Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
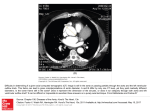
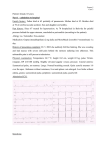
Optimal reconstruction phase of ECG-gated CT angiography in the diagnosis of acute thoracic aortic pathology (work-inprogress) Poster No.: R-0134 Congress: 2014 CSM Type: Scientific Exhibit Authors: D. Hocking, A. Gupta; FREMANTLE/AU Keywords: Cardiovascular system, Emergency, CT, CT-Angiography, Technical aspects, Artifacts DOI: 10.1594/ranzcr2014/R-0134 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply RANZCR/AIR/ACPSEM's endorsement, sponsorship or recommendation of the third party, information, product or service. RANZCR/AIR/ ACPSEM is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold RANZCR/AIR/ACPSEM harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, .ppt slideshows, .doc documents and any other multimedia files are not available in the pdf version of presentations. Page 1 of 13 Aim Helical multi-detector row computed tomography (MDCT) has an established role in the diagnosis of acute aortic pathology. Motion-free visualisation of the aortic root and ascending aorta allows the radiologists to make a confident diagnosis and can aide with surgical planning. Retrospectively ECG-gated scans acquire complete data throughout the cardiac cycle and are reconstructed at a specified point in the R-R interval, significantly reducing motion artifact [1]. Optimal reconstruction phase varies depending on the structure being evaluated and the patient's heart rate. Figures 1-3 illustrate the difference in quality between ungated CT (Fig. 1 on page 2), incorrect phase of gated CT (Fig. 2 on page 3) and correct phase of gated CT (Fig. 3 on page 4) at similar levels in the same patient. Current protocol at our institution is to reconstruct a 75% phase when the heart rate is less than 80 beats per minute (bpm) and a 40% phase for heart rates greater than 80 bpm; a practice which is based on operator experience. Similar past research by MorganHughes et al. has suggested a statification threshold at 70 bpm, with best phases at 75% and 50%, respectively [2]. However, this prior study utilised older equipment and the 50% phase did not reach statistical significance. This study aims to test the hypothesis that images are optimally reconstructed either during the end-systolic phase (35-45%) or the mid-diastolic phase (70-80%) and to establish the heart rate threshold where the transition occurs. The results will serve to form the basis of a standardized, evidencebased protocol for departmental use. Images for this section: Page 2 of 13 Fig. 1: Selected, non-consecutive axial slices from the level of the tubular ascending aorta (top left) to the aortic root (bottom right) in an un-gated CT pulmonary angiogram performed in an individual patient (Patient 8). The heart rate was not recorded at the time of the scan. Images demonstrate extensive motion artifact at all levels, which could be misinterpreted as an intimal flap (arrows). Page 3 of 13 Fig. 2: Selected, non-consecutive axial slices from the level of the tubular ascending aorta (top left) to the aortic root (bottom right) in a retrospectively gated CT angiogram targeted to the thoracic aorta. This was performed in the same individual patient shown in Figure 1 (Patient 8), shortly after the ungated CT scan. The heart rate was 75 beats per minute at the time of imaging. Images have been reconstructed at the 75% R-R interval. The presence of motion artifact is reduced compared to the ungated study, but remains present to a lesser degree (arrows). Page 4 of 13 Fig. 3: Selected, non-consecutive axial slices from the level of the tubular ascending aorta (top left) to the aortic root (bottom right) in a retrospectively gated CT angiogram targeted to the thoracic aorta. This was performed in the same individual patient shown in Figure 1 (Patient 8), shortly after the ungated CT scan. The heart rate was 75 beats per minute at the time of imaging. Images have been reconstructed at the 40% R-R interval. Almost no motion artifact is visible. Page 5 of 13 Methods and materials Equipment and CT Scan Parameters All patients were scanned on a 64-slice multi-detector row CT scanner (Philips Brilliance 64 running under the V.3.5.5.5 2007 11 Aprl 2013 software ugrade). The scan protocol included dual scout views, followed by un-enhanced thoracic CT and subsequent contrast enhanced aortic angiogram from the aortic arch to the aortic bifurcation, using a retrospective ECG-gating technique. Contrast phase scan parameters were as follows: 64 slice helical mode, collimation 0.625mm, 512 pixel matrix, pitch 0.299mm, gantry rotation time 0.4 seconds, FOV 350 and 120 kV tube voltage. Tube current varied by patient size, ranging between 300-600 mAs. Iodinated intravenous contrast was injected with an automated power injector. Optimal contrast timing was achieved with bolus tracking. For the purposes of this study, axial images were reconstructed at 3mm slice thickness at 10% intervals between 20-80% of the R-R interval. Additional phases at 35%, 45% and 75% were also included to more closely investigate end-systolic and middiastolic phases. Quality assessment was determined exclusively from the reconstructed axial data. The complete CT study data was transfered to a departmental research harddisc drive, which was utilised exclusively during image analysis. Patient Selection Consecutive patients ungergoing electrocardiogram-gated (ECG-gated) CT thoracic angiography, performed on the institutional emergency department CT scanner, during the trial period between 15th February 2014 and April 20th 2014, were included in study data collection. One patient was later excluded due to uniformly high quality images throughout all phases, limiting assessment for "best phase." Data Gathering A unique, anonymized patient identifier was issued to each patient. Age and gender were recorded. The mean patient heart rate during the CT scan was recorded for each patient, as obtained from the ECG performed by the CT scanner at the time of imaging. The heart rate regularity and presence of acute aortic pathology were noted. The images were subjectively evaluated for the "best phase" as defined by the phase with the least overall movement artifact at the aortic root and within the tubular ascending aorta. As the workstation software presented the phases in order of phase, the investigators were not blinded to the phases at the time of scoring. Assessment was by two independant investigators, one radiology registrar with 3 years of experience and an experienced thoracic radiologist. Consensus on disconcordant results was achieved through discussion. Tabulated findings were recorded in a Microsoft excel spreadsheet stored on an institutional research drive. Page 6 of 13 Statistical Analysis Statistical analysis was performed by an experienced biostatistician using the Stata/ SE v13.1 software package. Inter-rater agreement and reliability were assessed using the intraclass correlation coefficient and mixed-effects ML regression, respectively. Correlation between heart rate and best phase was assessed via random effects logistic regression analysis to evaluate overall relationship. Two-sample Wilcoxon rank-sum test was performed to establish significance between high and low heart-rate groups. Results A total of 20 patients were scanned during the study period. The majority of patients were male (15/20; 75%). The mean age was 58.0 years (SD 12.2, range 25-76). The mean heart rate across the study population was 63.5 beats per minute (SD 17.6, range 46-101). All patients included in the study had a regular heart rate. Acute aortic pathology was present in 3 cases. Patient demographics and observer findings are provided in Table 1 on page 8. Summary of results are presented in Table 2 on page 8. Inter-Rater Reliability The inter-rater reliability was good, with an intraclass correlation coefficient of 0.63 (95% CI 0.34 - 0.84). There was no difference in the reliability of ratings based on mixed-effects ML regression (p = 0.903). In one case (Patient 14), one investigator did not generate an opinion as to the best phase due the impression that all phases in the study were of equally high quality. This patient was excluded from "best phase" analysis as consensus could not be reached. Of the remaining cases, difference of opinion occured in 13 of 19 cases (68%). Of these disagreements, 3/13 (8%) were due to major variance of opinion between end-systolic and mid-diastolic "best phase". At consensus, in all three cases the variance was due to motion being minimal at the aortic root during the end-systolic phase, but minimal in the tubular ascending aorta during the mid-diastolic phase (Fig. 4 on page 9), with differening initial opinion as to which constituted better overall image quality. At consensus, the overall best image quality was determined to be during mid-diastole. In 5/13 cases (38%), disagreement was due to a lack of perceptible difference between the phases initially selected by the investigators. In these cases, consensus reflected both phases, as neither could be considered of superior quality. In the remaining 5/13 (38%), minor differences were visible, but did not alter the preferred phase group. Best Phase of Reconstruction Analysis was performed on mixed investigator scores (n = 38) and consensus results (n = 19). Pictorial representations of individual and consensus results are provided in Fig. 5 Page 7 of 13 on page 10 and Fig. 6 on page 11, respectively. There was a significant correlation between heart rate and best phase (p = 0.015; random effects logistic regression). The best phase fell into two significantly different groups (p < 0.0001; Wilcoxon signed-rank test), summarised in Table 2 on page 8. At higher heart rates (mean 88.6 bpm, range 75 - 101, SD 13.0), the mean "best phase" was 39% (range 30-45%) correlating with endsystole. At lower heart rates (mean 56.3 bpm, range 46 - 76, SD 8.8), the mean "best phase" was 74% (range 70-80%) correlating with mid-diastole. Based on the available data, a best estimate threshold value between the two groups is at 75 bpm. However, the sample size is too small to confirm this value. Images for this section: Table 1: Tabulated data from all patients including anonymised patient identifier, age, gender, individual investigator "best phase" preference and consensus results. * indicates an absent score. A preference was not indicated by investigator 2 in this patient due to uniformly high image quality across all phases. A consensus was not reached. Page 8 of 13 Table 2: Summary of final results derived from the study data. Values in parentheses indicate percentages. Page 9 of 13 Fig. 4: Selected, non-consecutive images obtained during retrospectively ECG-gated CT angiogram of the thoracic aorta (Patient 19). Images on the left demonstrate the 80% phase and images on the right demonstrate the 40% phase. Motion artifact is present in the 80% phase at the level of the aortic root (bottom images), but not seen in the tubular aorta (top images). The contrary is true in the 40% phase (right images). Arrows indicate location of wall motion artifact. Page 10 of 13 Fig. 5: Scatterplot showing mixed investigator scores for best phase of reconstruction (yaxis) relative to heart rate (x-axis). Investigator 1 scores are shown in blue. Investigator 2 scores are shown in green. The distribution suggests a bimodal relationship. Fig. 6: Scatterplot showing consensus for best phase of reconstruction (y-axis) relative to heart rate (x-axis). The distribution suggests a bimodal relationship with a transition heart rate threshold in the region of 75 beats per minute. Page 11 of 13 Conclusion This study demonstrates a significant correlation between heart rate and optimal phase of image reconstruction at retrospectively ECG-gated CT angiography of the thoracic aorta (p = 0.015). The best phase appears to correlate with two statistically significant groups at end-systole and mid-diastole (p < 0.0001). Based on these data, reconstruction recommendations are as summarised in Table 3 on page 12. Where the patient heart rate is less than 75 beats per minute, the data should be reconstructed during the middiastolic phase (near to 75%). When the heart rate is above this threshold, the data should be reconstructed in the end-systolic phase (near to 40%). Due to the small sample size, further study is required to confirm the 75 bpm threshold. Images for this section: Table 3: Summary of recommendations derived from the study results. The 75 beats per minute threshold is provided as a best estimate, based on the available data. Page 12 of 13 Personal information Dr David Hocking is a third year trainee registrar in the Western Australia Radiology Training (WART) program, based out of Royal Perth Hospital. Dr Ashu Gupta is a consultant radiologist at Fremantle Hospital in Perth, Western Australia. He has a special interest in chest and cardiac radiology. References 1. 2. Roos JE, Willmann JK, Weishaupt D, Lachat M, Marincek B, Hilfiker PR. Thoracic aorta: motion artifact reduction with retrospective and prospective electrocardiography-assisted multi-detector row CT. Radiology. 2002 Jan;222(1):271-7. Morgan-Hughes GJ, Owens PE, Marshall AJ, Roobottom CA. Thoracic Aorta at Multi-Detector Row CT: Motion Artifact with Various Reconstruction Windows. Radiology. 2003 Aug;228(2):583-8. Page 13 of 13