Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
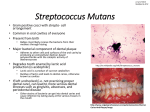
REVIEW ARTICLE The Microbial Ecology of Dental Caries G. H. W. Bowden From the Department of Oral Biology, Faculty of Dentistry, University of Manitoba, 780 Bannatyne Avenue, Winnipeg, Manitoba, Canada R3E 0W2 Correspondence to: George Bowden, Department of Oral Biology, Faculty of Dentistry, 780 Bannatyne Avenue, Winnipeg, Manitoba, Canada R3E 0W2. Tel: + 1 204 789 3595; E-mail: george – [email protected] Microbial Ecology in Health and Disease 2000; 12: 138–148 The microbial ecology of caries is complex and incorporates mechanisms common to the natural colonization of the host and to plaque accumulation at sites that do not develop caries lesions. It is not simply accumulation of plaque in the oral cavity but also the ecology of oral bacteria among the host population and the ecology of organisms in the lesion. In these three habitats odontopathogens and other oral bacteria can undergo genotypic change, which may produce phenotypes more virulent or better able to survive specific evironments. Adaptation and response to stress will also enhance bacterial survival and selection. Therefore, in these habitats diversity is generated and this, coupled with adaptation, provides strains that are selected to be best suited to specific environments, including cariogenic environments. In this way odontopathogens may be selected and become more numerous among hosts in a population. The most common ecological mechanism associated with caries is bacterial succession, and dominance of the plaque community by mutans streptococci. However caries is the outcome of interactions within the plaque community, host physiology, diet, fluoride, pH and the nature of the tooth enamel, and dominance by mutans streptococci does not always produce a lesion. Caries can be reduced by bacteria that degrade lactate or produce base from urea and salivary peptides, while other bacteria, including a group of ‘low pH’ streptococci could lower the pH of plaque, and produce enamel demineralization. In addition, the plaque biofilm not only serves as a habitat but includes in its structure a fluid phase (plaque fluid) and a matrix that have a direct influence on the physiology of plaque bacteria and the formation of a lesion. Given the complexity of the microbial ecology of caries even with the elimination of mutans streptococci caries would most likely persist, albeit at a significantly reduced level. Key words: biofilms, caries, microbial ecology, mutans streptococci, plaque fluid. INTRODUCTION Microbial ecology describes the interaction between microorganisms and the structural, physical and biological components of their habitats and infectious diseases provide examples of the impact of ecology of specific organisms on their host populations of plants or humans and other animals. Moreover, disease promotes responses from the host, changing the ecology between the host and the bacteria, influencing the well-being and activities of the host population (1). Examples of the responses of host populations that affect microbial ecology include vaccination, to reduce the ability of bacteria to colonize the host and delivery of fluoride in water and dental products that modifies bacterial metabolism and reduces the incidence of caries. Considering microbial ecology and its outcomes, at the level of infectious disease with a specific pathogen (2–5) makes it clear that complex mechanisms are involved and assessing their function in nature is a difficult task. This problem is made more complex when, as is the case with dental caries, odontopathogens are usually components of the resident flora of the host, unlike many other overtly pathogenic bacteria. Analysis of microbial ecology has been simplified to some extent by limiting studies to a selected stage or © Taylor & Francis 2000. ISSN 0891-060X sequence of stages in the ‘life cycle’ of a specific bacterial strain, a species, or a bacterial community. This approach has been taken with oral microbial ecology, where study is usually made of the stages of plaque accumulation, the biology of specific bacteria or selected microhabitats, and plaque physiology. However, studies of the ecology of oral bacteria in caries have not been limited to their activities in the mouth. A role for the human host population as a reservoir for mutans streptococci (6) has been considered in relation to transmission among hosts (7 – 9) and in approaches to prevent caries in humans (10, 11). Also, studies of antibiotic resistance and specific genes of individual strains of oral bacteria have revealed evidence for transfer of genetic characters that enhances their diversity (12 – 15). Furthermore, the ecology of caries includes not only the processes that cause destruction of enamel but also those that promote bacterial invasion of dentine. Clearly, the microbial ecology of caries involves at least three easily recognizable areas, 1. Bacterial ecology among the host population, 2. The ecology of the plaque community, 3. The ecology of the community within the lesion. Figure 1 shows the relationships between areas 1 and 2, which determine the composition and contribute to the microbial diversity of the oral flora of an individual host. Microbial Ecology in Health and Disease The microbial ecology of dental caries There are several reviews and book chapters that discuss the microbial ecology of caries (16–20). Consequently, this review will try to emphasize and discuss areas that are problematic and those that require more study. THE COMPLEXITY OF ORAL MICROBIAL ECOLOGY AND CARIES A problem in understanding microbial ecology of caries is that many of the events that lead to the development of a caries lesion are common to those associated with healthy enamel. In human nursing caries S. mutans can predominate at sites that develop a white spot and those that do not. This can occur even at adjacent susceptible sites in the same individual (21). Similarly, van Ruyen et al. (22) have shown no significant difference between the numbers of ‘low pH isolates’ from white spot lesions and normal enamel in subjects with caries. Explanations for such observations include suggestions for local environmental differences and ecological mechanisms that could modify the microflora to reduce its cariogenic potential (17, 19, 20, 23). The significance of the presence of mutans streptococci, diet and dietary sucrose, fluoride, poor oral hygiene and host antibodies on caries in 6i6o is well accepted. However, some other factors that may be involved such as 1. Complex interactions among cells within the dental plaque biofilm (24), 2. Novel expression of genes during biofilm formation (25, 26), 3. Stress responses by oral bacteria (27), and 4. The ability of bacteria to modify local environments (23, 28) may often be supported predominately by findings in 6itro. Confirmation of their roles in caries in animals or preferably in humans, is an important topic for research in oral microbiology. In 6itro study of mechanisms is essential to aid in developing strategies for prevention and control of caries however, the true value of 139 any strategy has to be confirmed in 6i6o and preferably in humans. A second significant point is that although many aspects of the caries process are common among hosts they may be influenced by factors that reflect the individuality of a person and their microflora. The common processes include adhesion, co-aggregation, growth and survival, which are basic to bacterial colonization of the mouth (29 – 32). However, genetic variation among hosts, their habits and immunological history (e.g. disease, vaccination), together with the variety of habitats in a given mouth, and the diversity among strains of species of oral bacteria that colonize a host are unique to a person. Therefore, while general observations can be made of microbial ecology and the development of a carious lesion it has to be recognized that host specific factors also influence the process. SIGNIFICANT FACTORS IN THE MICROBIAL ECOLOGY OF CARIES Before discussing microbial ecology and caries some of the components and factors shown in Figures 1 and 2 should be discussed. The final outcome of the interaction among these different factors and processes at a specific site on the dentition determines the formation, or not, of a caries lesion. The habitat The oral cavity provides an excellent environment for the growth and survival of bacteria. Although saliva is not a complete nutrient for all oral bacteria some species or consortia of species utilize it as a substrate (30, 33 – 36). Other oral nutrients arise from gingival crevicular fluid and desquamated mucosal cells. Also, in addition to these Fig. 1. The stages involved in colonization of infants by oral bacteria from the host population and the factors that contribute to the diversity among the bacterial populations within the oral cavity and the plaque biofilm. 140 G. H. W. Bowden Fig. 2. Stages in the accumulation of dental plaque, including the factors that contribute towards the metabolic activities of the plaque biofilm that determine the outcomes of oral microbial ecology in caries. physiologically based nutrients, oral bacteria receive an erratic input of variable substrate from the hosts’ diet, an important factor in caries risk (37). Apart from the nutritional components of saliva there are molecules that enhance colonization and those that have an adverse effect on oral bacteria (38–43). Saliva also acts as a buffer, modifying plaque pH and reduced salivary flow, xerostomia and the variation in salivary flow over different tooth surfaces can influence the formation of a caries lesion (44–46). In addition fluoride, which can dramatically influence the carbohydrate metabolism of bacteria is a significant component of both saliva and plaque. Fluoride delivery has proved to be one of the most important anticariogenic strategies available, and its action is based on modification of the ecology of bacteria and interaction with enamel and tooth root (47). The hard (enamel and tooth root) and soft (mucosal) tissue surfaces in the mouth provide a variety of microhabitats with distinctly different structural and environmental parameters. In particular, the non-shedding surface of enamel allows the accumulation of a biofilm that provides a protected habitat with a variety of niches that support a wide range of bacterial genera and species (48, 49). The plaque biofilm is an essential factor in the aetiology of caries. The interactions among the bacteria in dental plaque together with the variations in nutrient, buffer, fluoride, concentrations of various ions and pH in the biofilm determine the formation of a caries lesion. In addition to forming the substratum for dental plaque accumulation enamel and tooth root are the tissues that are destroyed during the formation of a caries lesion. The composition of enamel varies among teeth and even over the surfaces of a single tooth. These variations include the degree of mineralization and also the fluoride content (50, 51). Significantly, the composition of enamel is a determinant in its susceptibility to demineralization and consequently variation in enamel at a site can influence the development of caries lesions (52). Bacteria associated with caries in humans These bacteria are opportunistic pathogens, found commonly as members of the resident flora of persons without caries and expressing their pathogenicity only under specific environmental conditions. Streptococcus mutans and Streptococcus sobrinus, two species of the ‘mutans streptococci’ are the most significant in human caries (16, 19, 53) and studies of the microbial ecology of caries have been directed principally at these species (21, 54 – 56). There is The microbial ecology of dental caries also a strong association between Lactobacillus spp. and caries but little is known of the relative significance of the different species. It has been apparent for years that other genera and species of oral bacteria can either be associated with caries in humans, or cause caries in experimental animals (17, 22, 57–59). In particular, although S. mutans and S. sobrinus are the principal agents of enamel caries, a wider range of organisms is proposed as opportunist pathogens in root surface caries. Generally the organisms other than mutans streptococci and Lactobacillus associated with caries fall into Streptococcus and Actinomyces. Actinomyces odontolyticus, originally isolated from caries lesions (60), colonizes infants before eruption of teeth (61). An association between this species and progressing incipient interproximal caries lesions in humans has also been shown (62). Some root caries lesions are dominated by Actinomyces naeslundii and it has been suggested that strains of this species could play a pathogenic role in this disease (63–66) and recently, A. israelii and A. gerencseriae have also been shown to be present in high numbers in root caries lesions (67). Schüpbach et al., (65) demonstrated the complexity of the bacterial community associated with root caries and most importantly, they correlated the microflora to the state of lesions in extracted teeth (66). The other significant Streptococcus species involved in caries includes Streptococcus mitis (58, 63) and a group of ‘low pH’ aciduric streptococci (68). Recently, these, and other ‘low pH’ isolates (possibly Bifidobacterium and Actinomyces) have been isolated from white spot lesions in humans (22). In contrast to bacteria that lower plaque pH there are others including Veillonella and Actinomyces that degrade lactic acid, thereby increasing plaque pH and reducing its cariogenicity. This proposed anti-caries mechanism has been shown to be effective with Veillonella both in 6itro and in an animal model (69–71). A second bacterial process promoting an increase in plaque pH is the production of base from urea and the arginine containing peptides in saliva (31, 72). Oral streptococci and actinomyces can be protected in low pH environments by expression of urease (26, 73, 74). Recently, studies with recombinant strains of S. mutans in experimental animals have shown that urease production by strains contributed to reduction of caries (75). Also, support for this ‘anticariogenic’ effect comes from studies of plaque pH in 6itro and in 6i6o (76, 77) and from patients with chronic renal failure, who have high levels of salivary urea and show a reduction in caries (78). Di6ersity among strains of species of oral bacteria Although bacterial populations in oral microbial ecology are often studied at the level of species, it is well accepted that phenotypic characteristics among strains of bacterial 141 species can vary. Differences in phenotype may be important in caries if specific variants within the plaque community at localized sites on the dentition were ‘more cariogenic’ or, in contrast, strains had increased capacities to degrade lactate or produce base from urea and salivary peptides, reducing the cariogenicity of plaque. In addition, changes in the phenotypes in plaque could influence bacterial selection and survival (31, 79) and the overall (communal) activities of the plaque community (see below). In the past variations among strains of a species were identified by biochemical, physiological and antigenic differences. Analysis of variation in their enzyme profiles or their genomic DNA (31) has identified more recently individual strains (clones). The DNA typing methods have been valuable in showing the transmission and persistence of clones of oral species within and among their host population and the diversity among clones of a species in a habitat (8, 79, 80). Variations in the genome of daughter compared to parent cells can originate from mutation, transposition and recombination and also integration of DNA from other bacteria (79, 81). Therefore, the genome of strains within oral species may differ, resulting in a species population composed of clonal variants (31, 80, 82, 83). Commensal bacteria, including oral opportunistic pathogens usually, but not always, show more genetic diversity than overt pathogens and very often several different clonal variants will colonize a single host (31, 79). Interestingly, from the aspect of colonization of a host population clones of oral species can have a specific association with a limited group of hosts (84, 85). Although there are data on clonal diversity within oral species there is relatively little on any relationship between such variation and the phenotype or virulence of strains of oral opportunistic odontopathogens (31). In addition to generation of diversity through changes in their genomic DNA strains of species of oral bacteria colonizing a mouth may be influenced by ‘clonal replacement’. In ‘clonal replacement’ new clones replace the existing clones in a habitat and contribute to strain diversity (79). ‘Clonal replacement’ may be more common on mucosal surfaces where cells are shed, compared to the dental plaque biofilm, which provides a retentive and protected habitat. Adaptation by oral bacteria to en6ironmental parameters Apart from ecological advantages provided to oral bacteria arising through changes in their genome they will also adapt (phenotypic adaptation) and respond to environmental stress in order to survive. Generally, adaptive and stress response mechanisms such as tolerance of acid, starvation, oxygen, fluoride and expression of urease (26, 27, 31, 72, 73) that are common among strains of a species can be regarded as having evolved to assist bacteria to survive stresses common to their habitats (86). Phenotypic 142 G. H. W. Bowden adaptation is usually transient and expressed only during stress (31). However, stable adaptation to tolerate xylitol by S. mutans has been shown in 6i6o and although xylitol will normally inhibit the growth of S. mutans, xylitol tolerant strains are selected when S. mutans is grown in 6itro on another carbohydrate (glucose) in the presence of xylitol (87). An important feature of adaptation and survival of bacterial cells in sub-optimal growth environments (e.g. low pH, heat, starvation), is expression of a range of ‘stress proteins’ (88–90). These proteins that promote the survival of the cells in adverse conditions are the subjects of extensive research. Relatively little is known of stress proteins in oral bacteria, although information is accumulating (27). Significant to the current discussion is that adaptation or response to stresses varies among different oral species and among strains of a species, including odontopathogens (91). Responses by bacteria will also include the production of different signaling molecules that influence the activities of the cells within the population (92). Signaling molecules include peptide pheromones that promote competence and cell density dependent peptides in Gram positive and N-acyl homoserine lactones in Gram negative cells (24). These latter density dependent molecules are responsible for ‘quorum sensing’ in bacterial populations, promoting expression of genes when the population has reached a specific cell density. In one case a molecule that seems to act in a ‘quorum sensing’ manner has been demonstrated in an in situ model of dental plaque (93). The biofilm mode of growth Dental plaque is a complex biofilm community where bacterial populations exist as separated micro-colonies in physiologically diverse environments. Biofilm cells exhibit different characteristics from the same cells growing in suspended culture (24). Together with demonstration of the unique characteristics of biofilm cells has come the recognition that bacteria in a biofilm can form a community where the spatially distributed populations may interact (24). Caldwell and his colleagues have described the concept and implications of bacteria growing as communities (94). The activities of a community (communality) are distinct from those of a simple mixture of the same bacterial populations and the community life style provides advantages compared to those of the component populations. The range of habitats for colonization can be extended, resistance to stress and host defenses will increase, and cooperative degradation of complex substrates can take place (24). However, it is important to recognize that the presence of an organism in a biofilm does not necessarily mean that it is part of a community. Some bacterial populations could be present in their defined area of the biofilm, physiologically isolated from other populations, without interaction. The composition of the plaque biofilm community is directly related to the process of formation of a caries lesion. Also, the presence of a biofilm is important in governing the physical changes seen in enamel (95) during the formation of a lesion. Gelatine gels and biofilms of Streptococcus spp. have been used in 6itro to show the importance of such coatings in caries lesion formation and also, their interaction with different ions (96 – 99). Biofilms consist of three physical components, cells, extracellular matrix and a fluid that bathes both cells and matrix. Although the knowledge of the bacterial populations in plaque is far from complete over 300 taxa have been described. Relatively little is known of the composition of the extracellular matrix of plaque in 6i6o (100) but given its relationship to the formation of lesions, the composition of the matrix and factors controlling its composition and production would seem to be an important area for research. However, there are in 6itro studies of the structure and impact of bacterial polysaccharides on diffusion and demineralization (101 – 104). The fluid component of plaque, plaque fluid, plays a significant role in caries and microbial ecology. This fluid can be regarded as the ‘planktonic phase’ of dental plaque and as such its composition reflects not only the outcome of the physiological and metabolic activities of the plaque microflora but also the result of the dynamic interaction between these activities and tooth enamel. Importantly, differences in composition have been shown between plaque fluid from samples of plaque from caries free and caries active persons after sucrose rinses. Margolis & Moreno (105) discuss various aspects of plaque fluid, including variation in composition and the relationships between plaque fluid and demineralization and remineralization of enamel. Although methods are available to analyze the composition of plaque fluid from single tooth surfaces (106 – 108) relatively few studies (97, 98) have been made of plaque fluid from mixed or single culture in 6itro biofilms. Information on the influence that the composition of this fluid has on the physiology of biofilm cells and vice versa, would be very valuable. In particular, the potassium levels in plaque fluid are higher than those in saliva and extracellular potassium levels influence bacterial metabolism (109 – 113). Plaque fluid also probably acts as a ‘carrier’ for substrates, the endproducts of bacterial metabolism and the signal molecules that mediate interaction between bacterial cells. It seems most likely that the channels that run through the plaque biofilm (114) are conduits for plaque fluid. The foregoing has emphasized some of the aspects of microbial ecology that contribute to the complexity of the biology of dental plaque and factors that can influence its cariogenicity. Despite this potential complexity, caries remains a common problem in humans, suggesting that the occurrence of one or more combinations of factors necessary to produce a lesion is also common. It is possible that among these factors are those that may play a greater role The microbial ecology of dental caries than others. Given a normal resident flora, which would include odontopathogens, one can consider diet to be one such dominant factor (37). However, even under dietary conditions that favour caries identical bacterial succession may only produce a lesion on one of two adjacent susceptible sites in the same person (21). MICROBIAL EVENTS LEADING TO THE FORMATION OF A CARIES LESION Plaque accumulation is a dynamic process and central to the microbiology of caries is the concept that the plaque community responds to autogenic (internal) and allogenic (external) stimuli that modify the parameters of the niches available for bacterial populations (16, 48). The changing niches and interactions (24) result in sequential selection of component populations (succession) within the community of bacteria that develops to be in balance with its environment (climax community). Figure 2 shows the stages of accumulation of dental plaque together with the factors described above that can influence the ecology of the microflora during the formation of a climax community, and also the possible outcomes of such accumulation. Two processes that are not mutually exclusive and may be perhaps two stages of the same process can describe the microbial ecology of caries. The most obvious, well described and easily understood is bacterial succession in an environment (e.g. high carbohydrate, low salivary flow) leading to local dominance by mutans streptococci, followed by enamel demineralization and cavitation, that often involves Lactobacillus (16–20). This process probably accounts for the majority of caries lesions in humans. The second process involves different species of bacteria (22, 58, 59, 65, 66) and perhaps, the communal activities of plaque. It is more speculative, with less evidence to support it, compared to dominance by mutans streptococci. Both of these processes are illustrated in Figure 2 and discussed below. Dominance by mutans streptococci The risk of caries in children is influenced by the oral health status and attitudes of their care-givers (115), although isolation frequencies of odontopathogens in children may be independent of their socio-economic background (116). The ease of transmission and colonization of infants and children by mutans streptococci could be regarded as the earliest stage in the process leading to dominance of plaque by these bacteria. Factors influencing the transmission, oral colonization, caries risk and survival of S. mutans among its hosts have been described (6, 7, 10, 11, 117, 118). Clones of S. mutans vary in virulence (119) and selection or generation of more virulent clones of S. mutans within the host population could also influence the process of dominance by this species. 143 Adhesion and coaggregation A wide variety of oral bacteria will have colonized the mucosal surfaces of the oral cavity of infants prior to their acquisition of S. mutans and S. sobrinus. Therefore, mutans streptococci adhering to the newly erupted non-shedding surfaces of teeth do so in competition with a wide variety of established oral bacteria (29). Bacteriocin production is one mechanism that promotes colonization of S. mutans in the presence of other bacteria (117) and detailed analyses of these molecules has been made (120). A second mechanism for adhesion of bacteria to the dentition is by interaction with previously adherent bacteria, through a process described as co-aggregation (32). Co-aggregation of S. mutans with Actinomyces has been shown in 6itro (121) and Veillonella and S. mutans coaggregate in 6i6o (122). Growth and response to the en6ironment Although co-aggregation is significant it is only one of the mechanisms that determines the composition of dental plaque. Two other factors, the growth of bacterial cells in plaque (30), and the survival of strains that cannot grow (31, 79), also play important roles. There is a close association between diet and caries that identifies carbohydrate and acid production by plaque as significant risk factors for caries (19, 22, 37, 123). Dominance by S. mutans or S. sobrinus in areas of the plaque biofilm indicates that a strain or strains of these species occupy a favourable niche with available carbohydrate and a low pH (16, 23). It is the latter parameter that has featured predominantly in explaining the etiology of caries. The relationship between the ‘resting pH’ of plaque, the characteristics of the Stephan Curve including the lowest pH level reached and the time of recovery to the resting pH, are all related to caries risk (123). Selection of aciduric bacteria in plaque environments of low pH remains the central and fundamental concept in the microbial ecology of caries. An unanswered question is whether S. mutans is always responsible for the reduction in pH that gives it an ecological advantage in plaque. Other organisms such as the ‘low pH’ group (22, 124) may initially lower the pH of the local plaque environment and thereby promote dominance by mutans streptococci. Some in 6itro data support a role for other organisms in lowering the pH of communities of oral bacteria sufficiently to decalcify enamel or promote dominance by mutans streptococci (121). Studies in humans using a banding model also suggested that early enamel decalcification, presumably resulting from low pH could occur in the absence of S. mutans (57). However, in this study colonization by mutans streptococci was more common as the bands were left on the teeth for longer periods, suggesting that the early non-mutans organisms produced an environment conducive to colonization by mutans streptococci (125). Recently Van Ruyven et al. (22) have 144 G. H. W. Bowden proposed a model for succession in caries that takes into account carbohydrate intake, ‘low pH’ groups of bacteria and mutans streptococci. In any event, there is substantial evidence that succession in a suitable environment leads to local dominance by mutans streptococci that is associated with formation of a caries lesion. As stated above, it is less easy to explain why under apparently identical conditions, even in a child at high caries risk, S. mutans dominance at an adjacent susceptible site does not always lead to caries (21). In this case, although the environment promoted dominance by the organism, demineralization did not occur. As we have seen above and in Figure 2 a variety of complex factors may be involved in determining the formation of a lesion and more data are available on some than others: 1. The time of exposure to a ‘cariogenic’ plaque may be too short, 2. Salivary flow and fluoride levels at each site might be different, 3. The composition and fluoride content of the enamel at the sites may vary, 4. The local community or individual bacterial populations may increase the plaque pH at the ‘resistant’ site, 5. Strains of mutans streptococci at the two sites may vary in virulence, 6. The plaque fluid within the biofilm at the resistant site can provide a different environment for the biofilm community and influence demineralization, 7. The sites may receive differing levels of carbohydrate, 8. The populations of mutans streptococci may be in different spatial relationships to the enamel surface, 9. Unknown chemical mediators that modify the physiology of S. mutans may be present in plaque at the ‘resistant’ site. Although there is a plethora of factors and interactions that can influence dominance by S. mutans leading to the formation of a caries lesion it is possible that at some point this organism may be released from any constraints of the community. A dominant microcolony might become independent of the other populations in the community and ‘control’ its own environment (126). This would mean that essentially in a limited area the population could be acting in a manner similar to cells in a biofilm in mono-associated gnotobiotic animals. The release of such a microcolony from any ‘community control’ may encourage lesion formation. Finally, a point worth noting is that mutans streptococci, like other oral bacteria can, in all probability, survive in the plaque biofilm in the absence of an immediately available niche (31). These cells could take advantage of any change in the environment that provided a suitable niche and then move to dominance in the community. THE INVOLVEMENT OF BACTERIA OTHER THAN MUTANS STREPTOCOCCI IN CARIES The results from several studies (see above) suggest that other bacteria can also become dominant in plaque community and be associated with demineralization and for- mation of a caries lesion. The common finding of a predominant species in lesions suggests that the process of selection, succession and dominance is independent of the species involved. Again it is assumed that such succession to dominance is based on selection in an environment of low pH. However, there is some evidence that the pH associated with root surface lesions may not necessarily be any lower than that of plaque on normal enamel (127). Also, early lesions of root caries seem to favour Actinomyces (65), which are generally less acid tolerant compared to mutans streptococci (125, 128). Consequently, although acid selection may operate, it may be less stringent in some cases and favour bacteria that while being less aciduric than mutans streptococci are still able to destroy tissue. Also, it is known that other species and strains may be as aciduric as mutans streptococci (22). We lack evidence for caries being the result of the collaborative activities of a community (communality), as we usually tend to find dominance by a particular strain. However it could be argued that communality is responsible for all caries lesions. The formation of a lesion is the end result of a temporal process involving the bacterial community and also the physiology of the host. Certainly, other organisms and interactions (i.e. communality) are invoked for reducing the cariogenicity of plaque. However, as mentioned previously, the failure of these anti-cariogenic interactions and the loss of ‘communality’, which promotes isolated activity by a specific odontopathogen could promote caries. The microbial ecology of the lesion Bacteria decalcify enamel and tooth root and may follow protein in the enamel, and invade dentine via the tubules (95). It is well accepted that the microflora of lesions in teeth and tooth roots is extremely complex and may vary at different sites (65, 125, 129). Although decalcification is a major factor involved in the initiation of enamel and root caries, degradation of dentine probably involves proteolysis (130). Also, specific receptors allow Lactobacillus to localize to exposed dentine, via collagen receptors (131) and similar molecules may be present on other bacteria. The results of Schüpbach et al. (66) are particularly significant when the possibility of succession in caries lesions is addressed. These authors found different species to be predominant in the flora of lesions of different severity, suggesting that succession could occur during lesion formation. They present a detailed and logical discussion of the microbiology of caries lesions based on their careful sampling and extensive analysis of the microflora. The populations in the lesion community may also be spatially distributed in a manner similar to those in a biofilm. Therefore, one could suggest that a range of niches and microhabitats could equally well exist within a lesion. Spatial distribution could be one explanation of the finding of the same patterns of distribution of ribotypes of The microbial ecology of dental caries A. naeslundii, in samples from enamel, root and caries lesions of individuals (80), although in one case they have been shown to have different phenotypes (79). The emphasis that has been placed on the mechanisms involved in the initiation of caries lesions in enamel is easily understood in terms of designing strategies to prevent caries. However, the microbial ecology of the stages of dentine destruction presents an equally fascinating area for study. CONCLUSIONS The microbial ecology of caries includes the biology of oral bacteria within three related habitats 1. The host population, 2. The oral cavity of individuals and 3. The caries lesion. The distribution of odontopathogens among the host population influences the colonization of infants and children. Caries in an individual is characterized by a series of interactions and succession within the plaque biofilm as the populations respond to environmental changes and succession probably also occurs in the lesion. The population interactions are complex and apart from the commonly known mutualism, competition etc. involve stress responses, adaptation, variation in gene expression, genetic variation and probably ‘quorum sensing’. All of these can result in selection of bacteria, including odontopathogens best suited to the environment, which in some cases is conducive to caries. Modulation of the microbial ecology of caries using relatively simple approaches such as oral hygiene, diet control and fluoride are very effective. Perhaps that is because they modulate the oral bacterial community so that the bacteria cannot adapt, (oral hygiene), or control a significant parameter (diet) or adaptation reduces the cariogenicity of odontopathogens (fluoride). Other approaches to modulate the flora and control caries e.g. antibacterials (132), immune mechanisms (133), replacement therapy (134) are attractive and more sophisticated in concept and delivery. However, in general these approaches are directed at mutans streptococci and although their use would make significant reductions in caries, they may not eliminate the disease. As we have seen, oral microbial ecology is complex and other, somewhat forgotten bacteria, could assume the role of mutans streptococci in caries. REFERENCES 1. Locker D, Clarke M, Payne B. Self-perceived oral health status, psychological well-being and life satisfaction in an older population. J Dent Res 2000; 79: 970–5. 2. Finlay BB, Falkow S. Common themes in microbial pathogenicity revisited. Microbiol Mol Biol Rev 1997; 61: 136 – 69. 3. Brumell JH, Steele-Mortimer O, Finlay BB. Bacterial invasion. Force feeding by Salmonella. Curr Biol 1999; 9: R277 – 80. 4. Meyer TF. Pathogenic neisseriae: complexity of pathogenhost cell interplay. Clin Inf Dis 1999; 28: 433–41. 5. Rosenberg R, ed. Microbial Ecology and Infectious Disease. Washington: American Society for Microbiology, Washington, DC, 1999. 145 6. Keene HJ, Folsom KS, Basel DA, Puente ES. Primary reservoirs of Streptococcus mutans and their relationship to caries experience in adults with good oral health. Oral Microbiol Immunol 1990; 5: 19 – 23. 7. Caufield PW, Cutter GR, Dasanayake AP. Initial acquisition of mutans streptococci by infants: evidence for a discrete window of infectivity. J Dent Res 1993; 72: 37 – 45. 8. Redmo Emanuelsson I, Wang X. Demonstration of identical strains of mutans streptococci within Chinese families by genotyping. Eur J Oral Sci 1998; 106: 788 – 94. 9. Redmo Emanuelsson I, Thorhqvist E. Genotypes of mutans streptococci tend to persist in their host for several years. Caries Res 2000; 34: 133 – 9. 10. Köhler B, Andreen I, Jonsson B. The effect of caries preventive measures in mothers on dental caries and the oral presence of the bacteria Streptococcus mutans and lactobacilli in their children. Arch Oral Biol 1984; 29: 879 – 83. 11. Köhler B, Andreen I, Jonsson B. The earlier the colonization by mutans streptococci, the higher the caries prevalence at 4 years of age. Oral Microbiol Immunol 1988; 3: 14 – 7. 12. Reichmann P, König A, Liñares J, Alcaide F, Tenover FC, McDougal L, Swidsinski S, Hakenbeck R. A global gene pool for high-level cephalosporin resistance in commensal Streptococcus species and Streptococcus pneumoniae. J Infect Dis 1997; 176: 1001 – 12. 13. Hackenback R, König A, Kern I, van der Linden M, Keck W, Billot-Klein D, Legrand R, Scoot B, Gutman L. Acquisition of five high Mr penicillin-binding protein variants of high-level b-lactam resistance from Streptococcus mitis to Streptococcus pneumoniae. J Bacteriol 1998; 180: 1831 – 40. 14. Poulsen K, Reinholdt J, Jespergaard C, Boye K, Brown TA, Hauge M, Kilian M. A comprehensive genetic study of streptococcal immunoglobulin A 1 proteases: evidence for recombination within and between species. Infect Immun 1998; 66: 181 – 90. 15. Hanley SA, Aduse-Opoku J, Curtis M. A 55-Kilodalton immunodominant antigen of Porphyromonas gingi6alis has arisen via horizontal gene transfer. Infect Immun 1999; 67: 1157 – 71. 16. Bowden GHW. Which bacteria are cariogenic in humans? In: Johnson NW, ed. Risk Markers for Oral Diseases, Vol 1 Dental Caries. Cambridge: Cambridge University Press, 1991: 266 – 86. 17. Bowden GHW, Edwardsson S. Oral ecology and dental caries. In: Thylstrup A, Fejerskov O, eds. Textbook of Clinical Cariology, 2nd Ed. Copenhagen: Munksgaard, 1996: 45 – 69. 18. Marsh PD. Microbiology of dental plaque and its significance in health and disease. Adv Dent Res 1994; 8: 263 –71. 19. Van Houte J. Role of microorganisms in caries etiology. J Dent Res 1994; 73: 672 – 81. 20. Hamilton IR. Ecological basis for dental caries. In: Ellen R, Kuramitsu H, eds. Oral Bacterial Ecology: The Molecular Basis. Wymondham: Horizon Scientific Press, 2000: 219 –74. 21. Milnes AR, Bowden GH. The microflora associated with the developing lesions of nursing caries. Caries Res 1985; 19: 289 – 97. 22. van Ruyven FOJ, Lingström P, van Houte J, Kent R. Relationship among mutans streptococci, ‘low pH’ bacteria and iodophilic polysaccharide-producing bacteria in dental plaque and early enamel caries in humans. J Dent Res 2000; 79: 778 – 84. 23. Burne RA. Oral streptococci… products of their environment. J Dent Res 1998; 77: 445 – 52. 24. Marsh PD, Bowden GHW. Microbial community interactions in biofilms. In: Lappin-Scott H, Gilbert P, Wilson M, 146 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. G. H. W. Bowden Allison D. eds, Community Structure and Co-operation in Biofilms. Society for General Microbiology Symposium series. Cambridge:Cambridge University Press, 2000: in press. Burne RA, Chen y-TM, Penders JEC. Analysis of gene expression in Streptococcus mutans biofilms in 6itro. Adv Dent Res 1997;11:100-9. Li Y-H, Chen Y-YM, Burne RA. Regulation of urease gene expression by Streptococcus sali6arius growing in biofilms. Environ Microbiol 2000; 2: 169–77. Svensäter G, Sjögreen B, Hamilton IR. Multiple stress responses in Streptococcus mutans and the induction of general and stress-specific proteins. Microbiology 2000; 146: 107 – 17. Marsh PD, Bradshaw DJ. Physiological approaches to the control of oral biofilms. Adv Dent Res 1997; 11: 176 – 85. Ofek I, Doyle RJ. Adhesion of bacteria to oral tissues. In: Bacterial Adhesion to Cells and Tissues. London: Chapman and Hall, London, 1994:195-238. Bowden GHW, Li Y-H. Nutritional influences on biofilm development. Adv Dent Res 1997; 11: 81–99. Bowden GHW, Hamilton IR. Survival of oral bacteria. Crit Rev Oral Biol Med 1998; 9: 54–85. Kolenbrander PE, Anderson RN, Clemans DL, Whittaker CJ, Klier CM. Potential role of functionally similar coaggregation mediators in bacterial succession. In: Newman HN, Wilson M, eds. Dental Plaque Revisited Oral Biofilms in Health and Disease. Cardiff: Bioline, 1999: 171–86. Van der Hoeven JS, de Jong MH, van Nieuw Amerongen A. Growth of oral microflora on saliva from different glands. Microb Ecol Hlth Dis 1989; 2: 171–80. Van der Hoeven JS, Camp PJ. Synergistic degradation of mucin by Streptococcus oralis and Streptococcus sanguis in mixed chemostat cultures. J Dent Res 1991; 70: 1041 – 4. Bradshaw DJ, Homer KA, Marsh PD, Beighton D. Metabolic cooperation in oral microbial communities during growth on mucin. Microbiology 1994; 140: 3407–12. Byers HL, Tarelli E, Homer KA, Beighton D. Isolation and characterisation of sialidase from a strain of Streptococcus oralis. J Med Microbiol 2000; 49: 235–44. van Palenstein Helderman WH, Matee MI, van der Hoeven JS, Mikx FH. Cariogenicity depends more on diet than the prevailing streptococcus species. J Dent Res 1996; 75: 535 – 45. Scannapieco FA. Saliva-bacterium interactions in oral microbial ecology. Crit Rev Oral Biol Med 1994; 5: 203 – 48. Rudney JD. Does variability in salivary protein concentrations influence oral microbial ecology and oral health? Crit Rev Oral Biol Med 1995; 6: 343–67. Marcotte H, Lavoie MC. Oral microbial ecology and the role of salivary immunoglobulin A. Microbiol Mol Biol Rev 1998; 62: 71 – 109. Tenovuo J. Antimicrobial function of human saliva-how important is it for oral health? Acta Odontol Scand 1998; 56: 250 – 6. Helmerhorst EJ, Hodgson R, van’t Hof W, Veerman ECI, Allison C, van Nieuw Amerongen A. The effects of histatinderived basic antimicrobial peptides on oral biofilms. J Dent Res 1999; 78: 1245–50. Ayad M, van Wuyckhuyse BC, Minaguchi K, Raubertas RF, Bedi GS, Billings RJ, Bowen WH, Tabak LA. The association of basic proline-rich peptides in saliva from the human parotid gland with caries experience. J Dent Res 2000; 79: 976 – 82. Dawes C, Watanabe S, Biglow-Lecomte P, Dibdin GH. Estimation of the velocity of the salivary film at some different locations in the mouth. J Dent Res 1989; 68: 1479 – 82. 45. Macpherson LMD, Dawes C. Effects of salivary film velocity on pH changes in artificial plaque containing Streptococcus oralis, after exposure to sucrose. J Dent Res 1991; 70: 1230 – 4. 46. Dawes C, Macpherson LMD. The distribution of saliva and sucrose around the mouth during use of chewing gum and the implications for the site-specificty of caries and calculus deposition. J Dent Res 1993; 72: 852 – 7. 47. Fejerskov O, Ekstrand J, Burt BA. eds. Fluoride in dentistry. Copenhagen: Munksgaard, Copenhagen 1996. 48. Bowden GHW, Ellwood DC, Hamilton IR. Microbial ecology of the oral cavity. In: Alexander M, ed. Advances in Microbial Ecology, vol 3. New York: Plenum Press, 1979: 135 – 217. 49. Theilade E. Factors controlling the microflora of the healthy mouth. In: Hill MJ, Marsh PD, eds. Human Microbial Ecology. Boca Raton: CRC Press Inc., 1990: 2 – 48. 50. Weatherell JA, Robinson C, Hallsworth AS. Variations in the chemical composition of human enamel. J Dent Res 1974; 53: 180 – 92. 51. Li J, Nakagaki H, Tsuboi S, Kato S, Huang S, Mukai M, Robinson C, Strong M. Fluoride profiles in different surfaces of human permanent molar enamels from a naturally fluoridated and a non-fluoridated area. Archs Oral Biol 1994; 39: 727 – 31. 52. Tucker K, Adams M, Shaw L, Smith AJ. Human enamel as a substrate for in 6itro acid dissolution studies: influence of tooth surface and morphology. Caries Res 1998; 32: 135 –40. 53. Loesche WJ. Role of Streptococcus mutans in human dental decay. Microbiol Rev 1986; 50: 353 – 80. 54. Lang KP, Hotz PR, Gusberti F, Joss A. Longitudinal, clinical and microbiological study on the relationship between infection with Streptococcus mutans and the development of caries in humans. Oral Microbiol Immunol 1987; 2: 39 – 47. 55. Radford JR, Ballantyne HM, Nugent Z, Beighton D, Robertson M, Longbottom C, Pitts NB. Caries-associated micro-organisms in infants from different socio-economic backgrounds in Scotland. J Dent 2000; 28: 307 – 12. 56. Sigurjóns H, Magnúsdóttir MO, Holbrook WP. Cariogenic bacteria in a longitudinal study of approximal caries. Caries Res 1995; 29: 42 – 5. 57. Boyar RM, Thylstrup A, Holmen L, Bowden GHW. The microflora associated with the development of initial enamel decalcification below orthodontic bands in 6i6o in children living in a water-fluoridated area. J Dent Res 1989; 68: 1734 – 8. 58. Nyvad B, Kilian M. Microflora associated with experimental root surface caries in humans. Infect Immun 1990; 58: 1628 – 33. 59. Marsh PD, Featherstone A, McKee AS, Hallsworth AS, Robinson C, Weatherell JA, Newman HN, Pitter AFV. A microbiologcal study of early caries of approximal surfaces in schoolchildren. J Dent Res 1989; 68: 1151 – 4. 60. Batty I. Actinomyces odontolyticus, a new species of actinomycete regularly isolated from deep carious dentine. J Pathol Bacteriol 1958; 75: 455 – 9. 61. Sarkonen N, Könönen E, Summanen P, Kanervo A, Takala A, Jousimies-Somer H. Oral colonization with Actinomyces species by two years of age. J Dent Res 2000; 79: 864 –7. 62. Boyar R, Bowden GHW. The microflora associated with the progression of incipient caries lesions in teeth of children living in a water-fluoridated area. Caries Res 1985; 19: 298 – 306. 63. Bowden GH, Ekstrand J, McNaughton B, Challacombe SJ. The association of selected bacteria with the lesions of root surface caries. Oral Microbiol Immunol 1990; 5: 346 – 51. The microbial ecology of dental caries 64. Bowden GHW. Microbiology of root surface caries in humans. J Dent Res 1990; 96: 1205–10. 65. Schüpbach P, Osterwalder V, Guggenheim B. Human root caries:microbiota in plaque covering sound, carious and arrested carious root caries. Caries Res 1995; 29: 382 – 95. 66. Schüpbach P, Osterwalder V, Guggenheim B. Human root caries: microbiota of a limited number of root caries lesions. Caries Res 1996; 30: 52–64. 67. Brailsford SR, Lynch E, Beighton D. The isolation of Actinomyces naeslundii from sound root surfaces and root carious lesions. Caries Res 1998; 32: 100–6. 68. Sansone C, Van Houte J, Joshipura K, Kent R, Margolis HC. The association of mutans streptococci and non-mutans streptococci capable of acidogenesis at low pH with dental caries on enamel and root caries. J Dent Res 1993; 72: 508 – 16. 69. Mikx FMH, van der Hoeven JS, König KG, Plasschaert AJM, Guggenheim B. Establishment of defined microbial ecosystems in germ-free rats. Caries Res 1972; 6: 211 – 23. 70. Mikx FHM, van der Hoeven JS, Walker GJ. Microbial symbiosis in dental plaque studied in gnotobiotic rats and in the chemostat. In: Stiles HM, Loesche WJ, O’Brien TC, eds. Microbial Aspects of Dental Caries. Sp.Supplement Microbiology Abstracts Vol III. Washington: Information retrieval Inc., Washington 1976:763–71. 71. van der Hoeven JS, Toorop AI, Mikx FHM. Symbiotic relationship of Veillonella alcalescens and Streptococcus mutans in dental plaque in gnotobiotic rats. Caries Res 1978; 12: 142 – 7. 72. Marquis RE. Oxygen metabolism, oxidative stress and acidbase physiology of dental plaque biofilms. J Ind Microbiol 1995; 15: 198 – 207. 73. Sissons CH, Hancock EM. Urease activity in Streptococcus sali6arius at low pH. Archs Oral Biol 1993; 38: 507– 16. 74. Morou-Bermudez E, Burne RA. Genetic and physiologic characterization of urease of Actinomyces naeslundii. Infect Immun 1999; 67: 504–12. 75. Clancy KA, Pearson S, Bowen WH, Burne RA. Characterization of recombinant, ureolytic Streptococcus mutans demonstrates an inverse relationship between dental plaque ureolytic capacity and cariogenicity. Infect Immun 2000; 68: 2621 – 9. 76. Sissons CH, Wong L, Shu M. Factors affecting the resting pH of in 6itro human microcosm dental plaque and Streptococcus mutans biofilms. Archs Oral Biol 1998; 43: 93 – 102. 77. Imfeld I, Birkhed D, Lingström P. Effect of urea in sugarfree chewing gums on pH recovery in human dental plaque evaluated with three different methods. Caries Res 1995; 29: 172 – 80. 78. Peterson S, Woodhead J, Crall J. Caries resistance in children with chronic renal failure; plaque pH, salivary pH and salivary composition. Pediatr Res 1985; 19: 796–9. 79. Bowden GHW. Oral biofilm an archive of past events? In: Newman HN, Wilson M, eds. Dental Plaque Revisited Oral Biofilms in Health and Disease. Cardiff: Bioline, 1999: 211 – 35. 80. Bowden GHW, Nolette N, Ryding H, Cleghorn BM. The diversity and distribution of the predominant ribotypes of Actinomyces naeslundii genospecies 1 and 2 in samples from enamel and from healthy and carious root surfaces of teeth. J Dent Res 1999; 78: 1800–9. 81. Arber W. Genetic variation: molecular mechanisms and impact on microbial evolution. FEMS Microbiol Rev 2000; 26: 1 – 7. 82. Westegren G, Krasse B, Birkhed D, Edwardsson S. Genetic transfer of markers for sorbitol (D-glucitol) metabolism in oral streptococci. Arch Oral Biol 1981; 26: 403–7. 147 83. Colby SM, Harrington DJ, Russell RRB. Identification and genetic characterisation of melibiose-negative isolates of Streptococcus mutans. Caries Res 1995; 29: 407 – 12. 84. Haubek D, Dirienzo JM, Tinoco EM, Westergaard J, López NJ, Chung C-P, et al. Racial tropism of a highly toxic clone of Actinobacillus actinomycetemcomitans associated with juvenile periodontitis. J Clin Microbiol 1997; 35: 3037 – 42. 85. Acton RT, Dasanayake AP, Harrison RA, Li Y, Roseman JM, Go RC, Wiener H, Caufield PW. Associations of MHC genes with levels of caries-inducing organisms and caries severity in African-American women. Hum Immunol 1999; 60: 984 – 9. 86. Rainey PB, Moxon ER, Thompson IP. Intraclonal polymorphism in bacteria. In: Gwynfryn Jones J, ed. Advances in Microbial Ecology, Vol 13. New York: Plenum Press, 1993: 263 – 300. 87. Trahan L. Xylitol: a review of its action on mutans streptococci and dental plaque-its clinical significance. Int Dent J 1995; 45: 77 – 92. 88. Bearson S, Bearson B, Foster JW. Acid stress responses in enterobacteria. FEMS Microbiol Lett 1997; 147: 173 – 80. 89. Hecker M, Volker U. Non-specific, general and multiple stress resistance of growth-restricted Bacillus subtilis cells by the expression of the sigma B regulon. Mol Microbiol 1998; 29: 1129 – 36. 90. Segal G, Ron EZ. Regulation of heat shock response in bacteria. Ann N Y Acad Sci 1998; 851: 147 – 51. 91. Hamilton IR, Svensäter G. Acid-regulated proteins induced by Streptococcus mutans and other oral bacteria during acid shock. Oral Microbiol Immunol 1998; 13: 292 – 300. 92. Dunny GM, Winans SC. eds, Cell-cell Signaling in Bacteria. Washington:American Society for Microbiology Press, Washington, DC, 1999. 93. Liljemark WF, Bloomquist CG, Reilly BE, Bernards CJ, Townsend DW, Pennock AT, LeMoine JL. Growth dynamics in a natural biofilm and its impact on oral disease management. Adv Dent Res 1997; 11: 14 – 23. 94. Caldwell DE, Atuku E, Wilkie DC, Wivcharuk KP, Karthikeyan S, Korber DR, Schmid DF, Wolfaardt GM. Germ theory vs community theory in understanding and controlling the proliferation of biofilms. Adv Dent Res 1997; 11: 4 – 13. 95. Thylstrup A, Fejerskov O. Clinical and pathological features of dental caries. In: Thylstrup A, Fejerskov O, eds. Textbook of Clinical Cariology, 2nd. Ed. Copenhagen: Munksgaard, Copenhagen. 1996: 111 – 48. 96. Ingram GS, Silverstone LM. A chemical and histological study of artificial caries in human dental enamel in 6itro. Caries Res 1981; 15: 393 – 8. 97. Bowden GH, Spiers RL, Nash R. Modification of the release of calcium and phosphate from enamel by deposits of dextran-producing streptococci. Caries Res 1972; 6: 81 – 2. 98. Rose RK, Turner SJ, Dibdin GH. Effect of pH and calcium concentration on calcium diffusion in streptococcal model plaque biofilms. Archs Oral Biol 1997; 42: 795 – 800. 99. Assinder SJ, Dibdin GH, Marshall M, Shellis P. An in vitro system for the analysis of changes in depth distribution of diffusates in bacterial films. Caries Res 1998; 32: 255 – 61. 100. Guggenheim B, Schroeder HE. Biochemical and morphological aspects of extracellular polysaccharides produced by cariogenic streptococci. Helv Odont Acta 1967; 11: 131 –51. 101. Cury JA, Rebello MAB, Del Bel Cury AA. In situ relationship between sucrose exposure and the composition of dental plaque. Caries Res 1997; 31: 356 – 60. 102. Zero DT, van Houte J, Russo J. The intra-oral effect on enamel demineralization of extracellular matrix material syn- 148 103. 104. 105. 106. 107. 108. 109. 110. 111. 112. 113. 114. 115. 116. 117. G. H. W. Bowden thesized from sucrose by Streptococcus mutans. J Dent Res 1986; 65: 918 – 23. Dibdin GH, Shellis RP. Physical and biochemical studies of Streptococcus mutans sediments suggest a new factor linking cariogenicity of plaque with its extracellular polysaccharide content. J Dent Res 1988; 67: 890–5. Van Houte J, Russo J, Prostak KS. Increased pH-lowering ability of Streptococcus mutans cell masses associated with extracellular glucan-rich matrix material and the mechanisms involved. J Dent Res 1989; 68: 451–9. Margolis HC, Moreno EC. Composition and cariogenic potential of dental plaque fluid. Crit Rev Oral Biol Med 1994; 5: 1 – 25. Carey CM, Chow LC, Tatevossian A, Vogel GL. Extracellular potassium concentrations in human dental plaque fluid recovered from single sites. Archs Oral Biol 1988a; 33: 493 – 8. Carey CM, Gregory TM, Tatevossian A, Vogel GL. The buffer capacity of single-site resting, human dental-plaque fluid. Archs Oral Biol 1988b; 33: 487–92. Vogel GL, Carey CM, Chow LC, Tatevossian A. Microanalysis of plaque fluid from single-site fasted plaque. J Dent Res 1990; 69: 1316–23. Keevil CW, West AA, Bourne N, Marsh PD. Inhibition of the synthesis and secretion of extracellular glucosyl- and fructosyltransferase in Streptococcus sanguis by sodium ions. J Gen Microbiol 1984; 130: 77–82. Wang YB, Germaine GR. Effects of pH, potassium, magnesium, and bacterial growth phase on lysozyme inhibition of glucose fermentation by Streptococcus mutans 10449. J Dent Res 1993; 72: 907–11. Iwami Y, Guha-Chowhury N, Yamada T. Effect of sodium and potassium ions on intracellular pH and proton excretion in glycolyzing cells of Streptococcus mutans NCTC 10449 under strictly anaerobic conditions. Oral Microbiol Immunol 1997; 12: 77 – 81. Russell JB, Diez-Gonzalez F. The effects of fermentation acids on bacterial growth. Adv Micro Physiol 1998; 39: 205 – 34. Barnard JP, Stinson MW. Influence of environmental conditions on hydrogen peroxide formation by Streptococcus gordonii. Infect Immun 1999; 67: 6558–64. Wood SR, Kirkham J, Marsh PD, Shore RC, Nattress B, Robinson C. Architecture of intact natural human plaque biofilms studied by confocal laser scanning microscopy. J Dent Res 2000; 79: 21–7. Mattila ML, Rautava P, Silanpää M, Paunio P. Caries in five-year-old children and associations with family-related factors. J Dent Res 2000; 79: 875–81. Radford JR, Ballantyne HM, Nugent Z, Beighton D, Robertson M, Longbottom C, Pitts NB. Caries-associated microorganisms in infants from different socio-economic backgrounds in Scotland. J Dent 2000; 28: 307–12. Gronroos L, Saarela M, Matto J, Tanner-Salo U, Vuorela A, Alaluusua S. Mutacin production by Streptococcus mutans may promote transmission of bacteria from mother to child. Infect immun 1998; 66: 2595–600. . 118. Li Y, Wang W, Caufield PW. The fidelity of mutans streptococci transmission and caries status correlate with breastfeeding experience among Chinese families. Caries Res 2000; 34: 123 – 32. 119. Köhler B, Krasse B. Human strains of mutans streptococci show different cariogenic potential in the hamster model. Oral Microbiol Immunol 1990; 5: 177 – 80. 120. Krull RE, Chen P, Novak J, Kirk M, Barnes S, Baker J, Krishna NR, Caufield PW. Biochemical structural analysis of the lantibiotic mutacin II. J Biol Chem 2000; 275: 15845– 50. 121. Crowley PJ, Fischlschweiger W, Coleman SE, Bleiweis AS. Intergeneric bacterial coaggregations involving mutans streptoccci and oral actinomyces. Infect Immun 1987; 55: 2695– 700. 122. McBride BC, van der Hoeven JS. Role of bacterial adherence in colonization of the oral cavities of gnotobiotic rats infected with Streptococcus mutans and Veillonella alcalescens. Infect Immun 1981; 33: 467 – 72. 123. Johansson I, Birkhed D. Diet and the caries process. In: Thylstrup A, Fejerskov O, eds. Textbook of Clinical Cariology, 2nd Ed. Copenhagen: Munksgaard, 1996: 283 – 99. 124. Lingström P, van Ruyven FOJ, van Houte J, Kent R. The pH of dental plaque in its relation to early enamel caries and dental plaque flora in humans. J Dent Res 2000; 79: 770–7. 125. Bradshaw DJ, Marsh PD. Analysis of pH-driven disruption of oral microbial communities in 6itro. Caries Res 1998; 32: 456 – 62. 126. Shapiro JA, Dworkin M. eds. Bacteria as Multicellular Organisms. New York: Oxford University Press, New York, 1997. 127. Scheie A, Luan W-M, Dahlén G, Fejerskov O. Plaque pH and microflora of dental plaque on sound and carious root surfaces. J Dent Res 1996; 75: 1901 – 8. 128. Svensäter G, Larsson U-B, Grief ECG, Cvitkovitch DG, Hamilton IR. Acid tolerance response and survival by oral bacteria. Oral Microbiol Immunol 1997; 12: 266 – 73. 129. Edwardsson S. Bacteriological studies on deep areas of carious dentine. Odont Revy 1974; 25 (Suppl.32): 1 – 143. 130. Tjäderhane L, Larjava H, Sorsa T, Uitto V-J, Larmas M, Salo T. The activation and function of host matrix metalloproteinases in dentine matrix breakdown in caries lesions. J Dent Res 1998; 77: 1622 – 9. 131. McGrady JA, Butcher WG, Beighton D, Switalski LM. Specific and charge interactions mediate collagen recognition by oral lactobacilli. J Dent Res 1995; 74: 649 – 57. 132. Scheie A. Chemoprophylaxis of dental caries. In: Thylstrup A, Fejerskov O, eds. Textbook of Clinical Cariology, 2nd. Ed. Copenhagen: Munksgaard, 1996: 311 – 24. 133. Hajishengallis G, Michalek SM. Current status of a mucosal vaccine against dental caries. Oral Microbiol Immunol 1999; 14: 1 – 20. 134. Hillman JD, Brooks TA, Michalek SM, Harmon CC, Snoep JL, Der Weijden CC. Construction and characterization of an effector strain of Streptococcus mutans for replacement therapy of dental caries. Infect Immun 2000; 68: 543 – 9.