Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
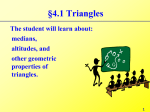
J Neuropathol Exp Neurol Copyright Ó 2010 by the American Association of Neuropathologists, Inc. Vol. 69, No. 8 August 2010 pp. 850Y863 ORIGINAL ARTICLE Early Progenitor Cell Marker Expression Distinguishes Type II From Type I Focal Cortical Dysplasias Ksenia A. Orlova, PhD, Victoria Tsai, MS, Marianna Baybis, MS, Gregory G. Heuer, MD, PhD, Sanjay Sisodiya, FRCP, PhD, Maria Thom, FRCPath, MD, Kevin Strauss, MD, Eleonora Aronica, MD, PhD, Phillip B. Storm, MD, and Peter B. Crino, MD, PhD Abstract Type I and type II focal cortical dysplasias (FCDs) exhibit distinct histopathologic features that suggest different pathogenic mechanisms. Type I FCDs are characterized by mild laminar disorganization and hypertrophic neurons, whereas type II FCDs exhibit dramatic laminar disorganization and cytomegalic cells (balloon cells). Both FCD types are associated with intractable epilepsy; therefore, identifying cellular or molecular differences between these lesion types that explains the histologic differences could provide new diagnostic and therapeutic insights. Type II FCDs express nestin, a neuroglial progenitor protein that is modulated in vitro by the stem cell proteins c-Myc, sexdetermining region Y-box 2 (SOX2), and Octamer-4 (Oct-4) after activation of mammalian target of rapamycin complex 1 (mTORC1). Because mTORC1 activation has been demonstrated in type II FCDs, we hypothesized that c-Myc, SOX2, and Oct-4 expression would distinguish type II from type I FCDs. In addition, we assayed the expression of progenitor cell proteins forkhead box G1 (FOXG1), Kruppel-like factor 4 (KLF4), Nanog, and SOX3. Differential expression of 7 stem cellproteins and aberrant phosphorylation of 2 mTORC1 substrates, S6 and S6 kinase 1 proteins, clearly distinguished type II from type I FCDs (n = 10 each). Our results demonstrate new potential pathogenic pathways in type II FCDs and suggest biomarkers for diagnostic pathology in resected epilepsy specimens. Key Words: Cortical dysplasia, Epilepsy, mTOR, STRAD>, Tuberous sclerosis complex. INTRODUCTION Focal cortical dysplasias (FCDs) are sporadic developmental malformations of the cortex that are the most common cause of intractable epilepsy in children (1Y3). Focal cortical From the PENN Epilepsy Center and Departments of Neurology (KAO, VT, MB, PBC) and Neurosurgery (GBH), University of Pennsylvania Medical Center, Philadelphia, Pennsylvania; Department of Clinical and Experimental Epilepsy (SS, MT), UCL Institute of Neurology, London, UK; The Clinic for Special Children (KS), Lancaster, Pennsylvania; Department of (Neuro)Pathology (EA), Academic Medical Center, University of Amsterdam, The Netherlands; Stichting Epilepsie Instellingen Nederland (EA), Heemstede, The Netherlands; and Department of Neurosurgery (PBS), Children Hospital of Philadelphia, Philadelphia, Pennsylvania. Send correspondence and reprint requests to: Peter B. Crino, MD, PhD, Department of Neurology, University of Pennsylvania, 3 W Gates Bldg, 3400 Spruce St, Philadelphia, PA 19104; E-mail: [email protected] This work was supported by grants NS045877 and NS045022, by the Department of Defense CDMRP TSC Initiative (P.B.C.), and by the National Epilepsy Fund (NEF 05-11) and Stichting Michelle (M06.011and M07 016; E.A.). 850 dysplasias have been classified histopathologically as either type I (subtype A or B), characterized by mild cortical disorganization and dyslamination and/or hypertrophic neurons, or type II, characterized by total loss of cortical lamination and the presence of cytomegalic-dysmorphic neurons (CDNs; type IIA) and/or balloon cells (BCs; type IIB) (2, 4). The histopathologic differences between type I and type II FCDs suggest that there are distinct mechanistic differences that lead to their formation, but the molecular pathogenesis of sporadic type I and type II FCDs has not been fully elucidated. Understanding the molecular mechanisms that underlie the histopathologic differences between type I and type II FCDs would provide important insights into diagnostic biomarkers and, potentially, new therapeutic strategies for patients with intractable epilepsy. The identification of 3 autosomal FCD subtypes associated with single gene defects provides insights into sporadic FCDs. For example, tubers in tuberous sclerosis complex (TSC) represent an autosomal dominant form of type IIB dysplasia resulting from mutations in TSC1 or TSC2 and are characterized by extensive laminar disorganization, CDNs, and the presence of BCs, also known as giant cells (GCs) in TSC (5). TSC1 or TSC2 gene mutations lead to constitutive activation of the mammalian target of rapamycin complex 1 (mTORC1) as evidenced by aberrant phosphorylation of several downstream signaling proteins including S6 kinase 1 (S6K1), ribosomal protein S6 (S6), and 4-elongation factor binding protein-1 (4E-BP1) in tubers (6Y8) (Fig. 1). The polyhydramnios, megalencephaly, symptomatic epilepsy syndrome (PS) is an autosomal recessive type II FCD characterized by cytomegalic cells and heterotopic cells in the subcortical white matter that results from a deletion in STRAD>, an upstream activator of the TSC1:TSC2 complex (9) (Fig. 1). Like TSC1 and TSC2, mutations in STRAD> also lead to hyperactivation of mTORC1 (9). Interestingly, enhanced phosphorylation of S6 protein is observed in sporadic type II FCDs and suggests that hyperactivated mTORC1 signaling may also be a pathogenic mechanism in this FCD subtype (10). In contrast, the cortical dysplasia focal epilepsy (CDFE) syndrome is a type I FCD that results from mutations in the contactin-associated protein-like 2 gene (CNTNAP2) encoding a scaffolding protein for the Kv1.1 channel, which has no known link to mTORC1 signaling (11). The pathway activation of mTORC1 has not been assessed in sporadic type I FCDs. Proteins that are typically expressed in neural progenitor cells (e.g. nestin, vimentin, CD133, and Mcm2) are found in J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 Early Progenitor Cell Markers in FCD Type II FIGURE 1. Schematic of mTORC1 signaling and genetic mutations at specific sites in the pathway. Cytoplasmic mTOR signaling is activated in normal cells by growth factors and nutrients. Loss-of-function mutations in either TSC1 or TSC2 lead to constitutive mTORC1 signaling and cause TSC. Loss-of-function deletions in STRAD> cause PS and result in hypoactivation of the TSC1:TSC2 complex and enhanced mTORC1 signaling. Hyperactive mTORC1 signaling results in enhanced S6K1 and S6 phosphorylation, leading to increased cell size, such as BCs and GCs. Mammalian target of rapamycin complex 1Ymediated inhibition of 4E-BP1 results in enhanced translation of c-Myc, which, in turn, translocates into the nucleus to regulate expression of Oct-4, SOX2, and nestin, perhaps conferring an immature cellular phenotype on many type II FCD cells. The molecular event causing sporadic FCD type II has yet to be identified, but the phenotypic and histologic similarities between sporadic FCD II, PS, and TSC suggest that sporadic FCD type II may be caused by dysfunction of an mTORC1 regulatory gene. GCs in TSC and CDNs and BCs in sporadic type II FCDs (12Y17) and may be linked to mTORC1 signaling (13, 18). Specifically, mTORC1 activation results in enhanced translation of the transcriptional activator c-Myc (19, 20). c-Myc is involved in the transcriptional regulation of certain stem cell marker proteins, such as sex-determining region Y-box 2 (SOX2) and Octamer-4 (Oct-4) (21). Sex-determining region Y-box 2 regulates nestin expression by binding to its enhancer domain (22), and sustained Oct-4 expression promotes differentiation of nestin-positive neural precursors (23). Moreover, the exogenous expression of c-Myc promotes proliferation of nestin-positive neural progenitor cells in vitro (24) and in vivo (25). Thus, we hypothesized that differential phosphorylation Ó 2010 American Association of Neuropathologists, Inc. of mTORC1 signaling proteins and expression of SOX2, Oct-4, and c-Myc could provide a mechanistic and pathophysiologic distinction between type II and type I FCDs. Furthermore, because expression of the stem cell proteins SOX2, Oct-4, and c-Myc could also suggest a phenotypic characteristic of GCs and BCs, we also examined 4 additional stem cell protein markers: the winged-helix transcription factor forkhead box G1 (FOXG1), Kruppel-like factor 4 (KLF4), Nanog, and sex-determining region Y-box 3 (SOX3). Our results demonstrate a clear distinction in stem cell protein expression and mTORC1 signaling between type I and type II FCDs that underscores the histologic differences between these dysplasia subtypes. 851 Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 Orlova et al MATERIALS AND METHODS TABLE 2. Clinical Features of Tuberous Sclerosis Complex Patients Human Tissue Specimens Sporadic type I and type II FCD specimens were obtained from 20 patients (type I: mean age, 7.8 years, 6 boys and 4 girls; type II: mean age, 5.5 years, 6 boys and 4 girls; Table 1) after epilepsy surgery at the Academic Medical Center, University of Amsterdam, the Netherlands; the Children’s Hospital of Philadelphia, Philadelphia, PA; or the National Hospital for Neurology and Neurosurgery, London, UK. Surgical localization of the resection site in all cases reflected the seizure focus as determined by standard presurgical evaluation including scalp or intracranial EEG monitoring. Tissue specimens were removed from frontal, temporal, or parietal lobes (Table 1). All patients exhibited Engel class I or II surgical outcomes (26). Type I FCD cases were defined histologically by cortical dyslamination and heterotopic neurons in layer I and the subcortical white matter. Type II FCD cases were defined by loss of cortical lamination, blurring of the gray-white junction and the presence of CDNs or BCs (1). Cortical dysplasia focal epilepsy syndrome specimens (n = 3; mean age, 4 years; 2 boys and 1 girl) were obtained after surgical resection (all 3 with Engel class II outcomes) and exhibited altered cortical lamination and heterotopic neurons similar to sporadic type I FCD. A single PS specimen from a 7-month-old female infant was available for analysis. This case exhibited aberrant cortical lamination, heterotopic neurons in the subcortical white matter and oval cytomegalic cells that were similar to those found in type II FCD. Cortical tubers were obtained from TSC patients (n = 8; mean age, 7.2 years; 4 boys and 4 girls; Table 2) with TSC defined by clinical criteria. Tubers exhibited loss of corTABLE 1. Clinical Features of FCD Patients Age at Surgery, Year/Sex 2/M 5/M 5/M 6/F 7/M 8/F 9/M 10/M 11/F 15/F 1/F 1/F 2/M 3/M 4/M 4/M 5/F 6/F 14/M 15/M Age at Seizure Onset Epilepsy Duration, Year FCD Type Location Engel Class* Birth 3 months 2 months 3 years Birth 1 year 1 year 3 years 4 years 2 years Birth Birth Birth Birth 3 months 3 months 2 years Birth Birth 1 year 2 5 5 3 7 7 8 7 7 13 1 1 2 3 4 4 3 6 14 14 IA IA IA IB IB IB IB IB IB IB IIA IIA IIA IIB IIB IIB IIB IIB IIB IIB Fr Fr T T T Fr Fr Fr T-P Fr Fr-P Fr P T-P T T Fr T Fr P I II II I II II I II II II I II I I I I II I I I *Engel et al (26). F, female; Fr, frontal lobe; M, male; P, parietal lobe; T, temporal lobe. 852 Age at Surgery, Years/Sex 2/M 4/M 8/M 9/M 4/F 7/F 14/F 10/F Age at Seizure Onset Epilepsy Duration, Years Location Engel Class Genotype Birth 2 years 2 years 5 years 3 months 1 year 4 years 2 years 2 2 6 4 4 6 10 8 Fr T T T Fr Fr Fr Fr I II II I II II II II TSC1 TSC2 TSC2 TSC2 TSC1 TSC2 TSC2 TSC2 TSC1 or TSC2, refers to clinical genetic testing results in these patients. tical lamination and contained CDNs and GCs consistent with type II FCD. In addition, 4 regions of nontuber cortex exhibiting normal histopathologic features were obtained postmortem from 4 TSC patients. There were 2 control patient tissue groups. First, specimens were obtained after focal cortical resection (n = 6; mean age, 7.2 years) for intractable seizures (Children’s Hospital of Philadelphia; Academic Medical Center, University of Amsterdam) from patients with no radiographic evidence of FCD or altered brain structure. Histologic analysis of these samples revealed intact cortical cytoarchitecture and no evidence of type I or II FCD. These samples did not differ in sex (n = 4 boys and 2 girls), age of seizure onset, duration of seizures, or numbers of antiepileptic drugs from the type I or type II FCD patients (Table 3) and were classified as Bepilepsy controls.[ Epilepsy control specimens were resected from frontal or temporal neocortices, and all resulted in Engel class I or II outcome. The second control group consisted of frontal and temporal neocortex specimens obtained from 6 patients at necropsy who died of nonneurologic causes (mean age, 5.8 years; 3 boys and 3 girls; Brain and Tissue Bank for Developmental Disorders, University of Maryland; Children’s Hospital of Philadelphia; mean postmortem interval, 14 hours; range, 11Y16 hours). Seizures were not terminal events in these patients, and none had a personal or family history of epilepsy. The cortical cytoarchitecture of these specimens was intact; these cases were classified as Bpostmortem controls.[ All human tissues were obtained in accordance with the protocols approved by the Academic Medical Center, University of Amsterdam, the Joint Research Ethics Committee TABLE 3. Comparison of FCD, Epilepsy Control, and Postmortem Control Samples Age (surgery) Seizure duration Age at onset AEDs used FCD Epilepsy Postmortem Significance (t Test) 6.6 5.3 10.7 4 7.2 4.6 8.9 4 5.8 (at death) NA NA NA NS NS NS NS Mean age at surgery or death is in years, mean seizure duration is in years; mean age at seizure onset is in months, and AEDs indicate mean number of antiepileptic drugs used. NA, not applicable; NS, nonsignificant (p 9 0.05, Student t-test). Ó 2010 American Association of Neuropathologists, Inc. Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 of the National Hospital for Neurology and Neurosurgery and Institute of Neurology, Children’s Hospital of Philadelphia, and the University of Pennsylvania Institutional Review Board and Committee on Human Research. Human Cell Culture In 1 FCD IIB specimen (14-year-old adolescent boy; Table 1), a portion of the resected tissue was used to generate dissociated cultures immediately after surgical removal. The tissue was digested in 0.25% Trypsin-EDTA (Gibco, Invitrogen, Carlsbad, CA) at 37-C for 20 minutes, triturated with flameconstricted glass pipettes, and plated on poly-L-lysineYcoated coverslips. Cells were cultured in 1 of 3 types of media: 1) Dulbecco modified Eagle medium/F12, 1% N2, 1% fetal bovine serum (FBS), 1% penicillin/streptomycin; 2) Dulbecco modified Eagle medium, 10% FBS, 1% P/S; or 3) Neurobasal, 5% FBS, 2% B-27 supplement, 2 mM GlutaMAX-I Supplement (Gibco). Cells were maintained at 37-C, pH 7.4, and analyzed after 24 and 72 hours in vitro. Genotype Analysis Genomic DNA was extracted (Qiagen, Valencia, CA) from all TSC and type I and type II FCD specimens. Exonspecific flanking polymerase chain reaction (PCR) primers (forward and reverse) were generated to TSC1 and TSC2, and amplicons from all exons were sequenced (ABI Prism, Invitrogen). All PCR and sequencing reactions were performed in duplicate. Sequence results were compared with existing database sequence for TSC1 and TSC2 (http://chromium.liacs.nl/ lovd/index.php?select_db=TSC1 or http://chromium.liacs.nl/ lovd/index.php?select_db=TSC2). Genotype analysis revealed that 2 TSC cases were associated with TSC1 mutations and that 6 cases were associated with TSC2 mutations. These findings corroborated the mutations identified by available clinical testing for 5 TSC patients. Genotype analysis in the 4 postmortem TSC specimens revealed 1 TSC1 and 3 TSC2 mutations. Previous studies identified a 5-exon terminal deletion in the STRAD> gene in all PS patients, including the patient in our sample (11). Published sequence analysis of CNTNAP2 in the 3 patients with CDFE revealed a single-base deletion at nucleotide 3709 (coding sequence 3709delG) in exon 22, resulting in a frameshift mutation and a premature stop codon (10). Tissue Processing, Immunohistochemistry, and Immunocytochemistry All tissue specimens were placed in 4% paraformaldehyde fixative for a defined period (based on the size of the tissue block) and were then embedded in paraffin. Portions of several specimens were rapidly frozen on dry ice for Western analysis. Paraffin-embedded blocks were sectioned at 7 mm; 5 representative sections per case were incubated overnight at 4-C with antibodies to c-Myc (mouse monoclonal, 1:250; Abcam, Cambridge, MA), FOXG1 (rabbit polyclonal, 1:500; Abcam), KLF4 (rabbit polyclonal, 1:25; Abgent, San Diego, CA), Nanog (mouse polyclonal, 1:100; Cosmo Bio Company, Tokyo, Japan), nestin (mouse monoclonal, 1:200; Chemicon, Temecula, CA), Oct-4 (rabbit polyclonal, 1:200; Chemicon), phospho-S6K1 (Thr389; rabbit monoclonal, 1:50; Novus Biologicals, Littleton, CO), phosphoÓ 2010 American Association of Neuropathologists, Inc. Early Progenitor Cell Markers in FCD Type II S6 (Ser235/236; rabbit polyclonal, 1:50; Bethyl Laboratories, Montgomery, TX), SOX2 (rabbit polyclonal, 1:100; Abcam), and SOX3 (rabbit polyclonal, 1:100; Chemicon). Sections were then probed with biotinylated secondary antibodies for 1 hour at room temperature and visualized using avidin-biotin conjugation (Vectastain ABC Elite; Vector Labs, Burlingame, CA) with 3,3¶-diaminobenzidine. Dehydrated sections were mounted with coverslips (Permount, Fischer Scientific, Pittsburgh, PA). Light microscopy images were acquired using a microscope (DM4000 B; Leica, Wetzlar, Germany). All immunohistochemistry (IHC) analyses were performed using batch processing for each antibody. Cells cultured from FCD IIB were fixed with 4% paraformaldehyde for 15 minutes after 1 day or 3 days of growth, were permeabilized in 0.3% Triton X-100, and were blocked in 2.5% normal goat serum and 2.5% normal horse serum for 4 hours at room temperature. Cells were probed with the following primary antibodies overnight: A-III tubulin (mouse monoclonal, 1:500; Abcam), microtubule-associated protein 2 (MAP2; mouse monoclonal, 1:500; Abcam), nestin (mouse monoclonal, 1:200; Abcam), and phospho-S6 (Ser235/236; rabbit monoclonal, 1:100; Cell Signaling Technology, Danvers, MA). Cells were then incubated in secondary antibodies, Texas Red goat anti-rabbit (Vector Labs) or fluorescein horse anti-mouse (Vector Labs) for 2 hours and costained with Hoechst 33342 (0.0001 Kg/KL; Invitrogen). Coverslips were mounted on microscope slides (Fluoromount-G, Southern Biotech, Birmingham, AL), and images were acquired using a microscope (DM4000; Leica) with a monochrome digital camera (DFC340 FX; Leica). Cell Counts Quantitative cell counts of SOX2-, Oct-4Y, and c-MycY immunolabeled cells in postmortem control, epilepsy control, sporadic type I FCD, and sporadic type II FCD tissue specimens were performed as previously described (27). A 1-cm2 region of interest (ROI) was identified in each tissue section (n = 3 sections per case) that extended from the pial surface to the edge of the resection margin and to the subcortical white matter and exhibited representative histologic features of each control or FCD type. Cells were analyzed under light microscopy (20 magnification) from each section using image acquisition and analysis software (Spot RT CCD camera [Diagnostic Instruments, Inc, Sterling Heights, MI] and Phase 3 Imaging System integrated with Image Pro Plus [Media Cybernetics, Silver Spring, MD]). All immunoreactive cells were counted in these specimens. In addition, the BCs in sporadic FCD IIB that expressed each of the progenitor cell protein markers were counted. BCs were identified by morphologic parameters. For all counts, each ROI was visually inspected and any cellular elements (e.g. blood vessels) erroneously included in the computerized count analysis were deleted. Western Analysis Frozen control (n = 3 epilepsy and n = 3 postmortem) and FCD (n = 6) tissue samples were thawed on ice in radioimmunoprecipitation assay lysis buffer containing protease and phosphatase inhibitors. Whole tissue lysates were prepared by continual passage through an 18-g 1.5-in needle 853 Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. Orlova et al using a 1-mL syringe followed by multiple centrifugations at 12,000 rpm at 4-C, and the supernatant fractions were collected. Total protein concentrations were determined using the DC Protein Assay Kit (Bio-Rad, Foster City, CA). Aliquots of total protein (40Y50 mg) were combined with 4 reducing sample loading buffer and denatured at 95-C for 5 minutes. The samples were then subjected to electrophoresis on a 4% to 15% sodium dodecyl sulfateYpolyacrylamide gel electrophoresis and transferred onto polyvinylidene difluoride membranes at 4-C. Membranes were blocked in Tris-buffered saline (TBS), 0.1% Tween 20 (TBS-T), 5% nonfat dry milk for 1 hour and washed in TBS-T. The membranes were then probed with antibodies against c-Myc (mouse monoclonal, 1:750; Abcam), Oct-4 (rabbit polyclonal, 1 Kg/mL; Abcam), phospho-S6 (Ser235/ 236; rabbit polyclonal, 1:2000; Cell Signaling Technology), or SOX2 (rabbit polyclonal, 1:2000; Abcam) overnight at 4-C, washed 3 times in TBS-T, and incubated with a horseradish peroxidaseYconjugated anti-rabbit or anti-mouse secondary antibody (1:1500 to 1:3000; GE Healthcare, Piscataway, NJ) J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 for 1 hour. The ECL detection system (GE Healthcare) was used for immunodetection by exposing the membrane to a radiograph (Kodak, Rochester, NY). To ensure equal loading, membranes were subsequently stripped in Restore Western Blot Stripping Buffer (Thermo Scientific, Waltham, MA), blocked in TBS-T, 5% nonfat dry milk, subjected to Western blot analysis as described previously, probed with a horseradish peroxidaseYconjugated antibody against A-actin (mouse monoclonal, 1:5000; Abcam) or glyceraldehyde phosphate dehydrogenase (rabbit polyclonal, 1:5000; Cell Signaling Technology), and visualized using the ECL detection system (GE Healthcare). Single-Cell Microdissection, Messenger RNA Amplification, and Reverse TranscriptionYPCR After SOX2 immunolabeling, sporadic FCD type II tissue sections were treated with Proteinase K (50 mg/mL) at 37-C for 30 minutes and then washed in diethylpyrocarbonate-treated water. Sections were processed for messenger RNA (mRNA) FIGURE 2. Hyperactive mTORC1 signaling and progenitor cell marker protein expression in rapidly processed, surgically resected type IIB FCD. (A) Axial FLAIR magnetic resonance image of a 14-year-old adolescent boy with intractable epilepsy demonstrating a cortical dysplasia extending from the right frontal horn of the lateral ventricle to the right frontal cortex (arrow). (B, C) Intraoperative photographs showing preoperative (B) and postoperative (C) images of the FCD depicted radiographically in (A). (DYI) Histology and immunohistochemistry of the resected FCD IIB demonstrating numerous BCs (arrowheads) and dysmorphic neurons (arrows) in a cresyl violetYstained section (D), enhanced immunoreactivity for mTORC1 signaling proteins phospho-p70S6Kinase (P-S6K1) (E), phospho-ribosomal S6 (P-S6) (F), and c-Myc (G), and expression of SOX2 (H) and nestin (I) by BCs and dysmorphic neurons (20 objective, scale bar = 50 Km). (JYR) Cells cultured from the resected FCD IIB specimen express MAP2 and A-III tubulin (K, N) and nestin (Q) and are highly immunoreactive for P-S6 (J, M, P). Cells were costained with Hoechst (L, O, R) to visualize the nuclei. Note the abnormal morphology of the cells and laterally displaced nuclei (L, O). Scale bar = 10 Km. (S, T) Representative Western blot analysis of whole tissue lysates from epilepsy control cortex (control no. 1), postmortem control cortex (control no. 2), and the FCD IIB specimen. Focal cortical dysplasia IIB demonstrates enhanced P-S6, Oct-4 (S), and SOX2 (T) expression versus the control samples. Glyceraldehyde phosphate dehydrogenase (GAPDH) served as an internal loading control. 854 Ó 2010 American Association of Neuropathologists, Inc. Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 amplification, beginning with in situ reverse transcription of cellular poly(A) mRNA into complementary DNA (cDNA) directly on the tissue section, as previously described (28). To initiate reverse transcription in situ, an oligo-dT primer coupled to a T7 RNA polymerase promoter (25,00 U/mL, 50,000 U; Epicentre Technologies, Madison, WI) was annealed to cellular Early Progenitor Cell Markers in FCD Type II poly(A) mRNA overnight at room temperature. Complementary DNA synthesis was then performed with avian myeloblastosis virus reverse transcriptase (0.5 U/mL; Seikagaku America, Chiyoda-Ku, Japan). Thereafter, sections were washed in 0.5 saline-sodium citrate buffer and were placed in RNAsefree water. FIGURE 3. Sex-determining region Y-box 2 is expressed in PS, type II FCD, and TSC but not in control, type I FCD, or CDFE cortex. (AYF) SOX2 expression detected by immunohistochemistry in neocortical brain tissue samples (large panel photos: 5 objective, bar = 200 Km; inset photos: 40 objective, bar = 50 Km). The expression of SOX2 is virtually absent in control (A), type I FCD (B), and CDFE2 (C) cases and abundant in PS (D), type II FCD (E), and TSC (F). Bottom left: Western blot analysis of SOX2 expression in tissue lysates from postmortem control cortex, FCD IIB, and 2 tuber specimens. Glyceraldehyde phosphate dehydrogenase served as an internal loading control. Bottom center: RT-PCR amplification of SOX2 transcripts (225-bp amplicon, arrow) from single microdissected SOX2+ BCs in 2 FCD IIB specimens but not a pyramidal neuron from postmortem control cortex. First lane is size marker. Bottom right: cell counts of SOX2+ cells in postmortem (PM) control, epilepsy (Epi) control, type I FCD, and type II FCD specimens. Counts reflect mean cell number across 3 ROIs per specimen; mean T SEM. *p G 0.05. Ó 2010 American Association of Neuropathologists, Inc. 855 Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. Orlova et al Single SOX2-labeled neurons were microdissected from 2 representative FCD (n = 10 cells) or from postmortem control cortex sections (n = 10 cells) under light microscopy using a J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 stainless steel microscalpel and a joystick micromanipulator. Single cells were aspirated into a pipette tip, transferred to a microfuge tube containing in situ reverse transcription buffer FIGURE 4. Octamer-4 is expressed in PS, type II FCD, and TSC but not in control, type I FCD, or CDFE cortex. Immunohistochemistry for Oct-4 expression in neocortical brain tissue samples (large panel photos: 5 objective, bar = 200 Km; inset photos: 40 objective, bar = 50 Km). Octamer-4 expression is virtually absent in postmortem control (A), type I FCD (B), and CDFE (C) cases and abundant in PS (D), type II FCD (E), and TSC (F). Bottom left: Western blot analysis of Oct-4 depicting enhanced expression in tissue lysates from FCD IIB and 2 tuber specimens compared with epilepsy control cortex (control no. 1) and postmortem control (control no. 2) cortex and type I FCD. Glyceraldehyde phosphate dehydrogenase served as an internal loading control. Bottom center: RT-PCR amplification of Oct-4 transcript (290-bp amplicon) from single microdissected SOX2immunoreactive BCs in an FCD IIB specimen but not a pyramidal neuron from postmortem control cortex. Bottom right: Cell counts of Oct-4+ cells in postmortem (PM) control, epilepsy (Epi) control, type I FCD, and type II FCD specimens. Counts reflect mean cell number across 3 ROIs per specimen; mean T SEM. *p G 0.05. 856 Ó 2010 American Association of Neuropathologists, Inc. Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 and avian myeloblastosis virus reverse transcriptase, and incubated at 4-C for 90 minutes to generate single-stranded cDNA. Double-stranded template cDNA was generated with T4 DNA polymerase I (Amersham, Piscataway, NJ) from cDNA. Specific primers recognizing SOX2 and Oct-4 transcripts were generated for reverse transcription (RT)YPCR. After PCR amplification, amplicons were resolved on a 1% Early Progenitor Cell Markers in FCD Type II agarose gel, and products were sequenced (ABI Prism) to confirm their identity. RESULTS Aberrant phosphorylation of S6K1 and S6 proteins and robust expression of all 7 stem cell marker proteins were observed in the type II but not type I FCD specimens. The FIGURE 5. c-Myc expression is prominent in PS, type II FCD, and TSC but not control, type I FCD, or CDFE cortex. c-Myc expression in neocortical brain tissue samples (large panel photos: 5 objective, bar = 200 Km; inset photos: 40 objective, bar = 50 Km). c-Myc immunoreactivity is virtually absent in control (A), type I FCD (B), and CDFE (C) cases and abundant in PS (D), type II FCD (E), and TSC (F). Bottom left: Western blot analysis of c-Myc showing enhanced expression in FCD IIB and tuber specimen compared with FCD I or postmortem control cortex. Bottom right: Cell counts of c-Myc+ cells in postmortem (PM) control, epilepsy (Epi) control, type I FCD, and type II FCD specimens. Counts reflect mean cell number across 3 ROIs per specimen; mean T SEM. *p G 0.05. Ó 2010 American Association of Neuropathologists, Inc. 857 Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. Orlova et al distribution of cells immunoreactive for each of the proteins assayed in type II FCDs was not uniform in each case and reflected the distribution of CDNs, BCs, or GCs. For example, in some specimens, CDNs, BCs, or GCs were observed throughout the thickness of the dysplasia (i.e. from white matter to pial surface), whereas in other cases, these cells were seen in deeper portions of the lesion. In general, there were many more BCs or GCs (and hence immunoreactive cells) in the deeper portions and white matter within the dysplasia than closer to the pial surface. Morphologically normal cortex at the edge of FCD type II or tuber resections that did not contain CDNs, BCs, or GCs did not exhibit immunoreactivity for any of the assayed proteins. Type II But Not Type I FCD Expresses Progenitor Cell Proteins We first analyzed mTORC1 signaling and progenitor cell proteins in an FCD IIB specimen rapidly processed from the operating room. Aberrantly enhanced phosphorylation of S6K1 and S6 proteins and robust c-Myc, SOX2, and nestin expression was detected by IHC and was corroborated by Western assay (Fig. 2). Several very large cultured neurons with a laterally displaced nucleus that were morphologically similar to CDNs in fixed FCD specimens coexpressed both phosphorylated S6 and nestin or phosphorylated S6 and A-III tubulin or MAP2 (14) (Fig. 2). We submit that the ultra rapid processing of the tissue for Western assay and IHC, as well as the detection of enhanced phospho-S6 in vitro, provide a view J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 of phospho-protein and progenitor cell protein expression that approximates the levels of these proteins in vivo. Because previous studies have identified robust nestin expression in BCs and GCs in FCD type II and TSC, respectively (13, 14, 29), we next investigated and compared the expression profile of SOX2 and Oct-4 (proteins that modulate nestin expression) in FCD type I and type II specimens (n = 10 of each type) by IHC and Western assay. The expression of SOX2 (Figs. 2 and 3) and Oct-4 (Figs. 2 and 4) were detected in all sporadic and syndromic type II FCDs and were largely confined to CDNs and BCs in FCD II or GCs in tubers. The subcellular distribution of SOX2 and Oct-4 immunoreactivity was both nuclear and cytoplasmic in sporadic FCD II or TSC, whereas it was largely nuclear in PS. In contrast, there was minimal expression of SOX2 or Oct-4 in sporadic type I FCD, CDFE specimens, nontuber cortex, or postmortem and epilepsy controls (Figs. 3 and 4). Western analysis demonstrated an increase in SOX2 and Oct-4 expression in tuber and FCD IIB specimens versus control samples. The 43- and 70-kd isoforms of Oct-4 were detected in tuber and FCD IIB but not in FCD type I or control cortex. To corroborate the IHC, single SOX2-labeled cells were microdissected from sporadic FCD IIB samples, and RT-PCR amplification of SOX2 and Oct-4 transcripts was performed. Amplicons of SOX2 and Oct-4 of appropriate sizes were detected in all dissected SOX2-labeled BCs, but not from control pyramidal neurons (Figs. 3 and 4), and were confirmed by cDNA sequencing. FIGURE 6. Immunolabeling of SOX3 (AYC) and KLF4 (DYF) in control (A, D), type II FCD (B, E), and TSC (C, F). Inset in (B) shows a higher-magnification image of SOX3 labeling. In (C), there are both SOX3-labeled (arrow) and unlabeled (arrowhead) cells. There is strong KLF4 labeling in type II FCD and tubers. The expression of SOX3 and KLF4 are absent in the control cortex. Bar = (A, B, D, F) 300 Km; (C) 100 Km. 858 Ó 2010 American Association of Neuropathologists, Inc. Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 Early Progenitor Cell Markers in FCD Type II FIGURE 7. Forkhead box G1 expression in control cortex, type I, and type II FCD. Expression is absent in control and type I FCD specimens versus strong protein immunoreactivity in type II FCD (large panel photos: 5 objective, bar = 200 Km; inset photos: 40 objective, bar = 50 Km). c-Myc was robustly expressed in all type II FCD specimens, and the IHC pattern closely paralleled that of SOX2 and Oct-4 expression (Figs. 2 and 5). Low to nearly absent levels of c-Myc expression were observed in sporadic type I FCD and CDFE specimens that did not differ from postmortem and epilepsy control specimens or nontuber TSC cortex. Enhanced c-Myc protein expression detected by IHC was confirmed by Western analysis (Fig. 5). Immunohistochemistry revealed that there was minimal expression of KLF4, FOXG1, SOX3, or Nanog in control specimens or in the sporadic or autosomal recessive type I FCD specimens. In contrast, expression of KLF4 (Fig. 6), SOX3 (Fig. 6), FOXG1 (Fig. 7), or Nanog (Fig. 8) proteins was detected in BCs in sporadic FCD type II and in GCs in all TSC tuber specimens. We were particularly interested in the numbers of BCs that expressed each progenitor cell protein marker and thus focused cell quantification on BCs within defined 1-cm2 ROIs for each FCD IIB case that extended from the pial surface to the edge of the resection margin and to the subcortical white matter (n = 3 sections per case). The mean maximal cell soma diameter of the BCs was 117.6 mm (range, 104Y125 mm), and FIGURE 8. Expression of Nanog in type II dysplasias. Nanog immunoreactivity is virtually absent in control (A), type I FCD (B), and CDFE (C) cases and abundant in polyhydramnios, megalencephaly, PS (D), type II FCD (E), and TSC (F) (large panel photos, 5 objective; bar = 200 Km; inset photos, 40 objective; bar = 50 Km). Ó 2010 American Association of Neuropathologists, Inc. 859 Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. Orlova et al J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 FIGURE 9. Mammalian target of rapamycin complex 1 activation distinguishes type I from type II FCD as evidenced by enhanced immunoreactivity for phospho-p70S6Kinase (P-S6K1; Thr389) and phospho-ribosomal S6 (P-S6; Ser235/236) in the latter. (AYH) Aberrant phosphorylation of S6K1 is prominent in PS (D), type II FCD (E), and TSC (F) but is virtually absent in postmortem control (A), type I FCD (B), and CDFE (C) samples. Hyperphosphorylation of the S6K1 target S6 is evident in PS (J), type II FCD (K), and TSC (L) but is virtually absent in control (G), type I FCD (H), and CDFE (I) samples (20 objective, bar = 50 Km). Bottom left: Western blot analysis shows enhanced S6 protein phosphorylation in FCD IIB and 3 tuber specimens versus FCD I, epilepsy control cortex (control no. 1), and postmortem control cortex (control no. 2). Bottom right: Percent of morphologically defined BCs in sporadic type IIB FCD expressing each stem cell marker protein (TSEM). this parameter was used to generate cell counts for each individual protein marker. Across the FCD IIB specimens, 93% of cells meeting morphologic criteria for BCs expressed SOX2, 89% expressed c-Myc, 86% expressed FOXG1, 82% expressed SOX3, 77% expressed KLF4, 61% expressed Oct-4, and 37% expressed Nanog (Fig. 9). Type II But Not Type I FCD Exhibits mTORC1 Activation The expression of progenitor cell protein markers distinguished type I and type II FCDs. Because expression of c-Myc, SOX2, and Oct4 have been linked to mTORC1 signaling, we investigated whether aberrant phosphorylation of downstream proteins such as S6K1 and S6 could also delineate these subtypes. There was a clear difference in phosphorylation of S6K1 and S6 between type I and type II FCDs (Fig. 9). More than 90% of BCs in sporadic type II FCDs or GCs in tubers exhibited enhanced S6 and S6K1 phosphorylation, in accordance with previous studies (9, 29, 30). In addition, phospho-S6 and phospho-S6K1 immunoreactivity was detected 860 in PS brain tissue (9). Aberrant S6K1 and S6 protein phosphorylation was not detected in sporadic or autosomal recessive (CDFE) type I FCD or in control specimens (Fig. 9). Greater S6 phosphorylation was identified by Western assay in FCD type IIB and 3 tuber specimens than in controls and sporadic type I FCD (Fig. 9). Another activated kinase, phosphorylated p90RSK (Ser380), is known to phosphorylate S6 in an mTORC1-independent fashion. There was no difference in TABLE 4. Representative TSC1 and TSC2 Polymorphisms in Sporadic Type I FCD Exon TSC1 14 TSC1 14 TSC1 17 TSC2 12 TSC2 17 Base Change Amino Acid Change SNP Type C9T A9G C9T C9T G9A H9Y G9G L9L F9F V9V NS S S S S NS, nonsynonymous; S, synonymous; SNP, single nucleotide polymorphism. Ó 2010 American Association of Neuropathologists, Inc. Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 phospho-p90RSK (Ser380) immunoreactivity in type I FCD, type II FCD, or control specimens (data not shown). Genotype Analysis of Type I and Type II FCDs Genotype analysis of TSC1 and TSC2 in the 20 sporadic FCD type I and type II cases did not reveal mutations in either gene, thereby confirming that these dysplasias did not represent somatic mosaic forms of TSC (28). However, sequencing was confined to exons only; splice site mutations were not identified. Several single nucleotide polymorphisms previously identified in the TSC sequence database that are known to be present in normal individuals were found in type I FCD (Table 4). DISCUSSION We demonstrate that the expression of SOX2, Oct-4, c-Myc, FOXG1, KLF4, Nanog, and SOX3, as well as those of hyperphosphorylated S6K1 and S6 proteins, distinguish sporadic, autosomal dominant (TSC), and autosomal recessive (PS) forms of type II FCD from sporadic or autosomal recessive (CDFE) forms of type I FCD or control cortex. Sexdetermining regions Y-box 2 and 3 are markers for multipotent neural stem cells, and FOXG1 is a known repressor of differentiation in neural progenitor cells, whereas c-Myc, KLF4, Oct-4, and Nanog are typically identified in pluripotent stem cells (31). Thus, these results suggest that BCs and GCs exhibit a protein expression phenotype similar to multipotent or pluripotent stem cells. The concomitant aberrant phosphorylation of S6K1 and S6 proteins (known downstream effectors of mTORC1 signaling in type II but not type I dysplasias) mirrors the expression profiles of the 7 stem cell proteins. This suggests that hyperactive mTORC1 signaling may be linked to a progenitor cell phenotype in type II FCD and highlights a mechanistic distinction between type I and type II FCDs. There are several caveats to the interpretation of our results. First, although the generation of dissociated cultures from 1 case of type II FCD provides a compelling novel strategy to study FCD in vitro, further work is necessary to define the phenotype of these cells. The experiments in the dissociated cultures were designed to demonstrate colocalization of nestin and phospho-S6 in live cells and to show the feasibility of cell culture from resected FCD specimens. Nestin, c-Myc, SOX2, and Oct-4 expression as well as phosphorylation of S6K1 and S6 were corroborated in this same sample by IHC and Western assay. Second, in view of the rarity of PS, only a single case specimen was available for analysis. However, because of the direct link between STRAD> and mTORC1 signaling via the TSC1:TSC2 complex (11), we suggest that the findings in the PS case support our hypothesis that hyperactive mTORC1 signaling is a central feature of type II FCD. Third, it is unlikely that seizures or antiepileptic drug exposure alone accounted for altered protein expression; for example, c-Myc, SOX2, and Oct-4 were not detected in our epilepsy control group or in the nontuber cortex of TSC patients. We previously reported minimal S6K1 phosphorylation in type II FCD (29), but we now revise these observations using a different antibody to phospho-S6K1 that has given us more reproducible results (P. Crino, unpublished obÓ 2010 American Association of Neuropathologists, Inc. Early Progenitor Cell Markers in FCD Type II servations). Indeed, other investigators have demonstrated aberrant phosphorylation of S6K1 as well as of eIFG4 in FCD IIB (10, 30, 32). The absence of immunoreactivity of phosphop90RSK (Ser308), another kinase that phosphorylates S6 on Ser235/236 in an mTORC1-independent fashion, in any of the dysplasia specimens lends support to the notion that enhanced S6 phosphorylation specifically reflects mTORC1 activation. Finally, the expression of progenitor cell marker proteins in FCD type II may not demarcate a specific cell differentiation state but instead may reflect aberrant gene transcription or protein translation as a consequence of the profound abnormality of cortical lamination in type II FCD. Our findings have implications for diagnostic pathology and clinical outcome after surgical resection of FCDs, since a clear designation as type I or type II FCD may pose a challenge, especially in the absence of BCs. The distinction between type I and type II FCD based on both histology and signal cascade activation may help to stratify patients and to identify FCD subtypes with greater accuracy. Although larger cohorts will be needed to determine the functional diagnostic sensitivity and specificity of these marker proteins, our findings coupled with those of other investigators (10, 12Y16, 32, 33) suggest that probing resected tissue with a panel of antibodies (e.g. phospho-S6K1, phospho-S6, nestin, c-Myc, FOXG1, KLF4, Oct-4, SOX2, and SOX3) might enhance detection and diagnostic accuracy of FCDs. Furthermore, in some recent studies, tissue resected from patients with normal preoperative magnetic resonance images (so-called nonlesional cases) was found to contain type I or type II FCD (34). Thus, the expression of mTORC1 signaling or progenitor cell proteins may enhance detection of small or radiographically occult sporadic type II FCDs. Finally, in a recent comprehensive review of surgical treatment of FCDs (35), it was observed that complete resection is the most consistent predictor of seizure freedom after epilepsy surgery for type I and type II FCD. Because the edge of the surgical margin is currently defined on morphologic grounds alone, clear definition of the resection edge using mTORC1 signaling proteins as biomarkers may aid in defining the extent of FCD type II. Further experiments will be needed to determine whether BCs and GCs are stem cells; the ability to maintain FCD IIB cells in culture supports the feasibility of this approach. Our findings are bolstered by literature that shows expression of other progenitor cell markers such as vimentin, CD133, and Mcm2 in type II FCD (12Y17). Although nestin, vimentin, Mcm2, CD133, c-Myc, FOXG1, KLF4, Nanog, Oct-4, SOX2, and SOX3 expression may reflect a stem cell phenotype, the true definition of stem cells will require further in vitro studies that demonstrate the capacity of these cells for self-renewal as well as the ability to differentiate into neuroglial (i.e. neurons, astrocytes, and oligodendrocytes) or other cell lineages. One compelling observation was that many more BCs or GCs in the subcortical white matter expressed the 7 progenitor cell proteins and that there seemed to be a labeling gradient between deep and more superficial portions. Conceivably, it may indicate that there are different pools of cells within the lesion or that some BCs or GCs undergo further differentiation and cease to express these protein markers. 861 Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 Orlova et al The detection of SOX2 and Oct-4 in BCs and GCs provides clues to expression of other progenitor cell markers (e.g. nestin and vimentin) that are also found in BCs and GCs (13, 14, 17, 33). Sex-determining regions Y-box 2 regulates nestin expression by binding to the neural enhancer of nestin during different stages of differentiation (23, 36) and occupies the vimentin promoter and enhances vimentin expression (36). Sustained Oct-4 expression promotes differentiation and proliferation of nestin+ progenitor cells (36). Thus, the strong expression of SOX2 and Oct-4 in type II FCDs suggests 2 potential transcription factors that may account for nestin expression in this dysplasia subtype. The expression of SOX2 and Oct-4 are directly modulated by mTORC1 activation via c-Myc, the translation of which is controlled by 4E-BP1/eIF-4E in an mTORC1-dependent manner (Fig. 1) (21, 22). Exogenous expression of c-Myc in glial fibrillary acidic proteinYpositive astrocytes has been shown to promote an undifferentiated phenotype, characterized by nestin and vimentin expression (22). Interestingly, KLF4 has recently been shown to bind with SOX2 and Oct-4 to regulate Nanog expression in embryonic stem cells (37). Previous studies have demonstrated upstream activation of the mTORC1 pathway in type II FCD (10, 29, 30, 32). Our present data demonstrate that pathway activation is extended downstream to both transcriptional, as evidenced by SOX2 and Oct-4 expression, and translational, as evidenced by c-Myc expression, activations. Knockout of Tsc1 or Pten in the mouse leads to mTOR activation and models some of the features of type II FCD such as cytomegaly, laminar disorganization, and, clinically, spontaneous seizures (38, 39). In contrast, we find no evidence of mTORC1 cascade activation, either transcriptional or translational, in type I FCD. Indeed, we show for the first time that somatic mutations in TSC1 and TSC2 do not occur in FCD type I. These findings suggest that the molecular mechanisms leading to type I FCD formation during brain development are likely to be distinct from those in type II FCD and unrelated to mTORC1. ACKNOWLEDGMENTS The authors thank Ralph J. Monfort, Jia Yu, and Leah Marcotte for technical assistance. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. REFERENCES 1. Palmini A, Najm I, Avanzini G, et al. Terminology and classification of the cortical dysplasias. Neurology 2004;62:S2Y8 2. Krsek P, Maton B, Korman B, et al. Different features of histopathological subtypes of pediatric focal cortical dysplasia. Ann Neurol 2008; 63:758Y69 3. Fauser S, Huppertz HJ, Bast T, et al. Clinical characteristics in focal cortical dysplasia: A retrospective evaluation in a series of 120 patients. Brain 2006;129:1907Y16 4. Andre VM, Flores-Hernandez J, Cepeda C, et al. NMDA receptor alterations in neurons from pediatric cortical dysplasia tissue. Cereb Cortex 2004;14:634Y46 5. Crino PB, Nathanson KL, Henske EP. The tuberous sclerosis complex. N Engl J Med 2006;355:1345Y56 6. Inoki K, Zhu T, Guan KL. TSC2 mediates cellular energy response to control cell growth and survival. Cell 2003;115:577Y90 7. Goncharova EA, Goncharov DA, Eszterhas A, et al. Tuberin regulates p70 S6 kinase activation and ribosomal protein S6 phosphorylation. A 862 26. 27. 28. 29. 30. 31. role for the TSC2 tumor suppressor gene in pulmonary lymphangioleiomyomatosis (LAM). J Biol Chem 2002;277:30958Y67 Wullschleger S, Loewith R, Hall MN. TOR signaling in growth and metabolism. Cell 2006;124:471Y84 Puffenberger EG, Strauss KA, Ramsey KE, et al. Polyhydramnios, megalencephaly and symptomatic epilepsy caused by a homozygous 7-kilobase deletion in LYK5. Brain 2007;130:1929Y41 Schick V, Majores M, Koch A, et al. Alterations of phosphatidylinositol 3-kinase pathway components in epilepsy-associated glioneuronal lesions. Epilepsia 2007;48(suppl 5):65Y73 Strauss KA, Puffenberger EG, Huentelman MJ, et al. Recessive symptomatic focal epilepsy and mutant contactin-associated protein-like 2. N Engl J Med 2006;354:1370Y77 Taylor JP, Sater R, French J, et al. Transcription of intermediate filament genes is enhanced in focal cortical dysplasia. Acta Neuropathol 2001; 102:141Y48 Ying Z, Gonzalez-Martinez J, Tilelli C, et al. Expression of neural stem cell surface marker CD133 in balloon cells of human focal cortical dysplasia. Epilepsia 2005;46:1716Y23 Crino PB, Trojanowski JQ, Eberwine J. Internexin, MAP1B, and nestin in cortical dysplasia as markers of developmental maturity. Acta Neuropathol 1997;93:619Y27 Thom M, Martinian L, Sisodiya SM, et al. Mcm2 labelling of balloon cells in focal cortical dysplasia. Neuropathol Appl Neurobiol 2005; 31:580Y88 Mizuguchi M, Yamanouchi H, Becker LE, et al. Doublecortin immunoreactivity in giant cells of tuberous sclerosis and focal cortical dysplasia. Acta Neuropathol 2002;104:418Y24 Lamparello P, Baybis M, Pollard J, et al. Developmental lineage of cell types in cortical dysplasia with balloon cells. Brain 2007;130: 2267Y76 Hambardzumyan D, Becher OJ, Rosenblum MK, et al. PI3K pathway regulates survival of cancer stem cells residing in the perivascular niche following radiation in medulloblastoma in vivo. Genes Dev 2008; 22:436Y48 De Benedetti A, Graff JR. eIF-4E expression and its role in malignancies and metastases. Oncogene 2004;23:3189Y99 Kuang X, Shen J, Wong PK, Yan M. Deregulation of mTOR signaling is involved in thymic lymphoma development in Atmj/j mice. Biochem Biophys Res Commun 2009;383:368Y72 Kidder BL, Yang J, Palmer S. Stat3 and c-Myc genome-wide promoter occupancy in embryonic stem cells. PLoS One 2008;3:e3932 Jin Z, Liu L, Bian W, et al. Different transcription factors regulate nestin gene expression during P19 cell neural differentiation and central nervous system development. J Biol Chem 2009;284:8160Y73 Shimozaki K, Nakashima K, Niwa H, Taga T. Involvement of Oct3/4 in the enhancement of neuronal differentiation of ES cells in neurogenesis-inducing cultures. Development 2003;130:2505Y12 Lassman AB, Dai C, Fuller GN, et al. Overexpression of c-MYC promotes an undifferentiated phenotype in cultured astrocytes and allows elevated Ras and Akt signaling to induce gliomas from GFAP-expressing cells in mice. Neuron Glia Biol 2004;1:157Y63 Fults D, Pedone C, Dai C, Holland EC. MYC expression promotes the proliferation of neural progenitor cells in culture and in vivo. Neoplasia 2002;4:32Y39 Engel J, Van Ness PC, Rasmussen TB, et al. Outcome with respect to epileptic seizures. In: Engel J, ed. Surgical Treatment of the Epilepsies. New York, NY: Raven Press, 1993:609Y21 Kyin R, Hua Y, Baybis M, et al. Differential cellular expression of neurotrophins in cortical tubers of the tuberous sclerosis complex. Am J Pathol 2001;159:1541Y54 Becker AJ, Urbach H, Scheffler B, et al. Focal cortical dysplasia of Taylor’s balloon cell type: Mutational analysis of the TSC1 gene indicates a pathogenic relationship to tuberous sclerosis. Ann Neurol 2002; 52:29Y37 Baybis M, Yu J, Lee A, et al. mTOR cascade activation distinguishes tubers from focal cortical dysplasia. Ann Neurol 2004;56:478Y87 Miyata H, Chiang AC, Vinters HV. Insulin signaling pathways in cortical dysplasia and TSC-tubers: Tissue microarray analysis. Ann Neurol 2004; 56:510Y19 Boyer LA, Lee TI, Cole MF, et al. Core transcriptional regulatory circuitry in human embryonic stem cells. Cell 2005;122:947Y56 Ó 2010 American Association of Neuropathologists, Inc. Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited. J Neuropathol Exp Neurol Volume 69, Number 8, August 2010 32. Ljungberg MC, Bhattacharjee MB, Lu Y, et al. Activation of mammalian target of rapamycin in cytomegalic neurons of human cortical dysplasia. Ann Neurol 2006;60:420Y29 33. Crino PB, Trojanowski JQ, Dichter MA, Eberwine J. Embryonic neuronal markers in tuberous sclerosis: Single-cell molecular pathology. Proc Natl Acad Sci U S A 1996;93:14152Y57 34. Lee SK, Lee SY, Kim KK, et al. Surgical outcome and prognostic factors of cryptogenic neocortical epilepsy. Ann Neurol 2005;58:525Y32 35. Lerner JT, Salamon N, Hauptman JS, et al. Assessment and surgical outcomes for mild type I and severe type II cortical dysplasia: A critical review and the UCLA experience. Epilepsia 2009;50:1310Y35 Ó 2010 American Association of Neuropathologists, Inc. Early Progenitor Cell Markers in FCD Type II 36. Tanaka S, Kamachi Y, Tanouchi A, et al. Interplay of SOX and POU factors in regulation of the nestin gene in neural primordial cells. Mol Cell Biol 2004;24:8834Y46 37. Wei Z, Yang Y, Zhang P, et al. KLF4 interacts directly with Oct4 and Sox2 to promote reprogramming stem cells. Stem Cells 2009;27:2969Y78 38. Zeng LH, Xu L, Gutmann DH, Wong M. Rapamycin prevents epilepsy in a mouse model of tuberous sclerosis complex. Ann Neurol 2008;63: 444Y53 39. Kwon CH, Zhu X, Zhang J, Baker SJ. mTor is required for hypertrophy of Pten-deficient neuronal soma in vivo. Proc Natl Acad Sci U S A 2003; 100:12923Y28 863 Copyright @ 2010 by the American Association of Neuropathologists, Inc. Unauthorized reproduction of this article is prohibited.