen consumption (V̇O2 peak) 5 53.5 6 6.5 ml · kg21 · min21] participated in this study, which conformed to all the rules and regulations of the University of Iowa Human Use Commit- 0161-7567/97 $5.00 Copyright r 1997 the American Physiological Society http://www.jap.org Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 18, 2017 Lambert, G. P., R. T. Chang, T. Xia, R. W. Summers, and C. V. Gisolfi. Absorption from different intestinal segments during exercise. J. Appl. Physiol. 83(1): 204–212, 1997.—This study evaluated intestinal absorption from the first 75 cm of the proximal small intestine during 85 min of cycle exercise [63.6 6 0.7% peak O2 consumption (V̇O2 peak)] while subjects ingested either an isotonic carbohydrateelectrolyte beverage (CHO-E) or a water placebo (WP). The CHO-E beverage contained 117 mM (4%) sucrose, 111 mM (2%) glucose, 18 meq Na1, and 3 meq K1. The two experiments were performed a week apart by seven subjects (6 men and 1 woman; mean V̇O2 peak 5 53.5 6 6.5 ml · kg21 · min21 ). Nasogastric and multilumen tubes were fluoroscopically positioned in the gastric antrum and duodenojejunum, respectively. Subjects ingested 23 ml/kg body weight of the test solution, 20% (383 6 11 ml) of this volume 5 min before exercise and 10% (191 6 5 ml) every 10 min thereafter. By using the rate of gastric emptying (18.1 6 1.1 vs. 19.2 6 0.7 ml/min for WP and CHO-E, respectively) as the rate of intestinal perfusion, intestinal absorption was determined by segmental perfusion from the duodenum (0–25 cm) and jejunum (25–50 and 50–75 cm). Water flux was different (P , 0.05) between solutions in the 0- to 25- and 25- to 50-cm segments for WP vs. CHO-E (30.7 6 2.7 vs. 15.0 6 2.9 and 3.8 6 1.1 vs. 11.9 6 3.3 ml · cm21 · h21, respectively). Furthermore, water flux differed (P , 0.05) for WP in a comparison of the 0- to 25- to the 25- to 50-cm segment. Total solute flux (TSF) was not significantly different among segments for a given solution or between solutions for a given segment. There was no difference between trials for percent change in plasma volume. These results indicate that 1) fluid absorption in the proximal small intestine depends on the segment studied and 2) solution composition can significantly effect water absorption rate in different intestinal segments. 205 ABSORPTION FROM DIFFERENT INTESTINAL SEGMENTS DURING EXERCISE tee. Each subject gave signed informed consent and received a physical examination before participation. V̇O2 peak was determined by using a graded protocol on an electronically braked cycle ergometer (The Bike, Cybex, Ronkonkoma, NY). Expired gases and ventilation were analyzed with a Q-Plex I metabolic system (Quinton Instruments, Seattle, WA). A workload corresponding to 60–65% V̇O2 peak was subsequently determined and served as the exercise intensity for the experimental trials. Subjects followed a controlled diet for 16–18 h before each experiment and were asked to limit their physical activity during this time to control preexperiment glycogen levels. The morning of an experiment, the subject arrived at the University of Iowa Hospitals and Clinics at ,5 AM after an overnight fast (at least 8 h) and was orally intubated with a nasogastric (NG) tube (50 in., 14 Fr, Levin) into the gastric antrum and a multilumen tube (construction described below) into the duodenojejunum. During tube placement the subject ingested water (,400–500 ml) to facilitate movement of the tubes and to control for preexperiment hydration status. The NG tube was attached to the multilumen tube with a small piece of thin rubber tubing so that its distal tip was 9 cm from the proximal sampling site of the multilumen tube. The rubber tubing was located 7 cm from the distal tip of the NG tube to allow the NG tube to separate from the multilumen tube in the stomach without passing into the duodenum. Tube placement was verified fluoroscopically, and contrast medium [Hypaque sodium 50%; a brand of diatrizoate sodium injection (USP)] was injected through the proximal sampling port during placement of the tube to ensure that the tube was positioned correctly. When both tubes were in position, the most proximal port of the multilumen tube was located ,5 cm from the pyloric sphincter, and the NG tube was positioned in the distal antrum. During positioning of the tubes, an 18-gauge, 13⁄4-in. catheter was placed in a superficial arm vein for blood sampling. Determination of Stomach Volume, GE Rate, and Gastric Secretion Stomach volume was determined every 10 min by using a modified version of the repeated double-sampling techniques described by George (18) and modified by Beckers et al. (2). Gastric secretion was calculated on the basis of the formula of Murray et al. (35) in accordance with Beckers et al. (2). Briefly, the procedure involves obtaining 5-ml gastric samples and injecting 15 ml of PR (200 mg/l) every 10 min with a 70-ml Toomey syringe. The technique is as follows: 1) a gastric sample is obtained; 2) PR is injected, mixed thoroughly with the stomach contents, and another sample is obtained; and 3) the subject ingests the test solution, the new stomach contents are mixed, and a final sample is drawn. The samples obtained in steps 1–3 are used to calculate stomach volume and gastric secretion every 10 min as follows Stomach volume (ml) 5 PRvol 3 PRinj 2 PRafter add PRafter add 2 PRbefore add where PRvol is volume of PR injected every 10 min, PRinj is the concentration of PR injected, PRafter add is the concentration of PR in the stomach contents after PR is added and mixed well, and PRbefore add is the concentration of PR in the stomach before PR injection. Gastric secretion is calculated as GS10 5 stomach volume 3 [1 2 (PR10 /PR0)] where GS10 is the volume of gastric secretion in the stomach contents after each 10-min period from the time a subject drinks to the time stomach volume is determined 10 min Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 18, 2017 Fig. 1. Individual data from a pilot study investigating water flux in first 25 cm of small intestine comparing a water placebo (WP) to an isotonic carbohydrate-electrolyte (CHO-E) beverage. Values are means 6 SE. Arrows, 7 of 8 subjects exhibited higher rates with a WP compared with CHO-E. After tube placement, the subject walked to the exercise physiology laboratory and sat for 20 min to allow plasma volume to equilibrate. After 20 min, blood and urine samples were collected, a rectal temperature (clinical thermometer), resting heart rate (heart rate monitor; Polar Vantage XL, Polar USA, Stamford, CT), and nude body weight were obtained, and the subject changed into cycling clothes. The subject then immediately mounted the stationary bike, and stomach contents were aspirated through the NG tube. After stomach aspiration, the subject drank an initial bolus of test solution equaling 20% of the total volume ingested (23 ml/kg body wt). The total volume averaged 1,914 6 191 ml, and the mean initial bolus was 383 6 37 ml. Five minutes after ingestion, the subject began cycling for 85 min. Each 10-min interval thereafter, an additional amount of test solution was ingested and equaled 10% of the total experimental volume (191 6 19 ml). The experimental solutions consisted of either a 117 mM (4%) sucrose, 111 mM (2%) glucose, 17.8 meq/l Na1, and 3.1 meq/l K1 beverage with an osmolality of 282 mosmol/kgH2O (i.e., CHO-E), or a deionized WP (osmolality 5 1.1 mosmol) flavored to match the CHO-E solution. Each solution also contained 1 mg/ml polyethylene glycol 3350 (PEG). The temperature of the solution, which was given to the subject in a clear graduated flask, was 10–15°C. Experiments were performed in a 22°C environment with a slight breeze (,2 ft /s) produced by a fan placed in front of the subject. Blood samples were drawn every 15 min to determine changes in plasma volume, osmolality, Na1, K1, and glucose. Heart rate was obtained every 15 min. Rectal temperature, nude body weight, and urine volume were recorded postexercise. Sweat rate was calculated from nude body weight change pre- to postexperiment corrected for fluid ingestion, phenol red (PR) injection, and stomach, intestinal, blood, and urine samples. 206 ABSORPTION FROM DIFFERENT INTESTINAL SEGMENTS DURING EXERCISE later. Stomach volume is that determined for the 10-min period under study, PR10 is the PR concentration in the stomach before the stomach volume is determined (after 10 min have elapsed since drinking), and PR0 is the PR concentration in the stomach immediately after the initial drink (10 min before). GE rate is derived by subtracting a given stomach volume from the volume that is in the stomach after the previous ingestion of beverage 10 min before. Determination of Intestinal Absorption by Segmental Perfusion Q̇E 5 GER · [PEG]s /[PEG]p 2 ṠP Q̇L 5 Q̇E · [PEG]p /[PEG]d Q̇N 5 Q̇L 2 Q̇E where GER is the gastric emptying rate; Q̇E is the flow rate entering a given segment (ml/min); Q̇L is flow rate leaving a given segment (ml/min); Q̇N is the net water movement across the wall of the segment of intestine studied (ml/min); ṠP is sampling rate from proximal collecting sites for each segment studied; and [PEG]s, [PEG]p, and [PEG]d are the concentrations of the nonabsorbable marker in the stomach, at the proximal site of a given segment, and at the distal site of a given segment, respectively. Individual segments along the total 75-cm test length (i.e., 25–50 cm and 50–75 cm) were calculated by subtraction after determination of flux in the 0to 25-, 0- to 50-, and 0- to 75-cm segments, respectively. Solute flux was calculated by multiplying the solute concentration at the proximal and distal sampling sites of the 0- to 25-, 0- to 50-, and 0- to 75-cm segments and by the flow rates entering and leaving these segments. Net movement of solute in these segments was determined by using the formulas of Cooper et al. (3). Solute fluxes in individual segments (i.e., 25–50 cm and 50–75 cm) were calculated in the same manner as described above for water flux. In the making of these calculations, negative values indicate absorption and positive values, secretion. However, for ease in presenting the results, the signs have been switched (positive values 5 absorption; negative values 5 secretion). All results were calculated after a 35-min equilibration period to allow a steady state to be reached (3, 46). Samples were collected during the equilibration period but were not used in data analysis. PR concentration in the stomach samples was measured spectrophotometrically at 560 nm after dilution (0.3-ml sample in 5-ml deionized water) and alkalinization with 1 ml borate buffer (pH 9.2) (18, 48). All samples and standards were analyzed in duplicate, with deionized water serving as a reference blank. PEG in the intestinal samples was determined by the method of Hyden (27) as modified by Malawer and Powell (32). Osmolality was measured by using freezingpoint depression (Multi-Osmette, Precision Systems, Natick MA), Na1 and K1 concentrations ([Na1] and [K1], respectively) by flame photometry (model IL 943, Instrumentation Laboratory, Lexington MA), and CHO by high-performance liquid chromatography (Dionex DX-500 System, Sunnyvale, CA). Samples that contained sucrose were hydrolyzed with 8.75 N trifluoracetic acid before measurement to liberate glucose and fructose. This allowed for a more accurate determination of CHO flux in the intestine. Percent change in plasma volume was calculated on the basis of the method of Dill and Costill (13). Statistical Analysis Data were tested for normality by using the Shapiro-Wilk test. The null hypothesis of the data, being a normal distribution, was not rejected (P . 0.05). A two-factor analysis of variance (ANOVA) with repeated measures was then used to determine 1) the effect of solution and intestinal segment on water and solute flux, 2) the effect of solution and intestinal segment on solution composition, 3) the effect of solution and time on blood and solution composition measurements, and 4) the effect of solution and time on PEG concentration at the various sampling sites. One-factor ANOVA and one-factor ANOVA with repeated measures were employed 1) when significant P values (P , 0.05) were observed in the two-factor ANOVA and 2) to compare mean values for sweat rate, percent body weight loss, urine production, rectal temperature, and heart rate. The Fisher post hoc test was utilized to identify significant differences (P , 0.05). Fig. 2. Stomach volumes and gastric emptying rates at each 10-min period during experiment after 35-min equilibration period. Values are means 6 SE. Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 18, 2017 The technique is described elsewhere (23), but changes made to fit this protocol are as follows. Multilumen tube specifications. The multilumen tube (Arndorfer, Greendale, WI) was 240 cm long and had five lumens, each 2 mm in diameter. At the end of the tube, a latex balloon was attached with 2–0 silk and held 1.5 ml of mercury enclosed in a double bag of latex. One lumen served to inflate the balloon, another to sample fluid from the proximal site of the test segment (,5 cm past the pyloric sphincter), and other lumens to sample fluid 25, 50, and 75 cm distal to the proximal site. These were glued together in a semirounded configuration. The sampling sites had three holes spaced 1 cm apart located at the top and bottom of the lumen, with a polyvinyl basket over one side to prevent the holes from lodging in the intestinal mucosa. During each 10-min interval of the experiment, intestinal fluid was collected at a rate of 1 ml/min from the proximal, 25-cm, and 50-cm sampling sites, and by constant siphonage at the 75-cm sampling site. Net water flux values were calculated for each interval according to the following equations (3) Analytical Procedures 207 ABSORPTION FROM DIFFERENT INTESTINAL SEGMENTS DURING EXERCISE Table 1. Comparisons of sweat rate, percent body weight loss, urine production, final rectal temperature, and final heart rate between the 2 experimental conditions Solution Sweat Rate, l/h Body Wt Loss, % Urine Produced, ml Final Rectal Temperature, °C Final Heart Rate, beats/min WP CHO-E 1.13 6 0.10 1.11 6 0.02 0.18 6 0.15 0.18 6 0.09 255 6 97 166 6 35 38.4 6 0.10 38.5 6 0.08 146 6 7 146 6 5 Values are means 6 SE; n 5 7 subjects. WP, water placebo; CHO-E, carbohydrate-electrolyte beverage. The pilot study referred to at the beginning of this study was carried out identically to the methods described above, except that there was only a 0- to 25-cm test segment in the multilumen tube (for specifics, see Ref. 27). RESULTS Fig. 3. Individual water flux data in segments of proximal small intestine. Mean values are 6 SE. A: 0- to 25-cm segment. Arrows, all 7 subjects exhibited higher rates of water absorption with WP compared with CHO-E. B: 25- to 50-cm segment. Arrows, 6 of 7 subjects had greater water absorption with CHO-E compared with WP. C: 50- to 75-cm segment. No significant difference was observed between beverages (arrows were not necessary). D: 0- to 75-cm segment. No significant difference was observed between beverages (arrows were not necessary). * Significantly different from WP, P , 0.05. # Significantly different from 0–25 cm, P , 0.05. Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 18, 2017 All subjects began the experiments in a euhydrated state on the basis of plasma osmolality values (290 6 1 mosmol/kgH2O for both WP and CHO-E). There were no differences in cardiovascular, fluid, or thermoregulatory measurements (sweat rate, percent body weight loss, urine production, rectal temperature, final heart rate) between the two experimental conditions (Table 1). Fluid ingestion offset fluid losses due to sweating and sample collection (see %body weight loss, Table 1). Mean GE did not differ between the two drinks (18.1 6 1.1 vs. 19.2 6 0.7 ml/min for WP and CHO-E, respectively). Mean gastric secretion rates were also not different for the two solutions (26.0 6 7.1 vs. 23.7 6 10.8 ml/10 min for WP and CHO-E, respectively). GE was maintained at a steady rate by producing a relatively constant stomach volume. There were no differences over time for stomach volume or GE in either experiment after the 35-min equilibration period (mean stomach volume postequilibration: WP 5 264 6 60 ml; CHO-E 5 240 6 43 ml) (Fig. 2). In terms of intestinal steady-state conditions (after the 35-min equilibration period), no differences were observed in PEG concentrations at a given sampling site over time for a given solution. However, significant differences were observed in mean fluid absorption in the different segments of the small intestine for a given solution (Fig. 3). Moreover, water flux in specific areas of the small intestine was dependent on solution composition (Fig. 3). When the whole 75-cm segment was examined, no difference occurred in water absorption (12.4 6 1.1 vs. 10.4 6 1.1 ml · cm21 · h21 for WP and CHO-E, respectively) (Fig. 3). Total water absorption for the whole 75-cm segment accounted for 83 and 72% (not sigificant) of the fluid available for absorption (after correction for fluid sampled from the stomach and intestine) for WP and CHO-E, respectively. Of the fluid absorbed, 80 and 82% were retained for WP and CHO-E, respectively, when urine production (Table 1) was taken into account. Total solute flux (TSF) was significantly different (0.8 6 0.2 vs. 4.2 6 0.3 mmol · cm21 · h21 for WP and CHO-E, respectively; P , 0.05) over the entire 75 cm. TSF did not differ among segments for a given solution, or between beverages within segments, although the CHO-E solution exhibited higher rates for TSF compared with WP (Fig. 4). The difference in TSF is primarily attributable to CHO flux for the CHO-E beverage (Table 2). The osmolality of the WP increased significantly (P , 0.05) at each sampling site in the intestine as it moved distally (Fig. 5), which was reflected in [Na1] and [K1] changes (Figs. 6 and 7). These changes were smaller during the CHO-E trial, although significant increases (P , 0.05) were observed for values for this solution in the stomach and proximal sampling site compared with sites 25 cm and beyond. Net fluxes for both Na1 and K1 are presented in Table 2. Plasma volume was not significantly different between trials at any time point throughout the experiments (Fig. 8). Plasma osmolality increased significantly (P , 0.05) during exercise in both trials but did 208 ABSORPTION FROM DIFFERENT INTESTINAL SEGMENTS DURING EXERCISE not change after the 35-min equilibration period, and there was no difference between experiments at any time point except at 45 min, when the WP (292 6 2 mosmol/kgH2O) was significantly lower than CHO-E (297 6 1 mosmol/kgH2O). Mean plasma osmolality values for the postequilibration period were 293 6 2 and 295 6 1 mosmol/kgH2O for WP and CHO-E, respectively. Plasma [Na1] did not change with exercise time, and the values did not differ at any point between beverages (mean values postequilibration 5 142.1 6 0.9 vs. 143.5 6 0.4 meq/l for WP and CHO-E, respectively). Plasma [K1] increased significantly at each time point in both trials (P , 0.05), although no differences were observed between trials at these times, nor were the postequilibration mean values different between trials (4.76 6 0.06 vs. 4.81 6 0.06 meq/l for WP and CHO-E, respectively). Plasma glucose concentration was maintained throughout the exercise protocol during ingestion of CHO-E but declined significantly during the WP trial, resulting in significant differences between the two trials for the final 55 min of the experiment (mean values postequilibration 5 5.4 6 0.09 vs. 4.7 6 1.0 mM for CHO-E and WP, respectively). DISCUSSION This is the first study to simultaneously measure intestinal absorption from sequential segments of the proximal small intestine together with GE of beverages consumed orally during exercise. The results provide Fig. 5. Osmolality of ingested solutions in stomach and at various sites in proximal small intestine. Values are means 6 SE. * Significantly different from WP. # Significantly different from stomach site, P , 0.05. †Significantly different from 0-cm site, P , 0.05. & Significantly different from 25-cm site, P , 0.05. @ Significantly different from 50-cm site, P , 0.05. evidence that fluid absorption from a given solution varies from one segment to another and with the composition of the ingested solution. The following discussion focuses on 1) potential mechanisms to explain this differential segmental absorption (duodenal vs. jejunal), 2) the consequences of bypassing the duodenum in intestinal absorption studies, 3) gastric influences, and 4) the relationship of intestinal absorption to fluid balance, thermoregulation, and energy substrate availability. It is important to note that these experiments were performed by euhydrated, healthy subjects during cycle exercise at 60–65% V̇O2 peak. Duodenal Absorption (0–25 cm) The duodenum is considered the most permeable portion of the small intestine to water, and its primary function is to bring either hyper- or hypotonic chyme to isotonicity through net secretion or absorption of water and diffusable ions (51). The greater fluid absorption observed in the duodenum during ingestion of the WP compared with the CHO-E beverage is attributable to the osmotic superiority of the WP and passive movement of water down its concentration gradient. The WP entered the duodenum at an osmolality of 52 6 11 mosmol/kgH2O and had an osmolality of 164 6 12 Table 2. Na1, K 1, and CHO fluxes in intestinal segments studied Na1 Flux K1 Flux CHO Flux Intestinal Segment WP CHO-E WP CHO-E 0–25-cm 25–50-cm 50–75-cm 0.0160.47 0.1960.44 1.9960.65† 21.0460.36 1.2260.33† 1.8760.10† 0.0960.02 0.0360.01 0.0560.01 0.060.03 0.1260.03* 0.0760.01 WP CHO-E 6.061.1 3.360.8 0.960.3† Values are means 6 SE. Na1 and K1 fluxes also represent movement of Cl2 with each respective cation. Units are meq · cm21 · h21 for Na1 and K1, and mmol · cm21 · h21 for CHO. Negative values represent secretion. * Significantly different from WP. † Significantly different from 0to 25-cm segment. Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 18, 2017 Fig. 4. Total solute flux in 3 segments of proximal small intestine. Values are means 6 SE. ABSORPTION FROM DIFFERENT INTESTINAL SEGMENTS DURING EXERCISE mosmol/kgH2O at 25 cm. Corresponding values for the CHO-E beverage were 252 6 5 and 278 6 3 mosmol/ kgH2O, respectively (Fig. 5). Luminal [Na1] was virtually identical between solutions at the beginning of the duodenum but rose significantly higher during ingestion of the WP compared with the CHO-E beverage (Fig. 6). This elevation in [Na1] is due to greater Na1 secretion and/or greater water absorption. Because net Na1 flux in the duodenum was essentially zero (Table 2) and net water flux was significantly greater for the WP than the CHO-E beverage, the higher [Na1] in the first 25 cm is attributable to initial Na1 secretion and a high rate of water movement down an osmotic gradient of Fig. 7. Potassium concentration in stomach and various segments of proximal small intestine. Values are means 6 SE. * Significantly different from WP, P , 0.05. # Significantly different from stomach site, P , 0.05. †Significantly different from 0-cm site, P , 0.05. & Significantly different from 25-cm site, P , 0.05. Fig. 8. Percent change in plasma volume during 85 min of cycle ergometry at 60–65% peak O2 uptake while subjects ingested either WP or a 6% CHO-E beverage. Values are means 6 SE. ,130–230 mosmol/kgH2O. Net water absorption in the presence of Na1 secretion has also been observed in the proximal small intestine by Santangelo and Krejs (45). K1 fluxes were negligible in both trials and did not contribute substantially to TSF. Water absorption values obtained in the 0- to 25-cm segment contrast with those previously observed during segmental perfusion of the duodenojejunum. Perfusion of distilled water (infusion rate 5 15 ml/min) in the distal duodenum and proximal jejunum during both rest and exercise (70% V̇O2 peak) in two previous investigations (20, 23) produced significantly lower fluid absorption rates (,8–9 ml · cm21 · h21 ) compared with a CHO-E solution similar to that used in this investigation (,12–13 ml · cm21 · h21 ). In the present study, water flux in the duodenum was 30 vs. 15 ml · cm21 · h21 for WP and CHO-E, respectively. This discrepancy is attributable to the intestinal segment studied. In the previous reports, the test segment under study consisted primarily of the jejunum. In this, and one other recent study (44), water absorption was greater when the duodenum was studied. Reitemeier et al. (42) also observed rapid rates of water absorption (50% in 3 min and 67% in 5 min) in the distal duodenum/proximal jejunum after infusion of labeled water (isotopic tracer method using D2O) into the duodenum. These rates closely resemble those of the present study (for WP, ,60% total volume absorbed in 0- to 25-cm segment). In addition, Shi et al. (49) reported water flux for a hypotonic solution exhibited the highest water absorption rates, followed by isotonic and hypertonic solutions, when water flux in the duodenum and jejunum was combined. In contrast, Santangelo and Krejs (45) perfused the stomach with water at 22 ml/min and examined water absorption in a 50-cm mixing segment, 70-cm jejunal test segment, and 70-cm ileal test segment. Their results indicated higher water absorption in the jejunum (7.2 ml · cm21 · h21 ) vs. mixing segment Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 18, 2017 Fig. 6. Sodium concentration in stomach and various sites in proximal small intestine. Values are means 6 SE. * Significantly different from CHO-E, P , 0.05. # Significantly different from stomach value, P , 0.05. †Significantly different from 0-cm site value, P , 0.05. & Significantly different from 25-cm site, P , 0.05. 209 210 ABSORPTION FROM DIFFERENT INTESTINAL SEGMENTS DURING EXERCISE [3.8 ml · cm21 · h21 (presumably duodenum)] and the ileum (2.0 ml · cm21 · h21 ). However, because their 50-cm mixing segment ended at the ligament of Treitz (start of the jejunum), and given that the duodenum is only ,25 cm long (10, 33), the other 25 cm of this segment must have been in the stomach. Thus mixing segment water absorption actually occurred in ,25 cm rather than 50 cm, elevating water absorption in the duodenum to ,7.6 ml · cm21 · h21, which is approximately the same as that found in the jejunum. Higher water absorption values in this study compared with those in others may also reflect high GE rates (,18–19 ml/min), which served as the infusion rate when water flux was calculated (52). Most investigators who use segmental perfusion employ infusion rates of 10–15 ml/min. Jejunal Absorption (25–50 cm and 50–75 cm) uptake is greater in jejunal compared with duodenal brush border membrane vesicles. By the final 25-cm segment (50–75 cm), 66% of the WP and 53% of the CHO-E beverage were absorbed, which presumably reduced the flow rate of each to this segment and explains the significant decline in fluid absorption compared with their highest values (0- to 25-cm segment). Furthermore, the osmotic gradient basically disappeared by the end of this segment for the WP beverage (WP 5 ,260 mosmol/kgH2O; Fig. 5). There were no differences between the two beverages for fluid absorption in this segment. In the entire 75-cm segment, ,75% of the ingested volume of each solution (minus volume withdrawn for sampling) was absorbed with no differences in total water absorption between solutions. Using the isotopic tracer technique (D2O), Davis et al. (12) also observed similar rates of fluid replacement between an isotonic CHO-E beverage and distilled water during cycle exercise in the heat (2 h at 75% V̇O2 peak; 27°C) . In contrast, Leiper et al. (30) and Davis (11) found that isotonic CHO-E solutions were absorbed more readily than water in resting subjects by using this method. It is important to note that isotopic tracer studies do not examine net flux of fluid, only unidirectional flux from intestinal lumen to blood. It is apparent that had the jejunum been studied exclusively, and the duodenum bypassed, the present results would have been misleading. Interpretation of absorptive efficacy of the beverages (on the basis of only jejunal data) would have favored the CHO-E beverage. However, when duodenal data are considered, fluid absorption was greater for the WP, and thus overall absorption of each beverage indicates no distinct advantage for either. Gastric Influence Individual GE rates served as infusion rates to calculate water and solute flux. Mean gastric volumes of ,250 ml maintained GE rates of 18–19 ml/min, which agree with other studies using this technique (28, 44) and are comparable with other repeateddrinking studies (34, 40, 41, 43). These rates were somewhat higher than infusion rates in most segmental perfusion studies (i.e., 10–15 ml/min). As previously noted, this may increase water and solute absorption in the intestine (52). Maintenance of a moderate to high gastric volume ensures a high rate of GE (38). For instance, Mitchell and Voss (34) reported a GE rate of 18.9 ml/min after ingestion of ,430 ml of a 7.5% CHO solution every 15 min during 2 h of cycle exercise at 70% V̇O2 peak. Rehrer et al. (40, 41) report emptying rates of 14–16 ml/min with ingestion of 8 ml/kg initially (,600 ml) and 2–3 ml/kg (,150–200 ml) at 20-min intervals of a 4.5% glucose solution, an isotonic sucrose (6%) drink, or water during cycling at 70% V̇O2 peak. Subjects in a study by Ryan et al. (43) emptied 5% CHO solutions at rates .16 ml/min while ingesting 350 ml every 20 min during cycling for 3 h at 60% V̇O2 peak in the heat. Although maximal GE rates are not known, Costill and Saltin (4) induced average GE rates of Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 18, 2017 Net fluid absorption significantly decreased for the WP beverage in the second 25-cm segment of the intestine but remained unchanged for the CHO-E beverage, resulting in significantly more fluid absorption from the CHO-E. This finding is attributable to three factors: 1) the WP had a lower flow rate to this segment due to higher water absorption in the duodenum; 2) the osmotic gradient for the WP was reduced compared with the duodenum (,100 mosmol/kgH2O increase in luminal osmolality from the proximal sampling site in the duodenum to proximal sampling site in the jejunum; Fig. 5); and 3) the WP did not contain CHO, which limited total solute absorption compared with the CHO-E beverage (Fig. 4). Other studies have also found CHO-E solutions to be absorbed faster than plain water in the jejunum (20, 23, 31). This finding is attributable to enhanced passive water movement in response to increased net solute absorption. Solute flux values are shown in Table 2 (Na1, K1, and CHO) and Fig. 4 (TSF). As expected, the CHO-E beverage produced greater TSF, the majority coming from CHO absorption, allowing sustained fluid absorption in the jejunum compared with the WP. This has been termed ‘‘solute drag,’’ ‘‘solvent drag,’’ and solution drag and was first proposed by Curran (8) and Curran and Macintosh (9). Schedl and Clifton (46), Sladen and Dawson (53), and Fordtran (16) further demonstrated the stimulatory effect of glucose on Na1 and water transport in the jejunum. Recently, Fine et al. (15) reported that the mechanisms responsible for this increased absorption are 1) forceful osmotically driven water movement that ‘‘pulls’’ small hydrophilic solutes through trans- and/or paracellular routes (i.e., solvent drag), and 2) the creation of a concentration gradient (created by osmotically driven water absorption) that allows for passive solute movement independent of water flow. Shi et al. (50) have also reported a close relationship between water absorption and solute absorption in the duodenojejunum, especially when multiple transportable substrates are present (i.e., glucose, sucrose, glycine, Na1 ). The maintenance of fluid and solute absorption in this segment for the CHO-E beverage can also be explained by the findings of Harig et al. (24), who showed that D-glucose ABSORPTION FROM DIFFERENT INTESTINAL SEGMENTS DURING EXERCISE 25 ml/min after a single bolus (600 ml) of a hypotonic (,200 mosmol/kgH2O) solution. Duchman et al. (14) observed GE rates for water of .40 ml/min after infusion of 750 ml into the stomach with subsequent infusions of ,180 ml every 10 min. Rates of gastric secretion in the present study were minimal for both solutions (26.0 6 7.1 vs. 23.7 6 10.8 ml/10 min for WP and CHO-E, respectively). These rates compare favorably with other recent studies using similar solutions (28, 35) and likely did not significantly impact GE. Furthermore, after a 35-min equilibration period, gastric secretions did not significantly alter the osmolality, [Na1], or [K1] of the ingested solutions (Figs. 6–8). Fluid Homeostasis, Thermoregulation, and Substrate Availability tion. Furthermore, these data argue for the inclusion of the duodenum in segmental perfusion studies designed to evaluate the efficacy of oral rehydration solutions because this segment of the intestine plays such a crucial role in fluid absorption. Finally, conclusions drawn from studies that only examine jejunal absorption of a beverage may be misleading when extrapolated to assess the overall effect on fluid homeostasis with oral ingestion of the same beverage. The authors thank the subjects for participating in the experiments, Joan Seye for assistance in manuscript preparation, and Pat Johnston, Shawn Fleck, Kay Pals, and Tonya Brueggeman for technical assistance. This study was supported by the Gatorade Sports Science Institute. Address for reprint requests: C. V. Gisolfi, Dept. of Exercise Science, N414 Field House, Univ. of Iowa, Iowa City, IA 52242-1111. Received 25 November 1996; accepted in final form 18 March 1997. REFERENCES 1. Barclay, G. R., and L. A. Turnberg. Effect of moderate exercise on salt and water transport in the human jejunum. Gut 29: 816–820, 1988. 2. Beckers, E. J., N. J. Rehrer, F. Brouns, F. T. Hoor, and W. H. M. Saris. Determination of total gastric volume, gastric secretion and residual meal using the double sampling technique of George. Gut 29: 1725–1729, 1988. 3. Cooper, H., R. Levitan, J. S. Fordtran, and R. J. Ingelfinger. A method for studying absorption of water and solute from the human small intestine. Gastroenterology 50: 1–7, 1966. 4. Costill, D. L., and B. Saltin. Factors limiting gastric emptying during rest and exercise. J. Appl. Physiol. 37: 679–683, 1974. 5. Coyle, E. F., A. R. Coggan, M. K. Hemmert, and J. L. Ivy. Muscle glycogen utilization during prolonged strenuous exercise when fed carbohydrate. J. Appl. Physiol. 61: 165–172, 1986. 6. Coyle, E. F., J. M. Hagberg, B. F. Hurley, W. H. Martin, A. A. Ehsani, and J. O. Holloszy. Carbohydrate feeding during prolonged strenuous exercise can delay fatigue. J. Appl. Physiol. 55: 230–235, 1983. 7. Coyle, E. F., and S. J. Montain. Carbohydrate and fluid ingestion during exercise: are there trade-offs? Med. Sci. Sports Exerc. 24: 671–678, 1992. 8. Curran, P. F. Na, Cl and water transport by rat ileum in vitro. J. Gen. Physiol. 43: 1137–1148, 1960. 9. Curran, P. F., and J. R. Macintosh. A model system for biological water transport. Nature 193: 347–348, 1962. 10. Davenport, H. W. Motility of the small intestine. In: Physiology of the Digestive Tract (5th ed.), edited by H. W. Davenport. Chicago, IL: Year Book, 1983, p. 70–97. 11. Davis, J. M., D. R. Lamb, W. A. Burgess, and W. P. Bartoli. Accumulation of deuterium oxide in body fluids after ingestion of D2O-labeled beverages. J. Appl. Physiol. 63: 2060–2066, 1987. 12. Davis, J. M., D. R. Lamb, R. R. Pate, C. A. Slentz, W. A. Burgess, and W. P. Bartoli. Carbohydrate-electrolyte drinks: effects on endurance cycling in the heat. Am. J. Clin. Nutr. 48: 1023–1030, 1988. 13. Dill, D. B., and D. L. Costill. Calculation of percentage changes in volumes of blood, plasma, and red cells in dehydration. J. Appl. Physiol. 37: 247–248, 1974. 14. Duchman, S. M., T. L. Bleiler, H. P. Schedl, R. W. Summers, and C. V. Gisolfi. Effects of gastric function on intestinal composition of oral rehydration solutions. Med. Sci. Sports Exerc. 22: S89, 1990. 15. Fine, K. D., C. A. S. Ana, J. L. Porter, and J. S. Fordtran. Mechanism by which glucose stimulates the passive absorption of small solutes by the human jejunum in vivo. Gastroenterology 107: 389–395, 1994. 16. Fordtran, J. S. Simulation of active and passive sodium absorption by sugars in the human jejunum. J. Clin. Invest. 55: 728–737, 1975. Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 18, 2017 Whereas water absorption differed among the intestinal segments and solutions in certain segments, there were no differences in overall water retention, percent change in plasma volume (Fig. 8), or plasma osmolality. Nor were differences observed between solutions for sweat rate, percent body weight loss, urine production, final rectal temperature, or final heart rate (Table 1). Within the 75-cm segment studied, our calculations accounted for the absorption of 83 vs. 72% of the ingested volume for the WP and CHO-E beverages, respectively. After urine production was substracted from results of each trial, 80 and 82% of the absorbed volume was retained for WP and CHO-E trials, respectively. This indicates that although the WP beverage was absorbed earlier in the small intestine than the CHO-E beverage, it does not improve fluid homeostasis or thermoregulatory function compared with the CHO-E beverage. Segmental perfusion data do not indicate the overall efficacy of a beverage. Studies examining intestinal absorption should also determine fluid retention together with plasma volume changes, and possibly body fluid shifts. Plasma glucose concentrations were significantly lower throughout exercise in the WP compared with the CHO-E trial. Absorption of CHO by all segments of the intestine in the CHO-E trial promoted maintenance of plasma glucose concentrations throughout the experiment. Eighty-eight grams of CHO were absorbed within the 75-cm segment studied, or ,1 g/min. This rate meets the maximal blood glucose oxidation rate during prolonged exercise (25). Although performance was not measured in these experiments, ingestion of CHOcontaining solutions during prolonged exercise can improve endurance and enhance performance probably through the maintenance of plasma glucose concentration (5–7, 12, 36, 37). In summary, significant differences exist in intestinal absorption between solutions and among segments in the proximal small intestine. In the duodenum, fluid from the WP beverage is absorbed quickly by movement down a large osmotic gradient despite the possibility of electrolyte secretion. In the jejunum, fluid absorption from the WP beverage is significantly reduced compared with the CHO-E solution, which stimulates greater solute flux, thus promoting greater fluid absorp- 211 212 ABSORPTION FROM DIFFERENT INTESTINAL SEGMENTS DURING EXERCISE 35. Murray, R., D. E. Eddy, W. P. Bartoli, and G. L. Paul. Gastric emptying of water and isocaloric carbohydrate solutions consumed at rest. Med. Sci. Sports Exerc. 26: 725–732, 1994. 36. Murray, R., D. E. Eddy, T. W. Murray, J. G. Seifert, G. L. Paul, and G. A. Halaby. The effect of fluid and carbohydrate feedings during intermittent cycling exercise. Med. Sci. Sports Exerc. 19: 597–604, 1987. 37. Murray, R., J. G. Seifert, D. E. Eddy, G. L. Paul, and G. A. Halaby. Carbohydrate feeding and exercise: effect of beverage carbohydrate content. Eur. J. Appl. Physiol. 59: 152–158, 1989. 38. Noakes, T. D., N. J. Rehrer, and R. J. Maughan. The importance of volume in regulating gastric emptying. Med. Sci. Sports Exerc. 23: 307–313, 1991. 39. Phillips, S. F., and W. H. J. Summerskill. Water and electrolyte transport during maintenance of isotonicity in human jejunum and ileum. J. Lab. Clin. Med. 70: 686–698, 1967. 40. Rehrer, N. J., F. Brouns, E. J. Beckers, F. TenHoor, and W. H. M. Saris. Gastric emptying with repeated drinking during running and bicycling. Int. J. Sports Med. 11: 238–243, 1990. 41. Rehrer, N. J., A. J. M. Wagenmakers, E. J. Beckers, D. Halliday, J. B. Leiper, F. Brouns, R. J. Maughan, K. Westerterp, and W. H. M. Saris. Gastric emptying, absorption, and carbohydrate oxidation during prolonged exercise. J. Appl. Physiol. 72: 468–475, 1992. 42. Reitemeier, R. J., C. F. Code, and A. L. Orvis. Comparison of rate of absorption of labeled sodium and water from upper small intestine of healthy human beings. J. Appl. Physiol. 10: 256–260, 1957. 43. Ryan, A. J., T. L. Bleiler, J. E. Carter, and C. V. Gisolfi. Gastric emptying during prolonged cycling exercise in the heat. Med. Sci. Sports Exerc. 21: 51–58, 1989. 44. Ryan, A. J., G. P. Lambert, X. Shi, R. T. Chang, R. W. Summers, and C. V. Gisolfi. Effect of hypohydration on gastric emptying and intestinal absorption during exercise. FASEB J. 9: 1692, 1995. 45. Santangelo, W. C., and G. J. Krejs. Absorption of pure water by the human gastrointestinal tract (Abstract). Gastroenterology 88: 1569, 1985. 46. Schedl, H. P., and J. A. Clifton. Solute and water absorption by the human small intestine. Nature 199: 1264–1267, 1963. 47. Schedl, H. P., R. J. Maughan, and C. V. Gisolfi. Intestinal absorption during rest and exercise: implications for formulating an oral rehydration solution (ORS). Med. Sci. Sports Exerc. 26: 267–280, 1994. 48. Schedl, H. P., D. Miller, and D. White. Use of polyethylene glycol and phenol red as unabsorbed indicators for intestinal absorption studies in man. Gut 7: 159–163, 1966. 49. Shi, X., R. W. Summers, H. P. Schedl, R. T. Chang, G. P. Lambert, and C. V. Gisolfi. Effects of solution osmolality on absorption of select fluid replacement solutions in human duodenojejunum. J. Appl. Physiol. 77: 1178–1184, 1994. 50. Shi, X., R. W. Summers, H. P. Schedl, S. W. Flanagan, R. T. Chang, and C. V. Gisolfi. Effects of carbohydrate type and concentration and solution osmolality on water absorption. Med. Sci. Sports Exerc. 27: 1607–1615, 1995. 51. Sladen, G. E. Absorption of fluid and electrolyte in health and disease. In: Intestinal Absorption in Man, edited by I. McColl and G. E. Sladen. London: Academic, 1975, p. 51–98. 52. Sladen, G. E., and A. M. Dawson. Effects of flow rate on the absorption of glucose in a steady state perfusion system in man. Clin. Sci. (Lond.) 36: 133–145, 1969. 53. Sladen, G. E., and A. M. Dawson. Interrelationships between the absorptions of glucose, sodium and water by the normal human jejunum. Clin. Sci. (Lond.) 36: 119–132, 1969. 54. Whalen, G. E., J. A. Harris, J. E. Geenen, and K. H. Soergel. Sodium and water absorption from the human small intestine. Gastroenterology 51: 975–984, 1966. Downloaded from http://jap.physiology.org/ by 10.220.32.247 on June 18, 2017 17. Fordtran, J. S., and B. Saltin. Gastric emptying and intestinal absorption during prolonged severe exercise. J. Appl. Physiol. 23: 331–335, 1967. 18. George, J. D. New clinical method for measuring the rate of gastric emptying: the double sampling test meal. Gut 9: 237–242, 1968. 19. Gisolfi, C. V., and S. M. Duchman. Guidelines for optimal replacement beverages for different athletic events. Med. Sci. Sports Exerc. 24: 679–687, 1992. 20. Gisolfi, C. V., K. J. Spranger, R. W. Summers, H. P. Schedl, and T. L. Bleiler. Effects of cycle exercise on intestinal absorption in humans. J. Appl. Physiol. 71: 2518–2527, 1991. 21. Gisolfi, C. V., R. Summers, and H. Schedl. Intestinal absorption of fluids during rest and exercise. In: Perspectives in Exercise Science and Sports Medicine. Fluid Homeostasis During Exercise, edited by C. V. Gisolfi and D. R. Lamb. Indianapolis, IN: Benchmark, 1990, p. 129–180. 22. Gisolfi, C. V., R. W. Summers, H. P. Schedl, and T. L. Bleiler. Intestinal water absorption from select carbohydrate solutions in humans. J. Appl. Physiol. 73: 2142–2150, 1992. 23. Gisolfi, C. V., R. W. Summers, H. P. Schedl, T. L. Bleiler, and R. A. Oppliger. Human intestinal water absorption: Direct vs. indirect measurements. Am. J. Physiol. 258 (Gastrointest. Liver Physiol. 21): G216-G222, 1990. 24. Harig, J. M., K. H. Soergel, J. Barry, and K. Ramaswamy. Brush border membrane vesicles formed from human duodenal biopsies exhibit Na1-dependent concentrative L-leucine and Dglucose uptake. Biochem. Biophys. Res. Commun. 156: 164–170, 1988. 25. Hawley, J. A., S. C. Dennis, and T. D. Noakes. Carbohydrate, fluid, and electrolyte requirements during prolonged exercise. In: Sports Nutrition. Minerals and Electrolytes, edited by C. V. Kies and J. A. Driskell. Boca Raton, FL: CRC, 1995, chapt. 19, p. 235–265. 26. Hunt, J. B., A. V. Thillainayagam, A. F. M. Salim, S. Carnaby, E. J. Elliott, and M. J. G. Farthing. Water and solute absorption from a new hyppotonic oral rehydration solution: evaluation in human and animal perfusion models. Gut 33: 1652–1659, 1992. 27. Hyden, S. A turbidimetric method of determination of higher polyethylene glycols in biological materials. Ann. R. Agric. Coll. Sweden 22: 139–145, 1955. 28. Lambert, G. P., R. T. Chang, D. Joensen, X. Shi, R. W. Summers, H. P. Schedl, and C. V. Gisolfi. Simultaneous determination of gastric emptying and intestinal absorption during cycle exercise in humans. Int. J. Sports Med. 17: 48–55, 1996. 29. Leiper, J. B. Absorption of water and electrolytes from hypotonic, isotonic, and hypertonic solutions (Abstract). Proc. Nutr. Soc. 45: 78A, 1986. 30. Leiper, J. B., A. E. Fallick, and R. J. Maughan. Comparison of water absorption from an ingested glucose/electrolyte solution (ges) and potable water using a tracer technique in healthy volunteers. Clin. Sci. (Lond.) 4, Suppl. 18: 68P, 1988. 31. Leiper, J. B., and R. J. Maughan. Absorption of water and electrolytes from hypotonic, isotonic and hypertonic solutions. J. Physiol. (Lond.) 373: 90P, 1986. 32. Malawer, S. J., and D. W. Powell. An improved turbidimetric analysis of polyethylene glycol utilizing an emulsifier. Gastroenterology 53: 250–256, 1967. 33. McGuigan, J. E., and M. E. Ament. The stomach and duodenum. Anatomy, embryology, and developmental anomalies. In: Gastrointestinal Disease. Pathophysiology Diagnosis Management (3rd ed.), edited by M. H. Sleisenger and J. S. Fordtran. Philadelphia, PA: Saunders, 1983, p. 505–521. 34. Mitchell, J. B., and K. W. Voss. The influence of volume on gastric emptying and fluid balance during prolonged exercise. Med. Sci. Sports Exerc. 23: 314–319, 1991.