Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
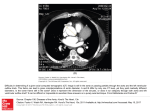
CLINICAL CONFERENCE Editor: EDGAR V. ALLEN, M.D. Associate Editor: RAYMOND D. PRUITT, M.D. Coarctation of Aorta Complicated by Bacterial Endocarditis and an Aneurysm of the Sinus of Valsalva By FRANK GLENN, M.D., HAROLD J. STEWART, M.D., MARY A. ENGLE, M.D., DANIEL S. LUKAS, M.D., JOSEPH ARTUSmo, M.D., ISRAEL S. STEINBERG, M.D., AND GEORGE R. HOLSWWADE, M.D. Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 she began to improve and by the age of 9 years she was average in size (fig. 1). She tired after exercise and became short of breath more quickly than her playmates. Restriction of activities was advised by the physician. At this time she had a murmur of aortic insufficiency. The first recorded blood pressure determination was at age 12, measured at 165-145/65 mm. Hg in the arm. In 1947 the patient had fever and blood DR. FRANK GLENN: The patient for today 's discussion presented sonme particularly interesting and challenging problems when she was first seen at The New York Hospital in November 1954. I am going to ask our panel to review with you the ideas and considerations that confronted us in the diagnosis and management of this patient's heart disease. Dr. Engle, will you please give us the history ? DR. MARY A. ENGLE: The patient, a 27year-old married woman, was admitted for evaluation of coarctation of the aorta. From her and from the physicians who took care of her from infancy we obtained the following information. She was born 1 month prematurely. Because she failed to thrive, she was taken to a pediatrician at the age of 51/2 months. He discovered a loud systolic murmur all over the precordium and in the lung fields. The aortic and pulmonic second sounds were distinct, and there was iio precordial bulge. Fluoroscopy disclosed enlargement of the left ventricle. These findings remained unchanged throughout infanuv and childhood and she was considered to have a ventricular septal def ect. Failure to thrive was most marked during the first year. After the age of 2, however, culture was positive for Streptococcus viridans. The blood pressure in the arms was 210/70 and in the legs 122/80 at this time. She received a course of penicillin for 2 weeks. She suffered a second episode of Str. viridans infection in 1954. This was treated with intravenous penicillin and streptomycin for 6 weeks. The diagnosis of coarctation of the aorta was made at this time. The cardiothoracic ratio at this time was 53.4 per cent. DR. GLENN: Dr. Engle, is this the usual course of events for a patient with coarctation of the aorta? DR. ENGLE: YeS, it is a common story. The patient with coaretation of the aorta is apt to have difficulty from his lesion at 2 age periods: early infancy and early to mid-adult life. Babies may fail to thrive and even go into heart failure in the first months of life. The early difficulties seem related to the severity of the coaretation as well as to the relationship of this constriction to the ductus arteriosus, which is normally still patent in the newborn period. Medical management of the heart failure is quite successful in tiding those babies over the period of early difficulty From the Cardiovascular Conference Group made up of members from the various departments of the New York Hospital-Cornell Medical Center: Surgery, Frank Glenn, George R. Holswade; Medicine, Harold J. Stewart, Daniel S. Lukas; Pediatrics, Mary Allen Engle, Henry P. Goldberg; Radiology, Israel Steinberg, Nathaniel Finby; Anesthesiology, Joseph Artulsio; Obstetrics, Curtis L. M-~ei(lelsOin. 4324 Circulation, Volume XVII, March 1958 COMPLICATED COARCTATION OF AORTA AGE IN YEARS AGE IN YEARS 0 150 40 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 AGE IN YEARS AGE IN YEARS FIG. 1. Growth chart of patient V.W. Failure to grow was most marked during first year. After age 2 it improved and by age 9 was in the average range. Blood pressure in arm at (We are in12 years was 165-145/65 mlmi. Hg; at 16 years, 150/20; and at 18 years, 150/40. (lebted to Drs. Benjamin Kramer and Charles Shookof for supplying the information on this patient 's childhood and adolescent years, including growth data.) until adequate collateral circulation develops. This is usually achieved by the age of 2 years. This particular patient was not in heart failure but she did have cardiac enlargement at least from 5 months of age and her growth was markedly retarded for the first year. It is interesting that adults may not volunteer such a history even though this was a difficult time in their lives. It is a period beyond their memory, and unless a parent or the physicians' notes are available, as in the present case, this part of the history may be lost. DR. G-LENN: Dr. Stewart, if these childreix survive childhood, in brief, what may be the course of their disease? DR. hAROLD J. STEWART: Certain patients live a normal life span and die of some disease not related to the congenital defect. On the other hand during adulthood, patients with coaretation of the aorta are subject to several complications: (1) to subacute bacterial endarteritis or endocarditis, which may occur on the additional lesion of bicuspid aortic valve, (2) to rupture of the aorta, (3) to a cerebral vascular accident, (4) or to the manifestations of hypertensive cardiovascular disease, and perhaps heart failure, (5) heart failure or rupture of the aorta, or of a cerebral anieuirysmii, may result from the increased burden of pregnancy. return to the case DR. GLENN: Let presentation. What were the pertinent findings on examination when this patient came under observation here? DR. ENGLE: Physical examination revealed strong radial pulses and weak femoral pulses with a perceptible lag behind the radial impulse. Blood pressure in the arms was 190/50-0 and in the legs 95/40 mm. of Hg. A bounding pulsation was visible in the sulprasternal notch, and pulsations could be us 434 CLINICAL CONFERENCE Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 FIG. 2. Roentgenograms. A. Frontal, showing enlargement of left ventricle, lack of aortic knob prominence, anid rib notching. B. Lateral, showving anterior displacenient of esophagus l)y enlarged ascending aorta. seen and felt over the chest posteriorly. There was no cyanosis or clubbing of fingers or toes. The heart was enlarged to the anterior axillary line. A systolic thrill was palpable over the aortic area and in the suprasternal notch. A loud, long systolic murmur, maximal in the second right interspace, was transmitted to the neck vessels and the aorta, over the precordium, and to the chest posteriorly. A separate harsh systolic murmur was heard ill the fourth and fifth left parasternal spaces. A long, blowing diastolic murmur along the left sternal border originated at Erb's point. The lungs were clear, the liver and spleen were not enlarged, there was no peripheral edema, and embolic phenomena were not detected. Laboratory studies showed normal red blood cell count, hemoglobin, and hematocrit level, but the white blood cell count was 12,500 and the sedimentation rate was elevated. Three blood cultures were negative. X-ray Pnd fluoroscopy of the chest (fig. 2) revealed a cardiothoracic ratio of 60 per cent. The enlargement was predominantly left ventricular, though there was some enlargement of the left atrium as well. The aortic knob was normally prominent. In the left anterior oblique projection the ascending aorta was dilated anid widely pulsatile. Barium swallow confirmed the left atrial enlargement anid disclosed an anterior displacement of the esophagn's by a dilated portion of the ascendincg aorta. This was thought (aand later shown by angioeardiography) to be due to the poststenotic dilatation of the aorta below the coaretation. There were no other retroesop)hageal vessels, suggestive of aneurysmally dilated intercostal arteries. Rib notehinig was present bilaterally. Anl electrocardiogram disclosed a pattern of left ventricular hypertrophy (abnormally tall R w-aves in the left precordial and foot leads with deep S waves in the right precordial leads) and of left ventricular "strain" (depression of S-T segments and inversion of T waves in left precordial and foot leads with reciprocal changes over the right side of the precordium). DR. GLENN: Dr. Lukas, will you give us the pressure mneasuremernts you made? DR. DANIEL S. LUKASS: Lntra-arterial pres- COMPLICATED COARCTATION OF AORTA tracings were characteristic of coaretation of the aorta and aortic insufficiency. Measurements were 227/63 (mean 122) mnm. Hg in the arm and 110/66 (inean 82) ill the leg. DR. GLENN: Dr. Stewart will you comment on the diagnosis at this point? DR. STEWART: Dr. Glenn, I think that the diagnosis of coaretation of the aorta was readily made clinically in this patient. The volume of all the peripheral pulses should be estimated clinically in every patient and the diagnosis should be suspected when the volume of the pulses ini the legs is less than that in the arms, or may indeed be absent. Moreover, the blood pressure should be taken not only in both arms but also in both legs in every patient in all age groups. The following findings pointed to this diagnosis: 1. The volume of the radial pulses was greater than the femoral pulses. 2. The blood pressure in the arms was higher than in the legs, indicating, an obstruction to the flow of blood through the aorta below the subelaviati artery. It mliay be said parenthetically that the blood pressure may l)e normal in the arms, but decreased to absent in the legs. The carotid pulsations were exaggerated as were the aortic pulsations in the suprasternal notch. 3. The peripheral signs of collateral circulation shown by pulsations and bruits over intercostal arteries posteriorly and other collateral vessels used to carry arterial blood from above the coaretation back into the aorta below the obstruction. 4. The x-ray of the chest showed notching or scallopingr of the lower margins of the ribs by the dilated tortuous intercostal arteries. Both the pulsations and notching may be absent in children. The presence of these latter 2 signs is a valuable guide to the surgeon as to the possibility of a successful operation because of the availability of these vessels to maintain circulation while the aorta is clamped. The x-ray showed left ventricular enlargement and absence of the aortic knob. 5. The exact location of the coaretation and the amount of proximal segment beyond the subelavian sure 4 35) Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 available to the surgeon for the repair was demonstrated by angiocardiogram, which Dr. Steinberg will discuss shortly. Perhaps Dr. Engle has some additional comment to make. DR. ENGLE: Localization of the coarctation was possible from the studies thus far presented. The fact that the pulses in the neck and in both arms were equally strong placed the obstruction distal to the left subelavian artery. There was evidence on barium swallow of a large retroesophageal vessel below the level of the descending aortic arch (fig. 2B). Ill such a patient this deformity of the esophogram is due to the poststenotic dilatation of the aorta just beneath the coarctation. Thus the narrowed segment of aorta was localized to the area of the aorta where it most commonly occurs: at the level of the ligamentnm arteriosum. One additional localizing sign that is useful is the smooth, blowing, well-localized systolic murmur that is heard posteriorly near the midline overlying the narrowed segment. If one listens along the course of the descending aorta, such a murmur can often be detected, even if the coaretation is in the abdominal aorta. This patient, however, had such a loud systolic murmur over her chest anteriorly and posteriorly that this sign was less valuable. Coaretation of the aorta is much less common in females than in males. When it is present, it is apt to be in an unusual location or complicated by some additional lesion. This patient 's coaretation was in the usual location, but the presence of an associated cardiac lesion was suggested by the loud systolic murmur over the heart and chest that were present from infancy. The murmur of a coaretation itself is soft and is heard better posteriorly over the descending aorta than it is over the heart. With enlargement of the left ventricle and dilatation of the mitral valve ring or of the aorta, murmurs of relative mitral insufficiency or aortic stenosis appear, but her murmur was quite loud and unchanging from early infancy, even though her heart was not mnch enlarged. A more likely ex- 43;3 CLINICAL CONFERENCE LEFT COMMON CAROTID ARTERY LEFT SUBCLAVIAN ARTERY #NNOMINATE ARTERY INTERNAL A WAMMARY ARTERIAL COLLATERALS X-,~ -XX- COARCTATION ( /1 A z i.\A l ! WALL OF LEFT Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 SINUS OF VALSALVA ANEURYSM FIG. 3. Left anterior obliquie angiocardiograill 7 seconds after beginning the injection. Left. N-ray Sloshwing hypertrophy of left ventricle, aneurysm of sinus of Valsalva, cOarCtaltioIn of aorta,, and inuterna 1 mrnanima ry arterial collateral vessels. Righ t. Tracing of x-ray. platation is that she had a congenital anomaly of the aortic valve in the form of a bicuspid, slightly stenotie aortic valve or subvalvular ridge. Abnormalities of the region of the aortic valve are commonly associated with coaretation of the aorta. DR. STEWART: In my experience the systolic murmur in adults is heard best anteriorly over the base of the heart. If it is very loud, it may be heard posteriorly as well but it is difficult to be certain whether a murmur heard posteriorly may not be bruit over the collateral circulation. The murmur of aortic insufficiency had been heard in this patient at 12 years of age before she had subacute bacterial endocarditis. It is not uncommon to hear such a murmur in these patients in the absence of any complication. I have thought that the murmur was due to dilatation of the aortic ring by the dilatation of her aorta with the hypertension above the coarctation. Murmurs are not heard in "normal" bicuspid aortic valves. DR. GLENN: The history and findings given by Dr. Engle justified the diagnosis of coaretation of the aorta, aortic regurgitation, and bacterial endocarditis. Demonstration of the exact location of the coarctation enables the surgeon to plan his approach as well as to be forewarned of additional possible abnormalities. Dr. Steinberg, will you review the x-ray findings including the angiocardiograms of the patient ? DR. ISRAEL STEINBERG: The conventional roentgenograms showed left ventricular enlargement. There were absence of the aortic knob and posterior indentation of the esophagus by a dilated descending aorta. Rib notehing was present bilaterally from the fourth to seventh ribs. Angiocardiography showed coaretation of the aorta at the usual site just below the origin of the left subelavian artery (fig. 3). There was dilatation of the ascending aorta and brachiocephalic arteries, and large arterial collateral vessels were seen. A COMPLICATED COARCTATION OF AORTA Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 2.2-cm. saccular aneurysm of the right aortic sinus was clearly visualized. DR. GLENN: Dr. Steinberg, would you tell us something about your experience with aneurysms of the sinus of Valsalva? DR. STEINBERG: The aortic sinuses are intracardiac and cannot be identified on conventional roentgenography. During angiocardiography they appear as dilatations at the root of the aorta immediately above the aortic valves and are best visualized in the left anterior oblique view. Inconstant filling of the coronary arteries during angiocardiography does not always allow individual identification of the sinuses. However, in the left anterior oblique view the right coronary sinus is regularly anterior to and just behind the sternum. The aortic sinuses are in close relation to all the cardiac chambers, particularly the right atrium and ventricle. The origins of the pulmonary artery, the interventricular septum, and the left atrium are adjacent, whereas the superior vena cava is more distant. Aneurysms of the aortic sinuses (of Valsalva) are rare and are either congenital or acquired. The acquired types are chiefly due to syphilis- or bacterial endocarditis. The congenital aneurysms are thought to be due to a development defect in either the aorticopulmonary septum or the elastic tissue of the aortic sinuses. Edwards and Burchell attribute congenital aneurysms to lack of continuity between ,he aortic media and aortic ring. In aortic sinus aneurysms the wall is made up of the atrium instead of aortic media; pressure within the aorta causes bulging of the sinus, producing an aneurysm. In an 11-year period, during which over 3,000 patients were studied by the intravenous method of angiocardiography, 25 cases of unruptured aneurysms of the aortic sinus have been diagnosed at this center. Ten were acquired; 9 were due to syphilis and 1 was due to arteriosclerotic dilatation of the thoracic aorta. Fifteen were congenital and of these 6, including the case herein presented, were associated with coarctation of the aorta. 437 One patient had aneurysmal dilatation of the aortic sinuses and pseudocoarctation of the aorta while another had associated aortic and mitral valvular disease. Seven patients had arachnodactyly. Aneurysmal dilatation of the aortic sinuses was found in all the cases except the one reported here; in this, the right aortic sinus alone was aneurysmal. Aortic regurgitation, which is common in patients with aortic sinus aneurysms, has been attributed to dilatation of the aortic ring and was present in all the acquired cases of aortic sinus aneurysm. In congenital aortic sinus aneurysms, anomalies of the aortic cusps have been frequent at autopsy. In our series, in addition to the case described above, aortic incompetence occurred in a patient with arachnlodactyly. Congenital aortic sinus aneurysms are paper thin and have a tendency to rupture into the structures of the right side of the heart. When perforation occurs, severe overloading of the right cardiac chambers, pulmonary hypertension, and intractable heart failure follow. Sudden onset of dyspnea associated with a machinery murmur suggests rupture of the aortic root with creation of an aorticocardiae fistula. Confirmation of this event may be obtained by cardiac catheterization. The incidence of aneurysm of the aortic sinuses in coarctation of the aorta is difficult to estimate; it occurred 6 times among 128 patients with coaretation of the aorta studied angiocardiographically at this center. The ages of patients varied from 13 to 27 years with an average of 21 years. Five were males and 3 females. Only 1 was a Negro. Three patients were asymptomatic although a history of previous hypertension or heart murmurs was present in every instance. Headache was present in 2, while 1 had bacterial endocarditis. Systolic murmurs (grade IIl to IV) transmitted to the axilla and back, especially over the suprascapula area and similar to those usually found in coaretation of the aorta, were common. In all cases of aneurysmal dilatation of the 438 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 aortic sinuses and coaretation there was enlargeinent of the heart, especially the left ventricle. Deformity of the aortie arch and rib notching were constant findings. Angiocardiography provided the definitive diagnosis of aortie sinus aneurysm and demonstrated the point of eoaretation. In the literature there is also a report of a right aortic sinus diagnosed by retrograde aortography. DR. GLENN: Thank you. That is a beautiful demonstration. Dr. Eiigle, will you tell us more of her hospital course ? DR. ENGLE: While these studies were being performed, the patient ran a low-grade fever, around 37.6 C., and had a persistently elevated white cell blood count and sedimentation rate. The possibility of incomplete cure of the subacute bacterial endocarditis was raised. DR. GLENN: Dr. Stewart, what should be done to evaluate such a situation? What therapy would you recommend for bacterial endocarditis ? DR. STEWART: A persistent search should be made for embolic manifestations: peripheral petechiae in nailbeds, fingertips, eyegrounds; repeated blood cultures at the height of the fever. Arterial blood cultures have not been more effective in securing positive blood cultures than venous blood. The most common organism that causes subacute bacterial endoearditis in this defect is the Streptococcits virida ss. Should the blood culture be positive, an optimal course of therapy should be instituted. It is the general experience that more relapses occur in patients treated for the shorter periods and with the smaller dosage schedules. Accordingly one starts out on a 6-week program of a total of 4 to 6 million units of sodium penicillin G every day, given in divided doses at 2-hour intervals intramuseularly. If later tests indicate that the strain of the organism is a nonresistant one, the amount of penicillin is increased. On occasion the treatment may be stopped at 4 weeks. If there is need for attempting to treat for a shorter period, a rapid 2-week "combined " CLINICAL CONFERENCE therapy course may be used, namely, a total of 6 million units of sodium penicillin G intramuscularly in divided amounts every 2 hours, every day, and a total of 2 Gm. of dihydrostreptomycin (or 1 Gm. of streptomycin and 1 Gm. of dihydrostreptomycini) in 4 doses intramuscularly as originally described by Robbiiis and Tompsett. If repeated blood cultures are negative but subacute bacterial endocarditis is still likely or suspected, a course of therapy should be given. Since 1 out of 5 instances of subacute bacterial endocarditis with positive blood cultures is due to enterococcus, it is best to treat those with negative cultures as though they are of this worst type and give the combined therapy for a period of 6 weeks. DR. GLENNX: Dr. Stewart, will you pull together the diagnosis that finally emerged? DR. STEWART: It was apparent that the patient had coaretation of the aorta with very high blood pressure above the coaretation, but w-ith good collateral circ(llation. There was the murmur of aortic insufficiency. The angiocardiogranm showed the coarctation to be located below the left subelavian artery, and also denionstrated an aneurysm of the sinus of Valsalva. The patient had had 2 episodes of bacterial endocarditis or endarteritis, the last one fairly recently. There was no w-ay of ascertaining whether the sinus of Valsalva wxas the site of the implantation, or perhaps an associated bicuspid aortic valve, or the coareted segment. She was a patient with a complicated background who was presented for correction of the coaretation of the aorta. DR. GLENN: We anticipated 2 hazards in particular with this patient. The first was that an increase in the blood pressure following the application of occluding clamps prior to resec tion of the coareted segment might result in a rupture of the aneurysm of the sinus of Vtralsalva. The second was the possible requirement of prolonged occlusion of the aorta because of technical difficulties that might arise from the result of a long-standing infection, the bacterial endocarditis. Dr. Stewart, how soon is it safe to operate COMTHPLICATED COARCTATION OF AORTA Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 after recent subacute bacterial endocarditis? DR. STEWART: Dr. Glenn, with this patient with slight fever only, who had coaretation of the aorta with Avery hi(rgh blood pressure and an aneuryssm of the sinus of Valsalva, the possibility of its rupture indicated that repair of the coarctation, if it could be done, should be carried out as soon as possible. To this end she was given a 2-week course of 1)enicillin therapy and was discharged afebrile on DVcember 6. Because of nocturnal cough, dyspiiea, and orthopniea as eviidelice of early heart failure, the patient was digitalized. Shle was readmitted on February 13, a)Jroximately 21/2 months later. This period of time was allowed to permit healing of the endocarditis and formation of strong scar tissue in the aneurysm of the sinus of V'alsalv a inl case this was involved. DR. GLENN: Dr. Artusio, what problems does this patient Present to tile anie.thesiologist ? DR. JOSEPii ARTU SIO: We have used diethyl ether in this clinic to accomplish a light level of anesthesia, which we have termed analgesia. The level is one in which there is minimal depression to respiration and circulation, and the patient frequently is oriented as to place but is completely analgesic and has no memory of the experience. At this level of anesthesia the patient has optimal reactivity to the stresses of surgery, blood loss, extreme positions on the operating table, and change of position on the operating table. Premedication consisted of a small dose of atropine, 0.2 mg., and in order that the circulation not be embarrassed by the presence of an opiate, none was used. A 250-mg. dose of thiopental sodium, in a 2.5 per cent solution, was given for the psychic sedation afforded the patient, so that she would not fear the anesthetic mask. Nitrous oxide-oxygen was started, with an 8-L. flow of 75 per cent nitrous oxide and 25 per cent oxygen, and ether was gradually added to the mixture until the patient entered a light level of surgical anesthesia. At that time, under direct vision, the pharynx and larynx were sprayed with 2 per cent Xylocaine for topical anesthesia, a 38- 439 French cuffed endotracheal tube was inserted into the trachea, and the patient was immediately returned to the analgesic state of anesthelsia where she responded to the spoken voice. Since this patient had an aneurysm of the sinus of Valsalva in association with her coaretation of the aorta, we were most concerned that during the period in which the proximal aorta was clamped the blood pressure should not rise unduly and produce rupture of the aneurysm. It was planned to use Arfonad, a thiophanium derivative, which would induce ganglionic blockade in the periphery and control the height of the blood pressure. llowever, from previous experience with this (ompound we knew that the desired hypotension was not always achieved. This resistance to hypotension is particularly true in the youmigr adult group to which this girl belonged. Thus it was considered that if Arfonlad did not produce the necessary hypotension, eoncomitant hypothermia might aid to control blood pressure. Actually Arfonad worked very well and we were able to reduce the blood pressure at will. The blood pressure before the aortic clamps were applied was 230/80 mm. Ilg with a pulse rate of 80. Arfonad was started by intermittent injections of 3 mg. followed by a 0.1 per cent adjustable drip. In this manner the blood pressure was maintained within a range of 140 to 200 systolic. Following the anastomosis the blood pressure leveled off to 170/80. DR. GLENN: Dr. Holswade, what are the advantages of hypothermia in this situation and how was it used? DR. GEORGE R. HOLSWADE: It was hoped that by cooling the patient to approximately 39 C. the blood pressure would fall subsequent to a decrease in cardiac output and would not rise precipitously during the occlusion of the aorta. When surface cooling of the body occurs, there is often a short initial rise in blood pressure due in part to peripheral vasoconstriction and possibly to shivering in some cases. But as the cooling progresses, the blood pressure falls in a curve CLINICAL CONFERENCE 440) Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 that is parallel to that of the temlperatnre and to that of the cardiac output. Cooling in a patient such as this should not be carried to a rectal temperature lower that 31 or 32 C. In this temperature range there is little danger of serious cardiac arrhy thmias. This degree of hypothermia might provide just enough slowing of heart action, just enough decrease in cardiac output and just enough hypotensive effect to prevent, a rupture of the aneurysm of the sinus of Valsalva when the aorta is cross clamped. For this reason it seemed advisable that the patient be cooled while the chest was being opened and the coaretation was being dissected free. Cooling of the patient did not delay the operation. It was easily accomplished by pumping a cold alcohol solution through special rubber blankets (Thermo-rite), which were placed beneath the patient and over the lower portion of the body. To further speed up the cooling process plastic bags filled with crushed ice were packed around the patient. The temperature was reduced to 32 C. and maintained at that level until the anastomosis was completed. Warm water at 44 C. was then pumped through the rubber blankets. The patient remained on the operating table until her body temperature had returned to 35 C. She withstood the procedure extremely well and was awake at the end of the operation. DR. GLENN: The operation was accomplished with little more than the usual effort required for an adult with a coaretation. There was a very luxuriant collateral circulation. The intercostal arteries near their origin from the aorta were almost aneurysmal. Three pairs were divided. The internal mammary was very large. The heart was enlarged, the left ventricle being quite prominent, its wall hypertrophied. The proximal aorta at its origin was enlarged and a coarse thrill was felt in systole, but perceptible in diastole. A saccular aneurysm of the right aortic sinus measured 2.2 em. in diameter, and projected 2 em. above the surrounding cardiac surface. It had an egg-shell consistency and expanded very little on contraction of the left ventricle. Probably it was B. FIG. 4. Findings at operation. A. Coaretaltion located 4 em. distal to stlubelavia.i. Aorta distal to it enlarged, jet plaque palpable 2 emi. beyond on the left lateral asl)eCt of arterial all. B. Liga- mentum a rteriosum entered coareted segmnent proximal to diaphragm. The lumien of the diaphragm was slit-like and measured 2 mm. in its greatest diameter. C. Wall of eoarle te(l segnuienit at level of the diaphragm. X 12. partially obliterated and, in the belief that it might further decrease following the lowering of the blood pressure after resection of the coarctation, it was left unmolested. Furthermore, it has been demonstrated that the initracardiac approach seems to be the avenue of preference. The coareted segment measured 1 ce. in length, and in its midportion as it was held forward on slight tension, a diaphragm could be palpated. A palpable thrill was quite evident, with a jet that, could be felt most distinctly 2 cm. beyond on the left lateral aspect of the dilated distal segment. Here there was a definite "jet plaque." The ligamenitum arteriosum entered the coareted segment just proximal to the diaphragm. It measured 1 em. in length and 0.3 em. in diameter. On palpation it seemed tubular and possibly patent but there was no thrill. It was divided, tiAe aortic half was patent but 441 COMPLICATED COARCTATION OF AORTA Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 the 1l)ilniollary portion was obliterated (fig. 4A). Clamps were placed proximal and distal to the coaretation. There was an elevation of the blood pressuire from 160/80 to 220/90 mm. Hg. The coareted segmienit was reseeted, and an aniastomliosis was done. This required almost 30 minutes and during this period the 1loo0( pressure, althougrh fluctuating betweeni 210/90 and 130/80, leveled off at 170/80, being controlled with Arfonad. After completion of the aniastomosis the distal clamp was removed and then the proximal (clam}a) was gra(nallyak released over an interval of 15 mniitecs. The blood pressure did not fluetuate thereafter and remained at 170/80. The lnmeii of the diaphragm ini the resected semeint was slit-like in shape andl measured 2 mni. ini its greatest (liameter. There were numerous; liniear bright yellow fibronis plaques in the diaphragm aln( the adjacent wall of the aorta (fig. 4B). The wa'all of the aorta was thickened in the area of (coar(atioll and its pattern was somewhat disrlu)ted (fig. 4C). At the jinetion of the thickened poortion and the more normal vas(enlar w-all there was ani atheromatous area conisistingt of a colleetion of large mononuclear plhago(ytes with foamy- cytolasm. Connectiv\e tisslle was abundant ini the wall of the aorta an(1 ini the area of diaphragmatic narrowing of the coaretation the usual parallel pattern hlad disappeared and the fibers were tangrled, twisted, and turned npoIi one another. Her immediate postoperative course was unevenitfnil and without complications. She was discharged 3 weeks later. At that time the blood pressures were right arm 150/55; left arm, 160/60; right leg, 210/110; left leg, 200/100. Dr. Engle, what has happened to this patient since she left the hospital? DR. ENGLE: After convaleseenc( e she returnied to her regular occupation as a freelance writer. It is now 21/2 years since the patienit 's operation. She states that she has never been so energetic or untiring. She can climb 3 or 4 flights of stairs before her legs fatigue. She does not experience shortness of FIG. 5. wOPcntgenlogralil 30 months after resect ion of eo .llreta.tioi showving decrease in size of left v eii~ tricle. breath, aiid she sleeps flat comfortably. She no longer takes a digitalis preparation. Her blood pressure is 130/50 - 30 mmn. Hg in the arms and 140/50 ill the legs. Exaggerated intercostal pulsations are gone. The aortic systolic mnurmur and the diastolic murmur of the aortic inisuffieiency persist. The aortic pulsation in the suprasternal notch is still evident. Tlie heart size is less by 1 em. than preoperatively, and this improvement is due chiefly to a decrease ill left ventricular size (figy. 5). There is Iio loniger evidence of left atrial enlargement, and the ascending aorta is smaller. 11er electrocardiogram continues to show left ventricular hypertrophy and "strain." Thus the manifestationis of (oaretation of the aorta have disappeared. Relief of this cardiac. burden has apparently made her better able to withstand the aortic valve involvement. Objectively, as well as symptomatically, she is better. She will continue under medical supervision. DR. STEWART: Dr. Glenn, what has been our experience with aortic insufficiency in coaretation of the aorta? DR. GLENN: Aortic insufficienicy is seeni ill coaretation under 3 circumstances. The first is believed to be due to prolonged hyperten- CLINICAL CONFERENCE 442 Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 sion that produces enlargement of the proximal aorta and the aortic ring at the level of the valves. Secondly the aortic valve may have only 2 leaflets instead of 3, and slight enlargement of the aorta may result in insufficiency. Then in the third group there are those instances where disease such as bacterial endocarditis or rheumatic heart disease may cause a loss of valve substance that results in insufficiency. Our experience with aortic insufficiency associated with coaretation of the aorta is limited. We have operated upon 4 such patients. All 4 tolerated the operation well. With a return of the blood pressure to normal, 1 patient lost the signs of insufficiency. Another, although experiencing relief from the preoperative hypertension, continued to have signs of aortic insufficiency and increasing left heart failure, and died almost a year later. The other 2 patients have had a persisteuee of definite evidenc(e of nor- tie regurgitation l)ut are definitely improved. This patient, our fifth with aortic insufficiency, continues to have a systolic and diastolic murmur along the left sternal border. Evidently she has a definite aortic regurgitation, now 30 months after operation. DR. STEXVART: Durinog the course of the 30 years of this woman 's life, advances in medicine and surgery have come along just in time to help her out of difficulty: antibiotic therapy for subacute bacterial endocarditis and surgery for removal of the coaretation. If she should later need help because of aortic insufficiency or rupture of anl aneurysm of the sinus of Valsalva, these conditions too are now within the ever-widening area of cardiovascular lesions, both congenital and acquired, that are aimieniable to surgery. Close teamwork of the medical and surgical specialties interested in this field has made possible these great steps forward. 9 Welch, J. S., Kirklin, J. W., Ellis, F. H., Jr., and Bruwer, A. J.: Resection and Grafting for Chronic Occlusion of the Terminal Aorta or Iliac Arteries. J.A.M.A. 164: 1045 (July 6), 1957. The recent Mayo Clinic experience in the management of aortic and iliac arterial occlusive disease is described. In the present series of 99 patients, intermittent claudication was the chief symptom and the status of the leg pulses was the most important physical finding. Preoperative aortography was done routinely in order to define the extent of the occlusions. Technical aspects of resection of the obstructed vessels and homograft reconstruction are outlined. Excellent operative results were obtained in 71 patients (72 per cent) as indicated by complete relief of symptoms and return of leg pulses. Five deaths occurred, all postoperatively. The most important factor in the success of this surgery is insuring that the distil alnastomosis is made to a patent artery, if necessary to the superficial femoral. ROGERS Coarctation of Aorta Complicated by Bacterial Endocarditis and an Aneurysm of the Sinus of Valsalva FRANK GLENN, HAROLD J. STEWART, MARY A. ENGLE, DANIEL S. LUKAS, JOSEPH ARTUSIO, ISRAEL S. STEINBERG and GEORGE R. HOLSWADE Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 Circulation. 1958;17:432-442 doi: 10.1161/01.CIR.17.3.432 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1958 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/17/3/432.citation Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/