Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Drug interaction wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Pharmacognosy wikipedia , lookup
Prescription costs wikipedia , lookup
Neuropharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
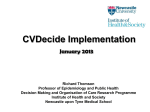
Pleiotropic Effects of Statins Review Article Acta Cardiol Sin 2005;21:190-8 Pleiotropic Effects of Statins Daniel Pella, Rafael Rybar and Viola Mechirova In the last decades, substantial progress has been made in understanding the relationship between lipid disorders and the prevention of cardiac ischemic disease. The identification of new therapeutic targets and new lipid-modifying agents expands treatment options. Statins have been described as the principal and most effective class of drugs to reduce serum cholesterol levels and cardiovascular events in patients with or without coronary artery disease. Since the discovery of the first statin nearly 30 years ago, this class of drugs has advanced to become the mainstay of cholesterol-lowering therapy. It was found during recent years that many of statins, positive effects could not be explained simply by lowering of atherogenic lipids. There were shown also to exist non-lipid-modifiable effects of statins called pleiotropic ones, which could be responsible for this additional benefit. The most important positive pleiotropic effects of statins are antiinflammatory, antiproliferative, and antithrombotic ones, improving endothelial dysfunction and others. Key Words: Statins · Pleiotropic effects · Atherosclerosis INTRODUCTION able to inhibit activity of one of the enzymes in the cascade of cholesterol synthesis, 3-hydroxy-3 methylglutaryl coenzyme A reductase (HMG CoA reductase).3 This substance was used for further name statins (vastatins). Two decades of research after discovery were sufficient for conclusion that statins were considered a very important group of drugs (professor Roberts stated that statins were for atherosclerosis the same as was penicillin for infectious diseases).4 Statins have become one of the basic pillars in the secondary and primary prevention of atherosclerosis.5-9 Their role is documented in preventing progression of atherosclerosis, and they are even able to cause regression of the disease. Decrease of cardiovascular endpoints, but also total mortality found in clinical studies could not be explained only by the decrease of atherogenic lipids – it was greater than benefit from lipid lowering. Speculation about so called pleiotropic effects (non-lipid-modifiable) appeared and was confirmed by further research activity. Cardiovascular disease, which includes coronary heart disease, stroke, and peripheral arterial disease, is the leading cause of death worldwide. In 2001, cardiovascular diseases contributed to nearly one third of all global deaths.1 According to World Health Organization statistics, more than 16 million people die of cardiovascular disease each year, and 7.2 million deaths in 2001 were caused by heart disease. 2 By the year 2020, approximately 25 million deaths annually worlwide are expected from cardiovascular disease, and almost half of those deaths (11.1 million) will be from coronary heart disease.2 Statins were discovered in 1976 when Endo et al. found that a product of mould Penicillium citricum was Received: December 29, 2004 Accepted: July 7, 2005 1st Internal Clinic, Faculty of Medicine PJ Safarik University Kosice, Slovakia Address correspondence and reprint requests to: Prof. Daniel Pella, MD, PhD, 1st Internal Clinic, Faculty of Medicine PJ Safarik University, Trieda SNP 1, 040 66 Kosice, Slovakia. Tel: 421 55 640 3409; Fax: 421 51 7725 118; E-mail: [email protected] Acta Cardiol Sin 2005;21:190-8 CHARACTERISTICS OF STATINS Statins are a chemically and pharmacologically di190 Pleiotropic Effects of Statins questions about additional beneficial effects of statins, because mevalonate, the product of the enzyme reaction, is the precursor not only of cholesterol but also of many nonsteroidal isoprenoid compounds, and inhibition of HMG-CoA reductase may produce pleiotropic effects (see Figure 1). Indeed, the mevalonate pathway yields a series of isoprenoids that are vital for diverse cellular functions.11 These isoprenoids include: isopentanyl adenosine, present in some types of transfer RNA; dolichols, required for glycoprotein synthesis; and polyisoprenoid side chains of ubiquinone and heme A, involved in electron transport. Several proteins have also been identified that are post-translationally modified by the covalent attachment of mevalonate-derived isoprenoid groups-either farnesyl or geranylgeranyl pyrophosphate. These proteins must be prenylated as a prerequisite for membrane association, which is required for their function. Members of this family are involved in a number of cellular processes, including cell signaling, cell differentiation and proliferation, myelination, cytoskeleton dynamics, verse group of drugs that share the ability to inhibit hydroxymethylglutaryl coenzyme A reductase (HMGCoA reductase), the enzyme that controls the ratelimiting step of cholesterol synthesis, but this inhibition is followed by other subsequences associated with the mevalonate pathway (Figure 1). The clinically beneficial effects of statins were usually assumed to result from their ability to reduce cholesterol synthesis. In 1994, the landmark Scandinavian Simvastatin Survival Study (4S) established the benefits of a HMG-CoA reductase inhibitor on mortality in patients with atherosclerosis.5 In accord with traditional acceptance of atherosclerosis as a consequence of lipid disorders, post-hoc analysis of the 4S trial suggested that the benefit provided by simvastatin in individual patients indeed related to the magnitude of change in low-density lipoprotein cholesterol.10 Subsequent studies, however, differed with this conclusion even as they affirmed the clinical benefits of statins as a class on cardiovascular morbidity and mortality in patients with or without established atherosclerotic disease.6-9 These studies raised Acetyl CoA HMG-CoA HMG CoA reductase mevalonate isopentanyl – PP* geranyl-PP ® dekaprenyl-PP ® dekaprenyl 4OH benzoate ® CoQ10 squalene ¬ ¾ farnesyl-PP ¾ ® farnesylated proteins cholesterol geranylated proteins activation NFkB** ® inflammation proliferation of SMC*** *PP – pyrophosphate **NFkB – nuclear factor kappa B ***SMC – smooth muscle cells Figure 1. Cholesterol (mevalonate) synthesis pathway. 191 Acta Cardiol Sin 2005;21:190-8 Daniel Pella et al. terol particles, and secondly, they have protective effect on myocyte membrane in ubiquinone deficiency which may appear during long-term statin therapy.16,18 The main action of statins is to specifically and reversibly inhibit HMG-CoA reductase, which controls the rate-limiting step in cholesterol synthesis. Several studies have compared lipid-lowering effects of different statins head to head. In one of the latest, STELLAR study, rosuvastatin in the dosage of 40 mg was more effective than all currently available statins in all recommended doses. LDL cholesterol was lowered by 55% with rosuvastatin 40 mg daily.19 These differences in efficacy were confirmed in a meta-analysis of 164 studies published in 2003. Here also, the different statins showed a two- to three-fold difference in the extent of LDL cholesterol lowering across the dosage range.20 The effect on HDL cholesterol was compared as well in the STELLAR study. It was shown that rosuvastatin had the greatest potency to increase HDL cholesterol, followed by simvastatin and atorvastatin (maximal increase 9.6% vs 6.8% vs 5.7%).21 The recent study of Bevilacqua showed different results.22 Compared were fluvastatin extended release form 80 mg daily, which was superior to atorvastatin 20 mg daily. However, in general, statins have much lower potency to increase HDL in comparison with fibrates or nicotinic acid. Surprisingly, it was shown in the MIRACL trial that high-density lipoprotein, but not low-density lipoprotein cholesterol levels, influenced short-term prognosis after acute coronary syndrome, and this finding suggested that the clinical benefit of atorvastatin after acute coronary syndrome was mediated by qualitative changes in the and endocytotic/exocytotic transport. Hence, through the inhibition of HMG-CoA reductase, statins may affect a variety of processes; this may help to explain their non-lipid-related pharmacologic properties. Indeed, several recent in vitro and in vivo experiments have demonstrated that HMG-CoA reductase inhibitors have antiatherosclerotic effects that are not related to lipid lowering. Because of their broad effects and their extremely low incidence of side effects, statins might even be seen as the new aspirin.12 The currently available statins are lovastatin, simvastatin, pravastatin, atorvastatin, fluvastatin and rosuvastatin. Cerivastatin was withdrawn from the market in 2001 due to increased number of fatal rhabdomyolyses.13 It seems that the process of metabolization of statins is important from the safety point of view. Several of them are metabolized via cytochrome P450 (see Table 1).14-16 However, only a small proportion of rosuvastatin and fluvastatin are metabolized via cytochrome P450 2C9, so there is no high risk of dangerous drug interactions associated with the use of these statins as well. Patients taking several drugs metabolized by the same cytochrome P450 are at higher risk of side effects of statins. Only two of the currently available statins are hydrophilic – pravastatin and rosuvastatin – this could also be important in prevention of “increased fluidity” of muscle cell membrane and then increased risk of myopathy or even rhabdomyolysis.16 Antioxidant activities of statins differ (the greatest is observed in atorvastatin, with surprisingly much lower activity observed in rosuvastatin) and might be cardioprotective in two different ways. Firstly, statins decrease oxidation of LDL cholesTable 1. Characteristics of statins Dose range (mg/dL) Maximal LDL-C reduction (%) Serum triglyceride reduction (%) Serum HDL-C increased (%) Penetration to CNS Renal excretion (%) Mechanism of hepatic metabolism Hydro/lipophilic properties Acta Cardiol Sin 2005;21:190-8 Atorvastatin Lovastatin Pravastatin Simvastatin 10-80 60 29 6 No 2 Cytochrome p-450 3A4 10-80 40 16 8.6 Yes 10 Cytochrome p-450 3A4 10-80 34 24 12 No 20 Sulfation 10-80 47 18 12 Yes 13 Cytochrome p-450 3A4 lipophilic lipophilic hydrophilic lipophilic 192 Fluvastatin Rosuvastatin 20-80 5-40 24 55 10 43 8 9,2 No No <6 10 Cytochrome Cytochrome p-450 2C9 p-450 2C9 (small proportion) (small proportion) lipophilic hydrophilic Pleiotropic Effects of Statins LDL particle and/or by non-lipid (pleiotropic) effects of the drug.23 upon endotheliumm, as was shown in study of Marchesi et al. with atorvastatin and other statins.29,30 Statins and Antiinflammatory Effects Recent research has shown that inflammation plays a key role in coronary artery disease and other manifestations of atherosclerosis. Immune cells dominate early atherosclerotic lesions, and activation of inflammation can elicit acute coronary syndromes. Elevated markers for inflammation such as CRP, interleukin-6, intercellular adhesion molecule-1 (ICAM-1), and serum amyloid A have been associated with increased risk for the first and reccurent cardiovascular events.31 Many experimental and clinical studies confirmed significant reduction of CRP measured by high sensitive method (hs CRP). The higher the baseline value of CRP, the higher the decrease that has been observed, e.g. in the PROVE IT study.32 In that study, decrease of hs CRP achieved 89% in the atorvastatin group and 85% in the pravastatin group. Generally, the greatest decreases of hs CRP were observed after treatment with atorvastatin or rosuvastatin. Increased levels of CRP were associated with more pronounced monocyte migration and increased LDL uptake by macrophages.33 PLEIOTROPIC EFFECTS – DEFINITION Drugs usually have multiple effects; through an analogy with single genes which affect more than one system or determine more than one phenotype, they are currently referred to as “pleiotropic effects” (from the Greek “pleion,” meaning more, and “tropos,” meaning direction or turn). These may be related or unrelated to primary mode of action of the drug. Pleiotropic effects may emerge during preclinical and clinical studies in drug development, but more often than not, they are discovered a posteriori long after the therapeutic agent is marketed (the same situation occurs in use of statins). They may be undesirable and recognized as adverse side effects, they may be neutral, or they may be beneficial, enhancing the desirable effect of a drug.24 ANTIATHEROGENIC PLEIOTROPIC EFFECTS OF STATINS Statins and Plaque Growth Statins have antiproliferative effects and inhibit transformation of contractile smooth muscle cells to reparatory-type cells and their migration from arterial media into intima. 34 Statins decrease synthesis of extracellular matrix and proteins Rac1, Rho A as well, and by this means decrease plaque growth.35 Substantial differences have been found between the statins. For example, in the ASAP study, it was shown that at the highest therapeutic dose, two years of treatment with atorvastatin reduced the thickness of the arterial wall, while after simvastatin treatment, the thickness of the arterial wall continued to increase.36 Similar results were achieved in the ARBITER study when atorvastatin and pravastatin were compared.37 In a very recent study, REVERSAL, where intravascular ultrasound method was used to quantify atherosclerosis, after 18 months of therapy with atorvastatin 80 mg daily, volume of the atherosclerotic plaque slightly decreased, while the volume of the plaque continued to increase during therapy with pravastatin 40 mg daily.38 The most important pleiotropic antiatherogenic effects of statins are improvement of endothelial dysfunction, antioxidative properties, antiinflammatory, antiproliferative and antithrombotic effects and neoangiogenesis.25 Statins inhibit by blocking HMG-CoA reductase, and also by blocking synthesis of geranylated proteins responsible for proliferation and migration of smooth muscle cells from vessel media to intima and their conversion from contractile to reparatory type which are causes growth of atherosclerotic plaque. Also, synthesis of farnesylated proteins is inhibited, that is why also activity of nuclear factor kappa B is decreased. This factor plays very important role in the initiation of inflammatory process-atherosclerosis is inflammatory disease.26 Statins and Endothelial Dysfunction Abnormal endothelium-dependent vasomotor responses predict the long-term progression of atherosclerosis and associated coronary events, as well as events after vascular surgery.27,38 Statins are able to increase nitric oxide synthesis and improve blood flow dependent 193 Acta Cardiol Sin 2005;21:190-8 Daniel Pella et al. Statins and Angiogenesis Statins are able to activate proteinkinase Akt in endothelial cells and thereby stimulate activity of endothelial nitric oxide synthethase leading to increased NO production and neoangiogenesis. Stimulation of proteinkinase Akt improves myocardial aerobic metabolism. Statins increase also the level of angiopoetine.39 Given the fact that statins will be prescribed more widely (“... statins to every patient with documented coronary artery disease...” Yusuf S, Lancet 2002), it is very important to consider the safety of such therapy.45 Statin therapy is long-term (even life-long, following evidence-based medicine), so the risk of adverse effects might be increased. More clinical studies are needed in order to confirm the beneficial effects of coenzyme Q10 substitution in long-term statin therapy. The International College of Cardiology, in its scientific statement, recommended use of statins preferably in conjunction with coenzyme Q10 in order to prevent possible myopathy.46 The recently published hypothesis by Moosmann and Behl has identified a possible role of deficiency of selenium and association with possible adverse effects of statins, namely myopathy and polyneuropathy.47 They noted that the pattern of side effects associated with statins resembled the pathology of selenium deficiency, and postulated that the mechanism lay in a wellestablished but often overlooked biochemical pathway – the isopentylation of selenocysteine-tRNA. A negative effect of statins on selenoprotein synthesis does seem to explain many of the enigmatic effects and side effects of statins, in particular, statin-induced myopathy. In a recent study, Silver et al. evaluated left ventricular diastolic function with Doppler echocardiography before and after statin therapy. Statin therapy worsened diastolic parameters in most patients; coenzyme Q10 supplementation in patients with worsened diastolic function with statin therapy improved parameters of diastolic function.48 Similar results were confirmed in the study of Kumar et al. in more than 100 studied subjects (the study of Silver et al. evaluated only 14 patients).49 What is very important to say is that statins are generally very well tolerated drugs and a remarkably safe class of lipid lowering agents. These data probably lead to the fact that in the United Kingdom simvastatin is now available in pharmacies without medical prescription.50 Statins and Plaque Rupture Statins significantly reduce metalloproteinases activity, mainly of MMP1 and MMP3, which play important roles in plaque rupture or fissuration. 40 Decrease of blood pressure observed during long-term treatment with statins lead to improvement of rheology and arterial stiffness.41 Statins and Thrombosis Statins have capacity to decrease global fibrinolytic activity of the blood, decrease activity of PAI-1 and inhibit thrombine generation. Data regarding influence of statins on fibrinogen levels are not so convincing.42 Statins and Plaque Stability There were several pleiotropic effects of statins described which should be responsible for the stability of the atherosclerotic plaque. Nevertheless, the most important finding for plaque stability is the combination of lipid-lowering effects with pleiotropic ones (especially decrease of plaque lipid core size and inhibition of inflammatory reaction).43 Possible Negative Pleiotropic Effects of Statins Inhibition of HMG-CoA reductase leads not only to decreased synthesis of cholesterol but also affects synthesis of other substances. Besides these positive pleiotropic effects, there is probably also a negative one, namely, inhibition of geranyl pyrophosphate synthesis and subsequently dekaprenyl-4-bensoate, which is a precursor of coenzyme Q10. Coenzyme Q10 (ubiquinone, ubidekarenone) is a very important substance in myocardial energetic metabolism and the stability of cell membrane as well; when deficient, myocytes could be prone to damage in the form of myopathy or myositis, or even rhabdomyolysis. 44 Deficiency of coenzyme Q10 will appear usually after longer duration of treatment and may also be dependent on type of statin and its dosage. Acta Cardiol Sin 2005;21:190-8 PLEIOTROPIC EFFECTS OF STATINS IN NON-ATHEROSCLEROTIC DISEASE Antiproliferative and antiinflammatory effects of 194 Pleiotropic Effects of Statins Table 2. Possible beneficial pleiotropic effects of statins in non-atherosclerotic diseases fibrosclerotic aortic stenosis arterial hypertension Alzheimer’s dementia rheumatic diseases (rheumatoid arthritis) sclerosis multiplex sudden cardiac death prevention deep venous thrombosis regression of left ventricular hypertrophy osteoporosis vitiligo Further study of pleiotropic functions of statins may provide insights into the biology of atherosclerosis (and other diseases e.g. osteoporosis, rheumatoid arthritis, connective tissue diseases, etc.) that could yield benefits in terms of targeting and developing novel strategies that will address the residual burden of atherosclerotic complications that plague even those individuals who achieved current lipid goals. statins have raised questions about possible use of statins in diseases other than atherosclerosis, cardiovascular and non-cardiovascular. Many clinical studies are in progress which probably should enlighten us on their relative clinical relevance and importance. Some of the diseases involved in this research are listed in Table 2.51 CONCLUSIONS REFERENCES Statins have the same mode of action via inhibition of HMG-CoA reductase activity but differ between each other in the extent of this inhibition, which leads to different levels of LDL cholesterol lowering. Due to this fact, not only cholesterol synthesis inhibited is but also formation of inflammatory proteins, substances associated with smooth muscle cells proliferation and endogenous synthesis of coenzyme Q10. Although the possibility that statins might have pleiotropic effects was met at first with healthy scepticism, the vast amount of knowledge accrued over the past few years has moved these effects into the spotlight. Pleiotropic effects of statins are numerous and varied, they may add to the desirable effect of a drug or be undesirable and interfere with the treatment. As the list of pleiotropic effects effects of statins is expanding rapidly, it will become essential to establish their relative biological significance and clinical relevance. LDL cholesterol indubitably represents a modifiable key risk factor for atherosclerosis, and lowering LDL-C blood levels certainly diminishes cardiovascular risk in the long term. The current flurry of interest in the socalled pleiotropic effects of statins should in no way deter practitioners from aggressive management of dyslipidemia, a long established risk factor, as mandated by current guidelines. Nevertheless, it will be important to take action on the new indications which have emerged from consideration of possible pleiotropic effects. 1. World Health Organization. The World Health Report 2002: Reducing risks, promoting healthy life. Geneva: World Health Organization; 2002. 2. American Heart Association. Statistical fact sheet — populations. International Disease Statistics. Dallas, T: American Heart Association; 2003. 3. Endo A, Kuroda M, Tanarawa K. Competitive inhibition of 3-HMG-CoA reductase by ML 236 A and ML 236 B. Febs Lett 1976;72:323-6. 4. Roberts JR. Lipid-lowering drugs in atherosclerosis. Am J Cardiol 1996;89:682. 5. Simvastatin Survival Study Group. Randomized trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;334:1383-9. 6. Sacks FM, Pfeffer MA, Moye LA. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. N Eng J Med 1996;335:1001-9. 7. The Long-term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and broad range of initial cholesterol levels. N Eng J Med 1998;339:1349-57. 8. West of Scotland Coronary Prevention Group. West of Scotland Coronary Prevention Study: identification of High-risk Groups and Comparison with Other Cardiovascular Intervention Trials. Lancet 1996;346:1339-42. 9. Downs JR, Clearfield M, Weis S. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels. N Eng J Med 1999;339:1615-22. 195 Acta Cardiol Sin 2005;21:190-8 Daniel Pella et al. 10. Pedersen TR, Olsson AG, Faergeman O, et al. For the Simvastatin Survival Study Group. Lipoprotein changes and reduction in the incidence of major coronary heart disease events in the Scandinavian Simvastatin Survival Study (4S). Circulation 1998;97:1453-60. 11. Corsini A, Bellosta S, Baetta R, et al. New insights into the pharmacodynamic and pharmacokinetic properties of statins. Pharmacol Ther 1999;84:413-28. 12. Veillard NR, Mach F. Statins: The new aspirin? Cell Mol Life Sci 2002;59:1771-86. 13. Staffa JA, Chang J, Green L. Cerivastatin and reports of fatal rhabdomyolysis. N Eng J Med 2002;346:539-40. 14. ACC/AHA/NHLBI Clinical Advisory on Statins: clinical advisory on the use and safety of statins. JACC 2002;40:567-72. 15. Chong P, Seeger J, Franklin C. Clinically relevant differences between the statins: implications for the therapeutic selection. Am J Med 2001;111:390-400. 16. Chiang CE, Pella D, Singh RB. Coenzyme Q10 and adverse effects of statins. J Nutritional and Environmental Med 2004; 14:1-12. 17. Shepherd J. Fibrates and statins in the treatment of hyperlipidaemia: an appraisal of their efficacy and safety. Eur Heart J 1995; 16:5-13. 18. Mason RP, Jacob RF. Membrane microdomains and vascular biology: emerging role in atherogenesis. Circulation 2003; 107:2270-3. 19. McKenney JM, Jones PH, Adamczyk MA. For the STELLAR Study Group. Comparison of efficacy of rosuvastatin versus atorvastatin, simvastatin, and pravastatin in achieving lipid goals: results from the STELLAR trial. Curr Med Res Opin 2003; 19:557-66. 20. Law MR, Wald NJ, Rudnicka AR. Quantifying effect of statins on low-density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysis. BMJ 2003;326: 1423. 21. Schuster H, Fox JC. Investigating cardiovascular risk reduction: the Rosuvastatin GALAXY Programme. Expert Opin Pharmacother 2004;5:1187-1200. 22. Bevilacqua M, Guazzini B, Righini V, et al. Metabolic effects of fluvastatin extended release 80 mg and atorvastatin 20 mg in patients with type 2 diabetes mellitus and low serum high-density lipoprotein cholesterol levels: a 4-month, prospective, open label, randomised, blinded-end point (Probe) trial. Curr Ther Res 2004;65:330-44. 23. Olsson AG, Schwartz GG, Szarek M, et al. High-density lipoprotein, but not low-density lipoprotein cholesterol levels influence short-term prognosis after acute coronary syndrome: results from the MIRACL trial. Eur Heart J 2005;26:890-6. 24. Davignon J. The pleiotropic effects of drugs affecting lipid metabolism. Atherosclerosis XI. Paris: Elsevier, 1998;63-77. 25. Davignon J. Beneficial cardiovascular pleiotropic effects of statins. Circulation 2004;109(suppl III):III-39-III-43. 26. Schoenbeck U, Libby P. Inflammation, immunity, and HMGActa Cardiol Sin 2005;21:190-8 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 196 CoA reductase inhibitors: statins as antiinflammatory agents? Circulation 2004;109(suppl II):II-18-II-26. Schächinger V, Britten MB, Zeiher AM. Prognostic impact of coronary vasodilator dysfunction on adverse long-term outcome of coronary heart disease. Circulation 2000;101:1899-906. Gokce N, Keaney JF Jr, Hunter LM, et al. Risk stratification for postoperative cardiovascular events via noninvasive assessment of endothelial function: a prospective study. Circulation 2002; 105:1567-72. Marchesi S, Lupattelli G, Schillaci G, et al. Short-term atorvastatin treatment improves endothelial function in hypercholesterolemic women. J Cardiovasc Pharmacol 2000;36:617-21. Forgione MA, Leopold JA, Loscalzo J. Roles of endothelial dysfunction in coronary artery disease. Curr Opin Cardiol 2000;15:409-15. Lindahl B, Toss H, Siegbahn A, et al. Markers of myocardial damage and inflammation in relation to long-term mortality in unstable coronary artery disease. N Eng J Med 2000;343: 1139-47. Cannon CP, Braunwald E, McCabe CH, et al. Comparison of intensive and moderate lipid lowering with statins following acute coronary syndromes. N Eng J Med 2004;350:1495-504. Zwaka TP, Hombach V, Torzewski J. C-reactive protein-mediated low-density lipoprotein uptake by macrophages: implications for atherosclerosis. Circulation 2001;103:1194-7. Weissberg PL. Atherogenesis: current understanding of the causes of atheroma. Heart 2000;83:247-52. Nakagami H, Jensen KS, Liao JK. A novel pleiotropic effect of statins: prevention of cardiac hypertrophy by cholesterolindependent mechanisms. Ann Med 2003;35:398-403. Smilde TJ, van Wissen S, Wollersheim H, et al. Effect of aggressive versus conventional lipid lowering on atherosclerosis progression in familial hypercholesterolemia (ASAP): a prospective, randomised, double-blind trial. Lancet 2001; 357:577-81. Taylor AJ, Kent SM, Flaherty PJ, et al. ARBITER: Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol: a randomized trial comparing the effects of atorvastatin and pravastatin on carotid intima medial thickness. Circulation 2002;106:2055-60. Nissen SE, Tuzcu EM, Schoenhagen P, et al. REVERSAL investigators. Effect of intensive? compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. JAMA 2004;291:1071-80. Kaski JC. Infection, endothelial dysfunction, and atherogenesis. Circulation 2003;108:E171-2. Callahan AS 3rd. Vascular pleiotropy of statins: clinical evidence and biochemical mechanisms. Curr Atheroscler Rep 2003;5: 33-7. Borghi C, Dormi A, Veronesi M, et al. Association between different lipid-lowering treatment strategies and blood pressure control in the Brisighella Heart Study. Am Heart J 2004; 148:285-92. Pleiotropic Effects of Statins 42. Levy Y. Beyond cholesterol lowering: effect of statins on markers of cardiovascular disease. Isr Med Assoc J 2004;6:490-1. 43. Crisby M, Nordin-Fredriksson G, Shah PK, et al. Pravastatin treatment increases collagen content and decreases lipid content, inflammation, metalloproteinases, and cell death in human carotid plaques: implications for plaque stabilization. Circulation 2001;103:926-33. 44. Singh, RB, Pella D, Chopra BP, et al. Overview of ubiquinone, in memory of a champion, Dr. Emile G. Bliznakov. J of Nutr and Enviroment Med 2003;13:211-4. 45. Yusuf S. Two decades of progress in preventing vascular disease. Lancet 2002;6:2-3. 46. Pella D, Singh RB, Tomlinson B, et al. Coronary artery disease in developing and newly industrialised countries: a scientific statement of the International College of Cardiology. In: Frontiers in Cardiovascular Health. Boston: Kluwer Academic Publishers, 2003:473-87. 47. Moosmann B, Behl C. Selenoprotein synthesis and side effects of statins. Lancet 2004;363:892-4. 48. Silver MA, Langsjoen PH, Szabo S, et al. Effect of atorvastatin on left ventricular diastolic function and ability of coenzyme Q10 to reverse that dysfunction. Amer J Cardiol 2004;94:1306-10. 49. Kumar A, Kaur H, Kumar S, et al. Atorvastatin alone/in combination with coenzyme Q10 in 103 cases of heart failure due to ischemic cardiomyopathy. In: Abstract book from the Fourth Conference of the International Coenzyme Q10 Association. Los Angeles 2005:54-6. 50. Nash DB, Nash SA. Reclassification of simvastatin to overthe-counter status in the United Kingdom: a primary prevention strategy. Am J Cardiol 2004;94:35F-39F. 51. Doggrell SA. New targets and new drugs down under in 2004. Drug News Perspect 2005;18:149-60. 197 Acta Cardiol Sin 2005;21:190-8 Review Article Acta Cardiol Sin 2005;21:190−8 高血脂治療藥物 STATIN 的多重作用 Daniel Pella Rafael Rybar Viola Mechirova 1st Internal Clinic, Faculty of Medicine PJ Safarik University Kosice, Slovakia 近十年來,對於改善血脂肪異常與預防缺血性心臟病之間的研究逐漸開展。對於建立 新的治療標的與研發新的高血脂治療藥物也拓展臨床治療的選擇。不論病人是否具有冠狀 動脈心臟病,STATIN 已成為降低血膽固醇值與心血管疾病併發症最主要及最有效的藥物。 最近研究指出,STATIN 在治療心血管疾病的好處,不僅僅只從降低血膽固醇值方面解 釋。一些改善血脂肪異常以外的效果,如抗發炎、抗增生及抗血栓效果,以及改善內皮細 胞功能等,也扮演部份角色,本文將對這些改善血脂肪異常外之多重作用 (extra-lipid pleiotropic effects) 作概略介紹。 關鍵詞:高血脂治療藥物、降血脂外多重作用、冠狀動脈心臟病。 198